
Abstract
Background:
Studies on the effect of weight on quality of life provide conflicting results. The purpose of the research was to assess the interconnection between the anthropometric variables and health-related quality of life (HRQoL) in a community-based sample of schoolchildren and to establish the role of body dissatisfaction (BD) in this association.
Methods:
A number of tenth-year schoolchildren (n = 413) completed a questionnaire making it possible to describe their sociodemographic and behavioral characteristics and assess body satisfaction and HRQoL (PedsQL 4.0, France). The hypothesis of BD as reflecting the relationship between anthropometric variables and HRQoL was tested using the logistic regression method.
Results:
No significant correlation was found between BMI and integral HRQoL scores. Waist circumference showed a significant negative correlation with the HRQoL scores in the girls, but not in the boys. The frequency of BD was 60.3% (n = 249). The relationship between BD and anthropometric variables proved to be differently directed in the boys and the girls. BD had a significant negative correlation with psychosocial and total HRQoL scores in adolescents of both sexes and with the girls’ physical functioning scores. The relationship between HRQoL and anthropometric indices in the girls, after making adjustment for sociodemographic, behavioral variables and BD in multivariate models, was no longer significant.
Conclusion:
This study has shown that BD is widespread among adolescents and has a significant impact on HRQoL. The impact of actual weight status on girls’ quality of life is entirely mediated by their dissatisfaction with their own bodies, thus justifying the approach to BD as a stand-alone problem having important psychosocial implications and requiring active identification and targeted intervention.
Introduction
Obesity in children and adolescents continues to be a global health problem. The prevalence of obesity remains consistently high in high-income countries, whereas it is increasing in low- and middle-income countries. If the current trends persist, then 254 million children and adolescents aged 5–19 will be obese by 2030. 1 In Russia, the primary incidence of obesity increased by 38.9% from 2012 to 2018 making a figure of 773 per 100,000 adolescents. The overall incidence of obesity increased by 50.1%, making a figure of 3523 per 100,000 adolescents. 2
Health-related quality of life (HRQoL) is a complex multidimensional construct that includes self-recognized physical, emotional, and social well-being. 3 Although many people do not perceive obesity as a disease, a number of both clinical and general community-based studies have reported impairment of various life-quality aspects in overweight and obese adolescents, compared with their normal-weight peers.4–7 However, other studies have not confirmed the impact of weight on the quality of life.8–9 The conflicting findings call for an in-depth investigation of the effect obesity may have on HRQoL in childhood and adolescence.
Previous research has shown that many factors can influence adolescents’ HRQoL, such as gender, age, socioeconomic, behavioral, racial and cultural factors.10–12 These factors can modulate the association between one’s weight and HRQoL. For instance, a stronger association between overweight/obesity and poor quality of life has been found in girls and adolescents. 6 It has also been shown that being overweight or obese can significantly reduce HRQoL in representatives of European ethnicity, but not in children of other races.6,8,13
There is evidence that adolescents’ HRQoL does not depend on actual body weight, but it depends on their perception of weight. In these terms, adolescents who are actually obese report better quality of life than those who perceive their weight as excessive. 14 Thus, one of the significant possible factors that can modulate the relationship between body weight and HRQoL is body dissatisfaction (BD) which characterizes a person’s subjective dissatisfaction with his/her body size or shape. 15
Given that adolescence is a critical period for the construction and formation of body image perception, it is important to understand better the possible impact of BD on one’s psychological domain at this stage of life. 16 This is especially true in light of the fact that BD has been reported to mediate the association between adolescent obesity and low self-esteem as well as depressed mood. 17 Considering the role of BD in mental well-being, it can be supposed that it may be a cause of poor HRQoL in adolescents with overweight and obesity.
The known studies of the relationship between weight and HRQoL tend to treat the above as separate categories. The studies presenting anthropometric characteristics as continuous variables traceable across a broad range of values are few. There are also few studies taking into account anthropometric indices other than the body mass index (BMI).
Thus, the aim of the present study was to assess the association between anthropometric variables and HRQoL in a community-based sample of schoolchildren of both sexes, and to ascertain the role that BD plays in this association.
Methods
The one-stage full-design survey was conducted between April 2017 and December 2018. It encompassed tenth-year schoolchildren from 14 high schools, with territorial coverage of all administrative districts of Irkutsk (Eastern Siberia, Russia).
Inclusion criteria: Tenth-graders of high schools; informed consent of the adolescent to participate in the study. Exclusion criteria: the presence of disease that could have an impact on the HRQoL of adolescents (e.g., cerebral palsy with severe motor impairments); the adolescent’s refusal to continue participation in the study at any stage.
After approval by the local ethics committee and obtaining permission to conduct the survey from the Education Department of the Social Policy and Culture Committee of Irkutsk City Administration, research team representatives met with the schoolchildren’s parents and provided comprehensive verbal and written information about the survey. On another day, the researchers met with the schoolchildren and, after presenting information about the survey, distributed informed voluntary consent forms that could be taken home by the students in order to make a joint family decision on participation. On subsequent days, the schoolchildren who returned completed consent forms underwent anthropometric measurement and questioning. All adolescents, with one exception, had reached the age of 15 years of age at the time of the study and independently signed consent. In one case, a 14-year-old boy signed the assent form, while the consent form was signed by his parents.
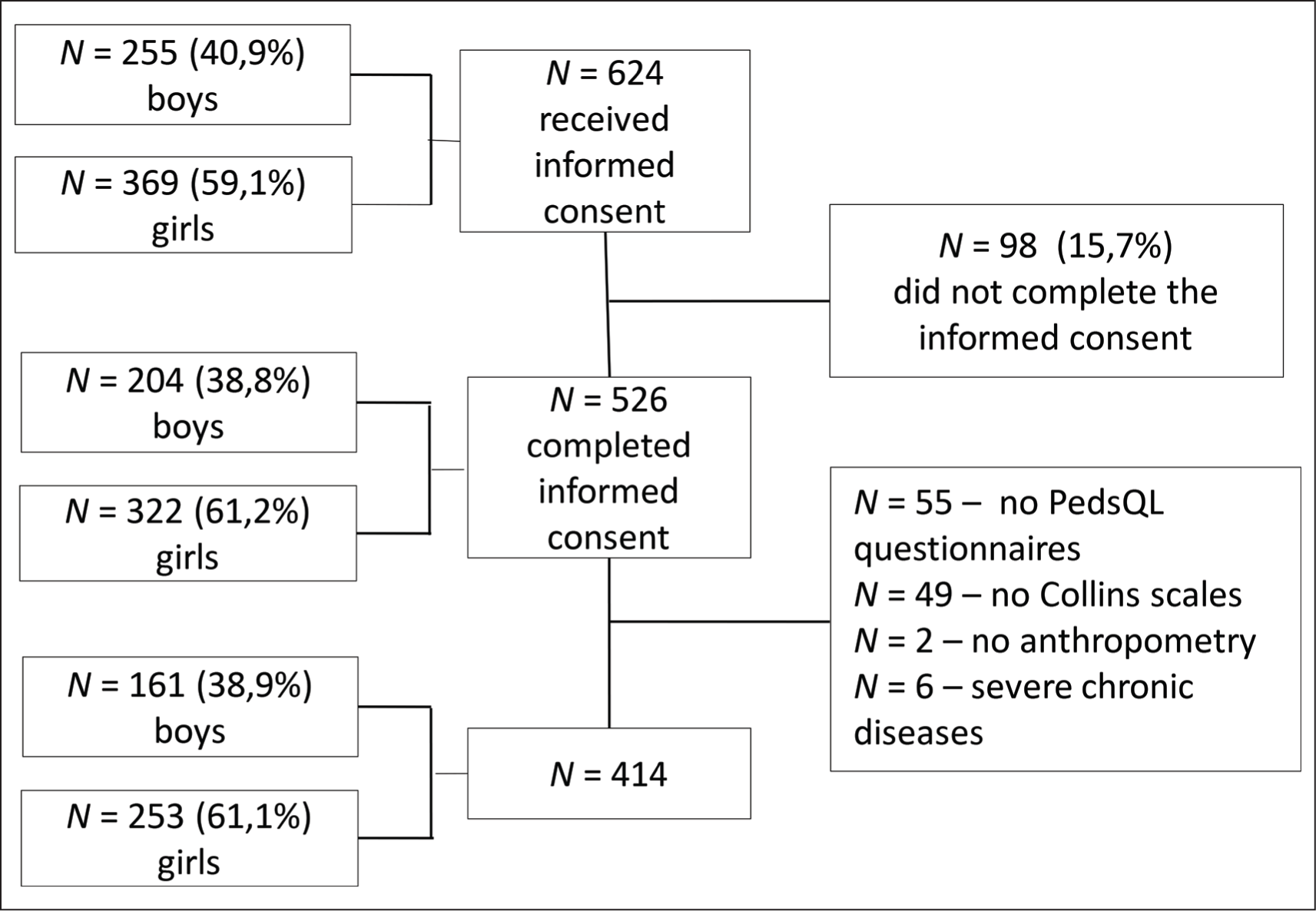
The sequence of forming a sample for inclusion in the study is shown in Figure 1. It should be noted that the BMI and BMI Z-score of adolescents that were included in the main study but who did not complete the Collins scales were statistically significantly higher than that in the formed sample (p = .01 and p = .012, respectively).
Graphic Representation of Study Sample Formation.
Self-reports from adolescents who completed the Russian version of the Pediatric Quality of Life Inventory (PedsQL 4.0, Lyon, France) for adolescents aged 13–18 were used to assess the HRQoL. PedsQL™ has a multidimensional structure and includes 23 questions split between Likert-type attitude scales assessing the domains of physical, emotional, social, and school functioning (PF, EF, SF, and ShF). The in-process score under each of the scales was then subjected to a recoding procedure to produce the actual life quality score ranked on a 100-point scale (0–100 points); the higher the score, the better the HRQoL. In addition, the psychosocial functioning (PSF) score (based on the score generated under EF, SF, and SF scales) and a total score (based on all scales) were calculated. The questionnaire showed acceptable reliability in this sample (Cronbach’s alpha for its subscales ranged from 0.73 to 0.80).
To assess body satisfaction, the child body silhouette diagrams proposed by Collins et al. were used. 18 They represent seven silhouettes of adolescent figures arranged in a row and vary from very thin to very fat. Each participant was asked to indicate which silhouette corresponded to their idea of an ideal body and which one corresponded to their actual perceived body size. The subtraction of the ideal body size from the perceived body size gave a BD score. Based on the absolute values of BD score differences, the participants were divided into groups: (a) those satisfied with their current body shape (|BD| = 0); (b) mildly dissatisfied with their current body shape (|BD| = 1); and (c) moderately or severely dissatisfied with their current body shape (|BD| > 1). The positive BD values correlated with the participant’s desire to be slimmer; the negative ones indicated the desire to gain weight.
The anthropometric measurements were taken in the morning; the adolescents wore light clothing and no shoes. The height and body weight were measured using a stadiometer and an electronic scale, respectively. BMI was calculated and processed using the AnthroPlus calculator (
Self-reported pubertal development data were also obtained using the Tanner scale of five stages of pubertal development.
Sociodemographic and Lifestyle Factors
All the adolescents completed the semi-structured questionnaires containing information on family composition, number of children in the family, birth order, age, education, parental employment, family income, and the adolescent’s self-assessment of housing conditions. The research team also received information about the adolescent’s extracurricular activities, the number of hours on weekdays and weekends spent watching TV, playing computer games, and at the screen for other purposes (social media, study courses); the distance to school; the total term spent outdoors during the day; time spent doing homework; smoking experience; and current smoking habits.
Statistical Procedures
The sample coverage for the study was calculated using the online calculator “RaoSoft” (
The statistical analysis was performed using the statistical software package IBM SPSS Statistics 26 (IBM Corp., Armonk, NY, USA). The distribution of continuous variables was checked for compliance with the normal probability law using Kolmogorov–Smirnov and Shapiro–Wilk test statistics. For non-normal distribution, continuous variables were presented as medians and 25th and 75th percentile values. The categorical variables were presented as absolute and relative values. The differences between independent groups of adolescents by continuous attributes were assessed using the Mann–Whitney test. When comparing the groups by the categorical attribute, the χ 2 test was used. In order to examine the relationship between continuous or ordinal attributes, the Spearman rank correlation coefficient was used.
The hypothesis of BD being mediated by the relationship between anthropometric variables and HRQoL was tested using the logistic regression method, on condition of the presence of statistically significant links: (a) anthropometric index with HRQoL; (b) anthropometric index with BD; and (c) BD with HRQoL. To reduce the number of statistical tests while maintaining the distinction between two HRQoL domains, the analysis was limited to the following integral characteristics: PF, PSF, and Total Score (TS), with the score dichotomized according to 25th percentile values. In the first stage, mono-factor analysis was applied to assess the correlation between the low HRQoL score (≤25th percentile) and dependent variables. The presence of a significant relationship between variables was determined in cases where a 95% CI, calculated for the obtained odds ratio (OR), did not contain one. The second step was to include the anthropometric variable in a multiple logistic regression model, along with the factors for which significant association was found with the dependent variable in one-dimensional models. The third step was the inclusion of a purported intermediary (BD) in the model. Complete mediation was reported if the established correlation between HRQoL and the anthropometric variable lost its significance completely, in cases when a mediator was introduced into the model. As far as significant gender differences were obtained, those involving two of the three variables of interest in the present study, the analysis in the boys and girls subgroups was carried out separately.
Results
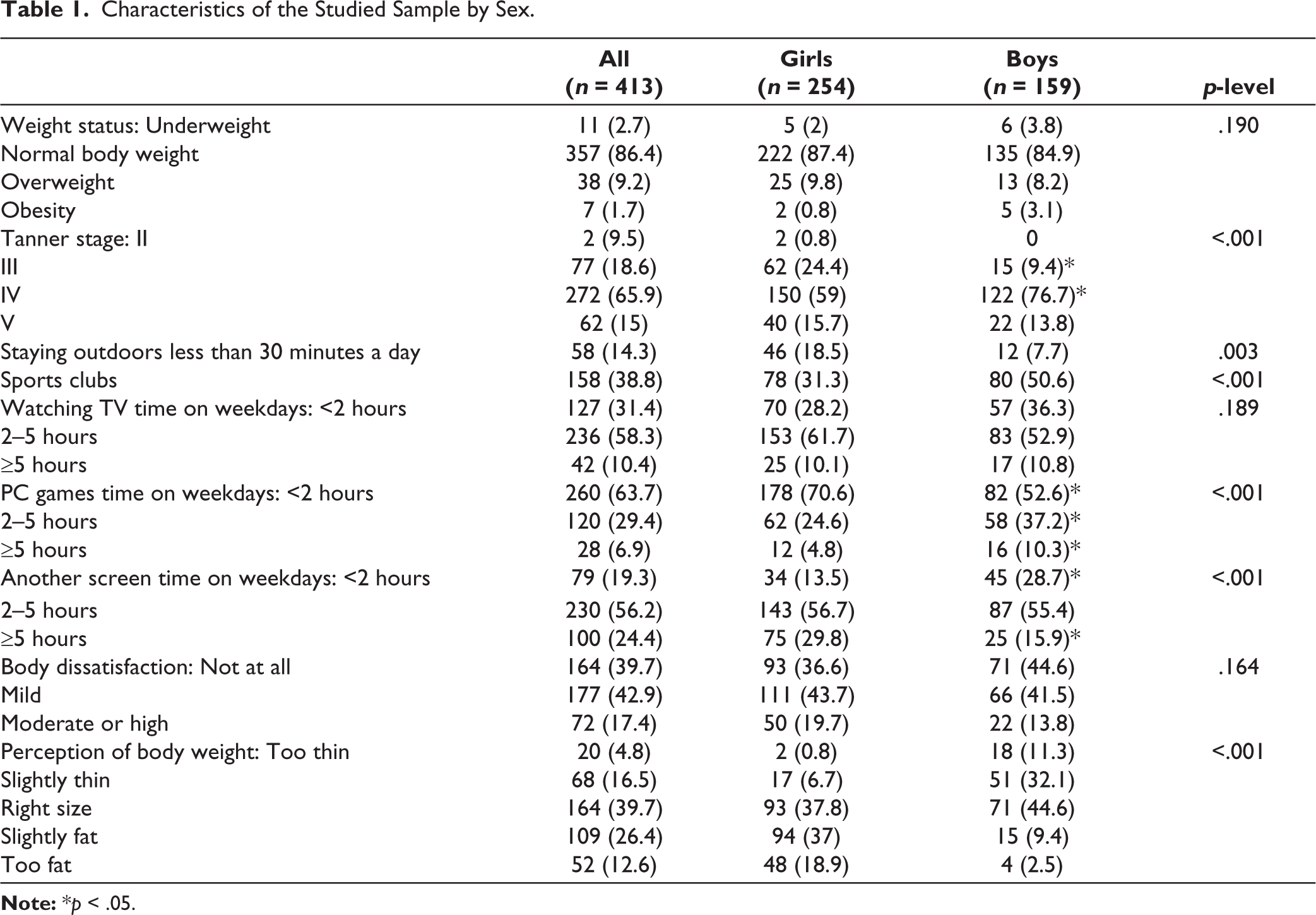
The study encompassed 413 adolescents aged 14–17 (80.6% aged 16); 160 (38.7%) boys and 253 (61.3%) girls. The comparative characteristics of the adolescents are presented in Table 1. It can be observed that the boys at the time of the study were at a higher stage of biological maturity than the girls, although the share of adolescents with Tanner stage V was comparable in both groups. The girls were less likely than the boys to participate in sports and spent less time outdoors. The boys and girls groups were characterized by adherence to different screen time modalities. The boys spent more time on computer games, while the girls predominantly spent more than five hours a day at computer/mobile screens for other purposes.
Characteristics of the Studied Sample by Sex.
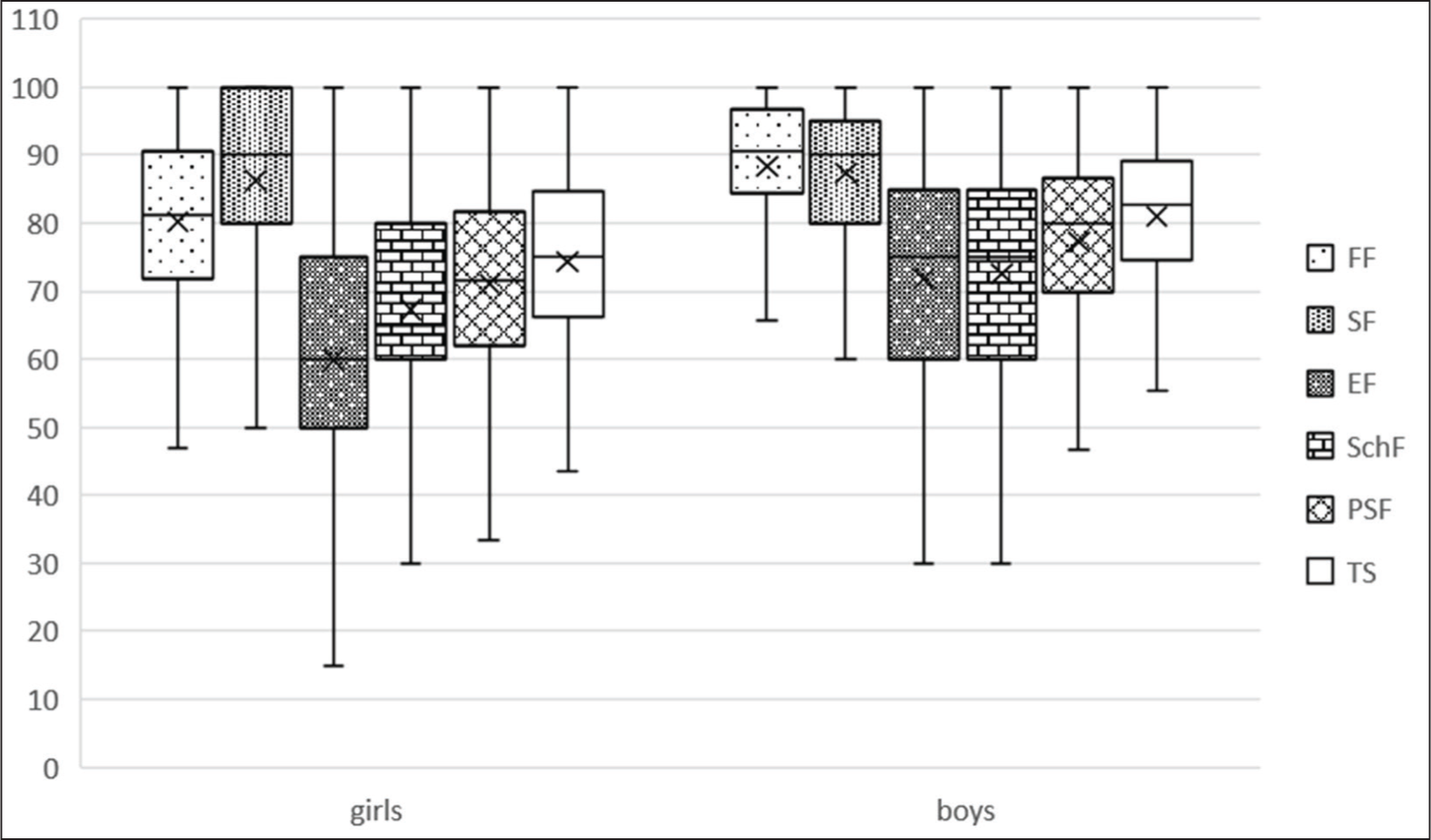
Statistically, the girls had a significantly lower score in all HRQoL domains except for SF, as compared to the boys (Figure 2). When examining the relationship between the HRQoL score and the adolescents’ anthropometric characteristics, it was found that the WC and WC/height index in the girls had a significant negative correlation with the HRQoL score in the SF and EF domains, as well as with the PSF and TS integral indicators score. A significant inverse correlation with the PF domain score was additionally presented for WC. As to the boys, the positive correlation between BMI (BMI Z-score) and HRQoL in terms of the ShF domain was the only one that reached the level of statistical significance (Table 2).
More than half (n = 249) (60.3%) of the schoolchildren were dissatisfied with their body shape. The share of adolescents dissatisfied with their silhouette, as well as the share of those with differing extents of dissatisfaction, was comparable in the subgroups of schoolchildren of both sexes. However, the correlation between BD and BMI Z-score was of a differently directed nature in the boys and girls groups. That is, the boys with lower body mass and the girls with overweight/obesity were more likely to be dissatisfied with their silhouette (Table 2). The association between the anthropometric parameters and BD was much more pronounced in the girls than in the boys (Z = 2.01, p = .022 for BMI Z-score, Z = 1.72, p = .043 for WC; Z = 2.4, p = .009 for WC/height).
The girls’ BD had a significant negative correlation with the HRQoL score in all domains and also with the integral indices scores (R = –0.23 for PF, R = –0.26 for PSF, R = –0.27 for TS, p < .001 for all). The correlation analysis showed a significant negative association between BD and the EF domain score in the boys (R = –0.29, p < .001), leading to a significant correlation between BD, on the one part, and the PSF and TS score, on the other part (R = –0.23, p = .004 and R = –0.2, p = .012, respectively).
Since no significant association between the anthropometric indices and HRQoL integral characteristic score was shown for the boys, the conditions for testing the mediation hypothesis were not met. Therefore, further analysis was performed only in the subgroup of girls.
The one-factor regression analysis performed for integral characteristics of HRQoL as dependent variables and aimed at the search for significant confounding factors revealed a significant association of low PF, PSF, and TS scores with the girls’ lowest self-rating as to their living conditions and time spent at the computer. The low PF and PSF domain scores had statistically significant negative association with participation in organized sports, as additionally shown. As to the PF and TS domain score, the association was found with the time spent on computer games; as concerns the PSF and TS domains—with the time spent in front of TV screens (Table 3).
Significant Correlations of Anthropometric Indices with HRQoL and BD.
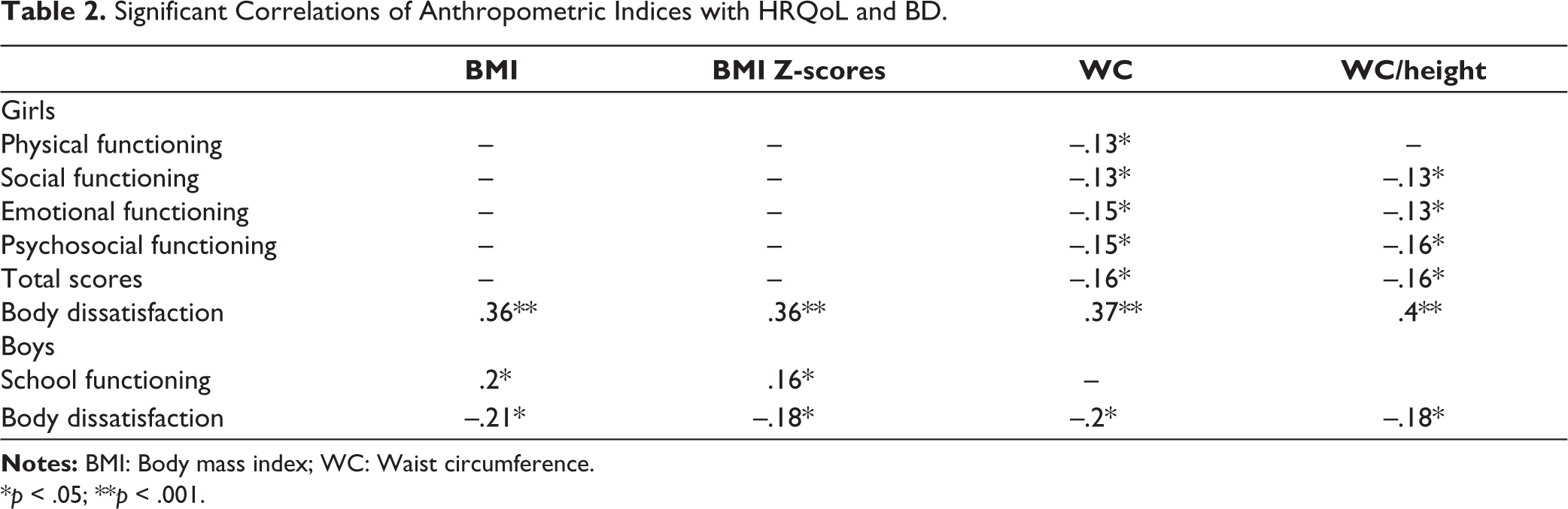
*p < .05; **p < .001.
Factors Associated with Low HRQoL Scores in Schoolgirls.
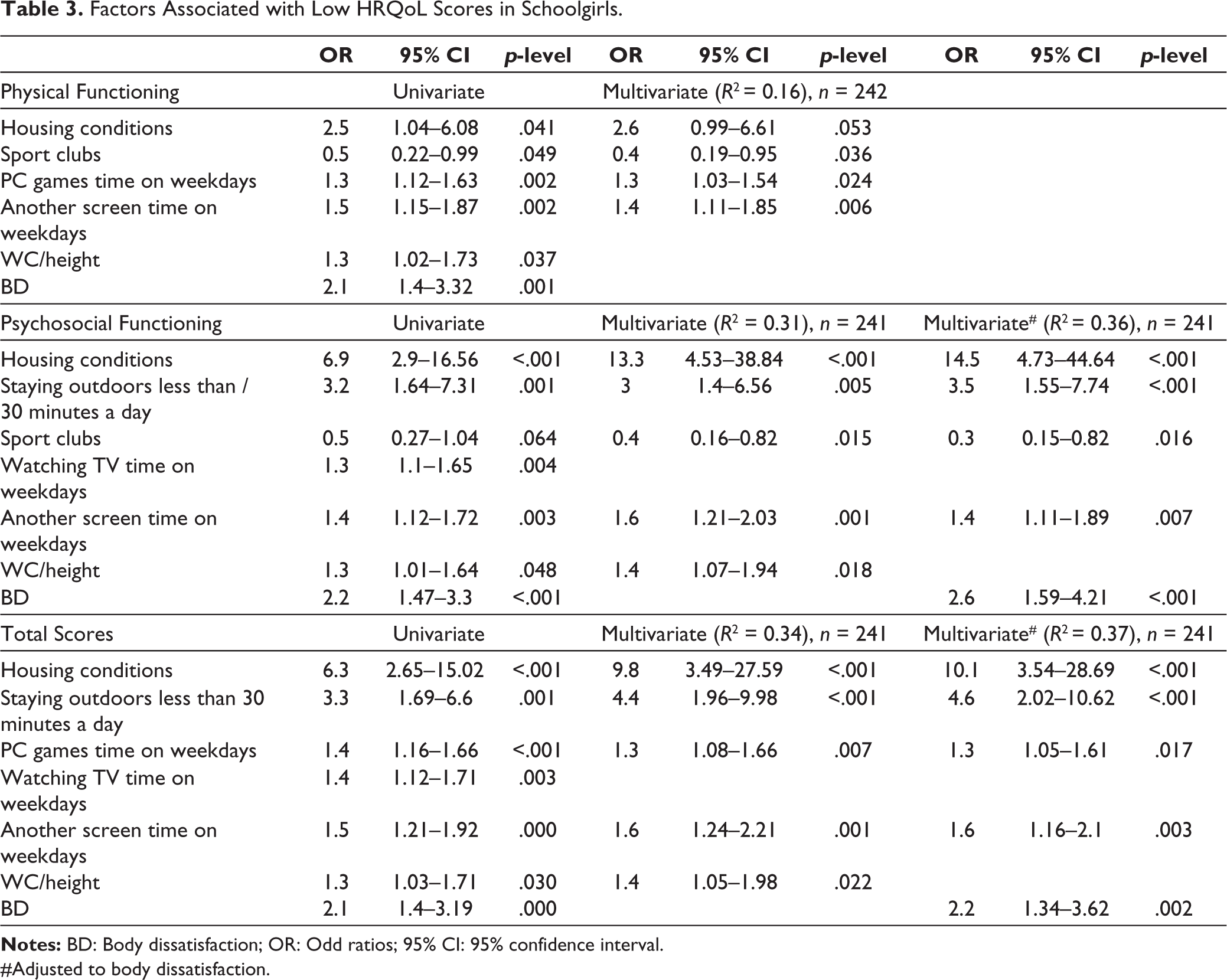
#Adjusted to body dissatisfaction.
The WC/height index did not confirm its significance for low scores in the PF domain, when considered in multivariate models adjusted for social and behavioral factors; therefore, no further analysis was conducted.
Low scoring in the PSF domain in the first-order multivariate model (without regard for BD) was associated with worse living conditions, insufficient time spent outdoors, long time at the computer screen and specific WC/height ratio (R2 = 31). However, after introducing BD into the model, the anthropometric variable ceased to be significant, although in general, the model demonstrated good quality and accounted for 36% of the dispersion of the dependent variable.
A similar pattern was observed for the life quality total score: the WC/height anthropometric variable, in a model giving consideration to significant social and behavioral factors, lost its independent significance after the introduction of the BD variable into the model (R2 = 37 for the final model).
Discussion
The research results suggest that anthropometric variables are not independent predictors of HRQoL in a community-based sample of urban tenth-year schoolchildren.
The study sample encompassed healthy adolescents of the same level of general secondary education, living in the same city. BMI Z-score values ranged from –3.23 to 3.32, but the prevalence of overweight was only in 9.2% (9.8% in the girls and 8.2% in the boys), and obesity—in 1.7% (0.8% and 3.1%, respectively). According to some recently published data, the prevalence of overweight and obesity in 16-year-olds from 17 Russian regions (n = 7065) was 14.5% and 2.7%, respectively, in girls and 16.5% and 4.7% respectively, in boys, with considerable variation by region. The lowest prevalence rates for overweight and obesity demonstrated for one of the regions were 11.2% and 3.3%, respectively. 20 The low prevalence of obesity in the considered sample, apart from the territorial factor, may also be explained by a sampling bias caused by the fact that overweight/obese adolescents were less willing to complete the Collins scale.
The girls’ HRQoL was lower than that of the boys in all domains except SF. The girls’ lower quality of life has also been demonstrated in most other studies.10,21–23 A possible explanation is teenage girls’ greater sensitivity to the physiological changes of adolescence, which in turn leads to degraded physical and psychological self-perception and HRQoL.24–26 Of some importance is the factor that boys in adolescence begin to follow the gender role that makes them less likely to express emotions and complain about health problems.
The present research did not reveal any significant association between HRQoL and BMI (BMI Z-score) in adolescents, except for a minor positive correlation between BMI and the ScF score in boys. However, the girls’ WC and WC/height index was to a great extent negatively associated with all HRQoL aspects except for ScF. Similar results were obtained in a study of Iranian adolescents aged 12–18, which found a significant inverse correlation of WC with the social functioning indices in girls, but not in boys, in the absence of a significant correlation between HRQoL and BMI in adolescents of either sex. 22 A study of a clinical sample of obese adolescents also found no interrelation between HRQoL and BMI, but revealed an association between the WC Z-score and the worse score in the EF domain and the overall HRQoL, regardless of gender or age. 5
In virtue of the lack of a significant association between anthropometric variables and integral characteristics of HRQoL in boys, subsequent stages of the analysis were carried out for girls only. The significance of the interrelation between WC and HRQoL was lost after giving consideration to BD, which suggests that this correlation was entirely mediated by dissatisfaction with one’s silhouette. It can be assumed that the girls’ HRQoL is influenced not by weight status per se, but rather by fat deposition specifics that change the silhouette shape and cause dissatisfaction with one’s appearance. Adolescent girls are particularly sensitive to changes in appearance; therefore, deviations from the accepted standards of feminine beauty, such as a slim figure and thin waist, may cause dissatisfaction with the body image even in girls who are not overweight as classified by BMI.
A study by Farhat et al. showed that the link between obesity and physical and emotional functioning, established in the primary analysis, as shown for a representative sample of schoolgirls in the USA, lost its significance after consideration of the BD variable. 27 A multi-ethnic sample of fifth-year schoolchildren (aged 10–11, 26%—with obesity) showed that children with obesity had a significantly lower PSF. However, when BD and global self-esteem were taken into account, the BMI factor, as a contribution to HRQoL, became irrelevant. 28 Moreover, a study of 205 adolescents with overweight and obesity showed that the revealed significant association between BMI and HRQoL was entirely mediated by the body image factor. 29 This suggests that the “weight status – BD – HRQoL” relationship is reproduced not only in community-based but also in clinical samples.
In the present study, the BD prevalence was quite high and comparable in frequency for both sexes. This is consistent with the results obtained for a cohort of 1035 Brazilian schoolchildren. 30 However, other studies have shown that BD is more common among girls;22,23 meanwhile, a study by Liu et al. showed that 8–12-year-old boys in China, in contrast, were more likely to be dissatisfied with their body than girls. 31 In Russian studies, the incidence of BD among adolescent girls is reported to be around 77%, slightly higher than the figure shown by us.32,33 This is probably due to the broader age range of the participants and the differing BD assessment tools used in the aforementioned studies. Moreover, no Russian studies considering the incidence of BD in boys were found.
The BD profile in boys and girls had the opposite direction. These results are similar to those found in other studies which report that, regardless of weight, girls tend to want to be slimmer, whereas boys strive to have big-bodied silhouettes.31,34,35 Furthermore, the present research revealed that adolescents of different genders not only had different preferences as to the desired body changes, but also showed a different effect of BD on HRQoL. Whereas BD affected only the EF domain in the boys, it affected all life-quality aspects of the girls, significantly impairing them, even after the consideration of sociodemographic and behavioral characteristics.
Among recent findings, a significant association with the HRQoL score was demonstrated by the lowest rating of adolescents’ living conditions, shorter outdoor exposure, and increased screen time. The connection between low HRQoL in adolescents with unfavorable socio-economic conditions and extended screen-viewing activities has been previously described.36,37 Additionally, research based on data from the UK Millennium Cohort Study, which explored whether the subjective perception of economic disadvantage among friends is associated with social challenges and poorer mental well-being during adolescence, revealed that perceived income inequality predicted adverse mental health outcomes and a range of interpersonal difficulties during adolescence, even when accounting for objective family income. 38
The observed association between poor PSF in adolescents and limited outdoor time can be explained by their reduced engagement in social interactions (active games with peers) as well as lower physical activity levels often associated with extended indoor stays. All forms of screen time (TV, computer, smartphones) also contribute to a sedentary lifestyle which leads to both physical and mental health issues. 39
The obtained results confirm that adolescents’ quality of life is influenced not by their actual weight but by satisfaction with their body image. These findings are reproduced in cohorts including both high and low share of participants with excessive body weight/obesity, as well as in the studies covering adolescent samples with participants willing to lose weight. The role of BD as an important predictor of poor HRQOL (especially PSF) in adolescents, as shown in this and other studies, may justify the use of simple screening tools for identifying groups at risk, such as poor emotional well-being, social integration and role functioning. Furthermore, our results support the potential benefits of mental health interventions aimed at improving adolescent’ perception of their own body image, both at the individual level and within community. In a societal context, where media resources promote unattainable ideals of beauty, such interventions could prove valuable for enhancing mental health.
Limitations and Strengths
When interpreting the findings, some limitations have to be taken into account. The study had a cross-sectional design; therefore, the causal relationship in the revealed association cannot be adequately revealed.
The study included adolescents living in one selected city, so the sample is representative of that city, not of all adolescents in the country. Thus, generalizations should be avoided for adolescents living in rural areas and those residing in other regions.
The selection of adolescents for the survey was made using an all-encompassing method; however, the formed sample consisted predominantly of normal-weight adolescents. This may have influenced the findings in exploring the interrelation between the HRQoL score and anthropometric parameters.
In order to clarify the true associations between anthropometric parameters and HRQoL, the authors made best efforts to consider a broad range of behavioral and socio-demographic confounding factors. However, a number of important factors connected with school environment and family background were not taken into consideration in this study.
The share of boys in the present study was lower than that of girls, reflecting the real gender ratio among 10th–11th-year students of high schools. Consequently, caution is needed when making a comparative interpretation of the results for adolescents of both sexes, as obtained in this study.
On the positive side, it should be noted that the research was carried out on a fairly homogeneous sample of tenth-year schoolchildren of regular schools, those not taking the final state examinations in the current year. This made it possible to minimize the stressful influence caused by work over an extended curriculum and excluded the stress associated with preparing for final examinations.
The anthropometric measurements in the present study were performed by trained medical professionals and, in addition to BMI, the WC and WC/height indices that characterize fat distribution specifics were assessed. Anthropometric variables were not treated as discrete categories but across a range of values, which may have greater sensitivity in revealing significant associations. It should be noted as well that the present research is the first Russian survey considering the association between weight status and HRQoL through the prism of BD.
Conclusion
The present research has shown that BD is widespread among adolescents and has a significant impact on the HRQoL of both girls and, to a lesser extent, boys. The impact of the actual weight status on girls’ quality of life is entirely mediated by their dissatisfaction with their own bodies, which justifies the necessity to pursue an approach to BD as a distinct problem with important psychosocial implications and requiring active identification and targeted intervention. More extensive research is required to clarify the association between weight status and HRQoL in boys.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study protocol has been approved by the Ethics Committee of the Scientific Centre for Family Health and Reproduction Problems (Study Ref No. 1, 09.03.2017).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.