
Abstract
Introduction:
The burden and impact of childhood emotional abuse (CEA) among children and adolescents utilizing psychiatry services is a less studied area, especially in the Indian context. This study aims to study the prevalence and correlates of CEA in adolescents attending psychiatry services and to understand the subjective experience of emotional abuse (EA) in this population.
Methods:
Adolescents aged between 12 and 18 years attending child and adolescent psychiatry (CAP) services were recruited for the study. The prevalence of CEA was assessed using ICAST-C (ISPCAN Child Abuse Screening Tool), temperament was assessed using the Malhotra Temperament Scale, and psychosocial adversities were assessed with the Parent Interview Schedule (PIS). From those reporting CEA, a few of them were interviewed to get narratives of subjective experiences of CEA, and this was analyzed using thematic analysis.
Results:
In total, 81 adolescents were recruited for the study, and among them, 82.7% (n = 67) reported at least 1 form of EA in the last year, and 93.8% (n = 76) of them reported a lifetime history of at least 1 form of EA. The frequency of other psychosocial adversities like abnormal intrafamilial relationships (n = 33; 40.7%) and inadequate or distorted intrafamilial communications (n = 49; 60.5%) was high in this sample. There was a significant association between the presence of EA in the last year and physical abuse (p = .00) and neglect (p = .01) in the last year. Narratives for qualitative analysis were collected from 21 adolescents. The most common themes in the context of CEA were related to academics (n = 10) and emotional and behavioral problems in the child (n = 7).
Conclusions:
There is a high prevalence of EA among adolescents attending CAP services. There is a high co-occurrence of other forms of abuse and other psychosocial adversities with EA. As adverse childhood experiences (ACEs) pose a high risk for future physical and mental health sequelae, this needs to be identified early and intervened with.
Introduction
Child abuse is an important area of public health importance and understanding its impact in the community is important for policymakers to plan prevention and safeguarding strategies. The long-lasting sequelae of child abuse on brain development and mental health are widely studied and have a strong evidence base. 1
Although the term child abuse entails different forms of abuse and neglect, emotional abuse (EA) and emotional neglect (EN) are often overlooked and under-researched. 2 But, recent evidence from meta-analyses points to a much higher prevalence of childhood emotional abuse (CEA) globally compared to other forms of abuse. 3
The community study on the prevalence of child abuse conducted jointly by the Ministry of Women and Child Development (MoWCD) and the United Nations Children’s Fund (UNICEF) (2007) reported prevalence of CEA to be 48.37% in India indicating that every second child in India has faced EA. 4 But, there are hardly any studies from India that looked into the prevalence of CEA in young people with mental health difficulties. Moreover, there is poor understanding of the relationship of CEA with various psychosocial adversities in the micro and macro environment of children and adolescents.
It is very important to understand the association of CEA with mental health difficulties because the odds of developing psychiatric comorbidity are quite high in those with a history of CEA. 5 Having other psychosocial adversities along with CEA can have a complex bidirectional interaction and as suggested by the research on adverse childhood experiences (ACEs), contributing to a higher burden of physical health and mental health sequelae. 6
Some of the challenges in doing research on CEA include lack of consensus in the definition of EA, difficulty in quantifying the frequency of CEA and its impact, and cultural differences in perceptions around CEA.7, 8 Another factor is the subjective difference in the processing of CEA, this the authors’ hypothesize is a factor in determining the impact of CEA in each individual. To understand this further, apart from looking at the quantitative variables that are related to CEA, we need to understand the subjective experience around CEA to understand the context and the emotional and cognitive processing of the event(s).
Thus, in this study, we aim to study the prevalence of EA in adolescents presenting with mental health difficulties and its association with various psychosocial adversities. We also aim to understand the subjective experience of EA among them and understand in depth the contexts and processing of the experience.
Methodology
This cross-sectional mixed methods study was conducted in the Department of Child and Adolescent Psychiatry (CAP), National Institute of Mental Health and Neurosciences, Bengaluru. Adolescents aged between 12 and 18 years who presented to the outpatient or inpatient services were included in the study. Those adolescents who had intellectual disability, autism spectrum disorder, or those currently in a psychotic episode were excluded. The study protocol was approved by the institutional ethics committee.
From the previous studies, the combined prevalence of CEA was estimated to be 36.3% (95% CI 28.1–45.4%) 9 and based on this, the sample size for this study was calculated to be between 80 and 100.
Patients attending the CAP services undergo a detailed mental health evaluation and a clinical diagnosis is made in discussion with a child and adolescent psychiatrist in the department. From among the patients who had already completed the detailed evaluation, study participants were recruited through convenience sampling.
A semi-structured proforma was used to collect the demographic and clinical details. ISPCAN child abuse screening tool (ICAST-C) developed by the “International Society for Prevention of Child Abuse and Neglect” was used to assess different forms of child abuse, including EA and EN. This is a scale which is validated in Indian population and has 52 items among which 18 items are specifically for EA. 10 For this study, EA was defined as that identified using ICAST-C.
Parent Interview Schedule (PIS) was used to assess psychosocial adversities. This instrument was put forth by WHO in 1988, and it focuses on the factors in the psychosocial environment of the child to be coded in the psychosocial axis (Axis 5) of the multiaxial classification system of child and adolescent disorders (WHO). This scale looks at the adversities in various environmental domains right from the family relationships to adversities in the school environment to any societal stressors. 11
The temperament was assessed using Malhotra Temperament Schedule. This schedule consists of 45 items to assess the temperament of the child in the domains of sociability, emotionality, energy, attentivity, and rhythmicity and each item is scored on a Likert scale. It was published in 1988 and is validated in Indian children. 12
From those who reported CEA, a small sample which was information rich was taken to study the subjective experience of CEA. An interview guide was prepared covering the domains—experience of the abuse, processing of the event and attribution, associated emotions, their action/response, and the current patterns. The interview guide was then translated into 3 other languages—Hindi, Tamil, and Kannada. This was then back translated to English by an independent person (who is a senior resident in the department) to English to ensure the accuracy of translation. Minor discrepancies noted were corrected. The final version of the interview guide was independently validated by 2 child psychiatrists. The questions were read out to the adolescents and the response was noted verbatim.
Data Analysis
Descriptive statistics was used for analyzing the sociodemographic details, clinical details, and prevalence of CEA. For qualitative analysis, thematic analysis was used. In the first step, the transcript was read more than once, notes were made and different emergent themes in each transcript were identified and these transcripts were coded based on the themes identified.
Results
A total of 80 adolescents were recruited for the study. The mean age of the sample was 15.3 years (1.69) with an almost equal proportion of males (n = 41) and females (n = 40).
Majority were recruited from the outpatient setting (n = 71, 87.5%). In total, 23 (28.4%) of them had a life time history of receiving inpatient care. Most common diagnosis in the sample was anxiety disorders (n = 16; 19.7%) followed by ADHD (n = 11; 13.5%). In total, 30.8% had more than 1 diagnosis.
From the PIS, 60% (n = 33) had inadequate or distorted intrafamilial communication and 40.7% (n = 33) had abnormal intrafamilial relationships.
Emotional Abuse
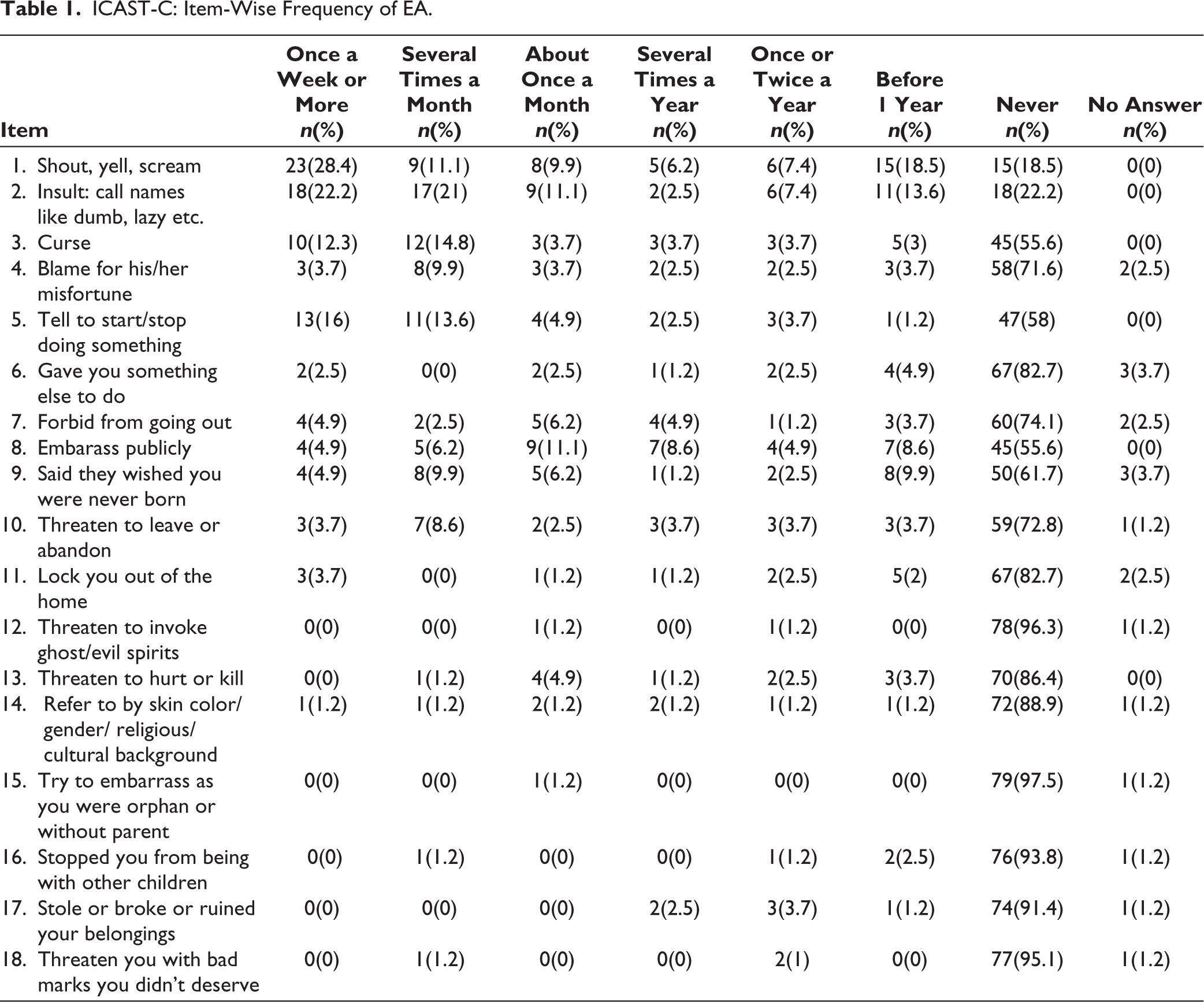
In total, 67 (82.7%) of the adolescents reported at least 1 form of EA in the last 1 year and 76 (93.8%) of them reported lifetime history of at least 1 form of EA. The most common form of EA reported in the past 1 year was Shouting, yelling, or screaming (n = 51; 45%) followed by insulting by calling names like “dumb,” “lazy,” etc. (n = 46; 44%). One-fourth of those who reported being shouted or yelled at reported this happened once or more than once a week (n = 23; 28.4%). Item-wise frequency of EA is tabulated in Table 1.
ICAST-C: Item-Wise Frequency of EA.
Emotional Neglect
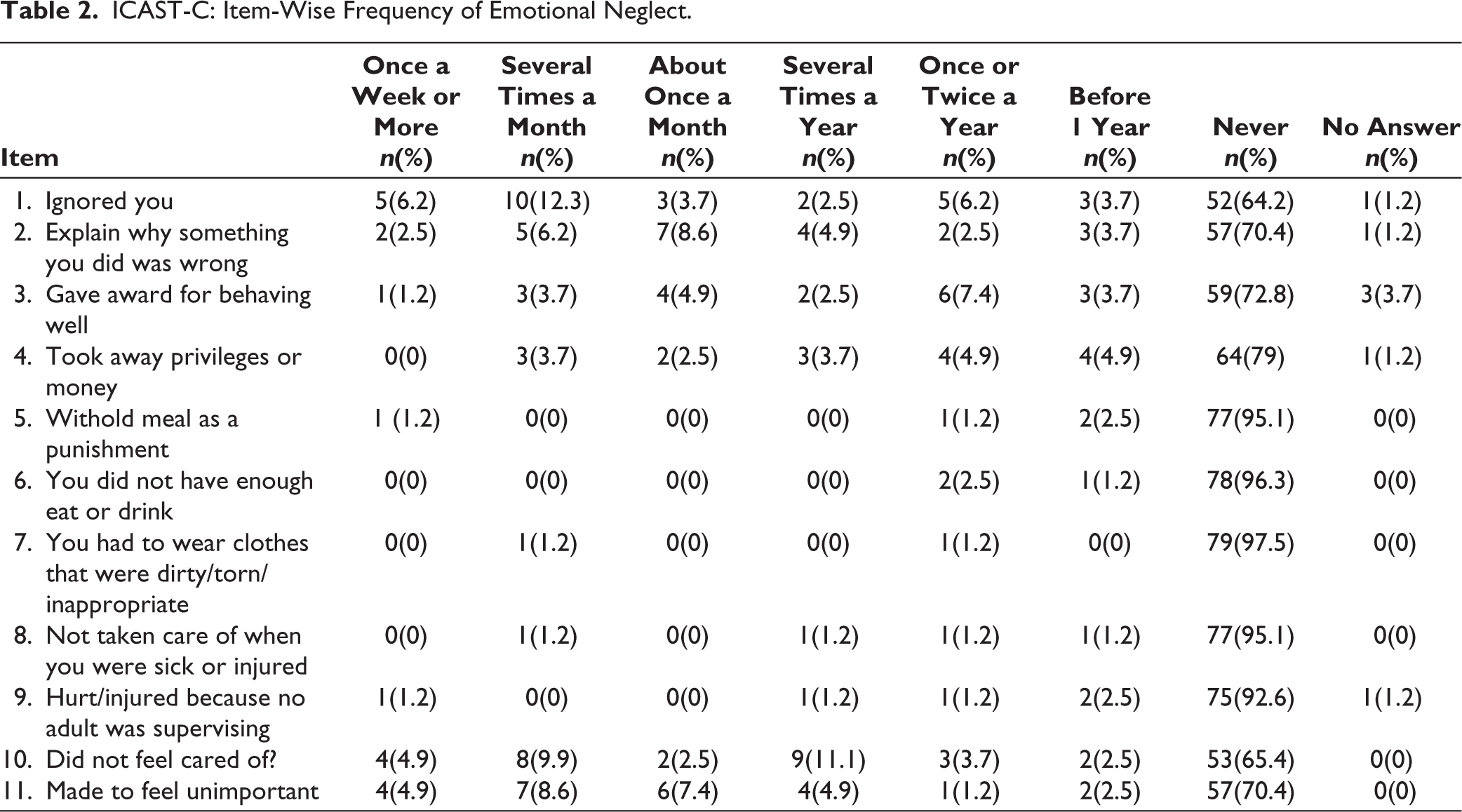
In total, 30.8% (n = 25) of the sample felt they were ignored by caregivers in the last 1 year. In total, 32% (n = 26) felt not being cared for and 27.1% (n = 22) felt they were made to feel unimportant in the last 1 year. Neglect related to material needs were reported only by 2 (2.5%). Table 2 shows item-wise frequency of neglect.
ICAST-C: Item-Wise Frequency of Emotional Neglect.
Other Forms of Abuse
Almost 60% of the sample reported lifetime history of physical abuse (n = 48) and 7 of them (8.6%) reported lifetime history of sexual abuse.
Interventions as per standard treatment protocols were provided to all the study participants who had reported abuse by the multidisciplinary CAP clinical team.
Association Between EA and Different Study Variables
Among the sociodemographic variables, there was no significant association between gender (Χ 2 = 0.003, p = 1.000) or socioeconomic status (Fisher’s exact p value = .462) with EA.
The psychiatric diagnosis of the adolescent did not have any statistically significant association with EA. There was also no significant association between different temperamental characteristics (as noted by Malhotra Temperament Schedule) and the presence of EA
In this study, there is significant association between presence of EA in the last 1 year and physical abuse (p = .00) and neglect (p = .01) in last 1 year, as well as lifetime occurrence of EA and lifetime physical abuse (p = .009).
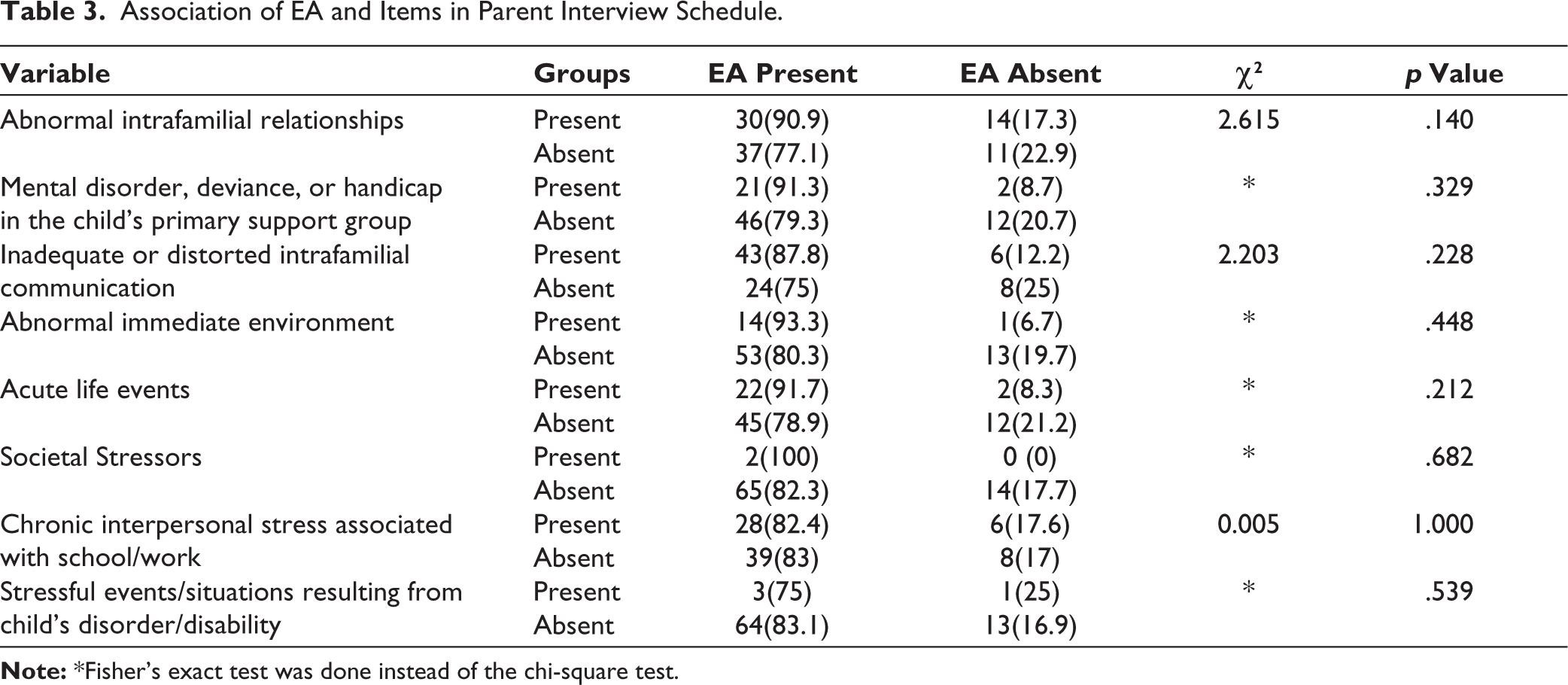
There was higher frequency of abnormal intrafamilial relationships, mental disorder, deviance or handicap in child’s primary support group and inadequate or distorted intrafamilial communication among those with EA but these associations were not statistically significant. Associations of different variables in PIS with EA has been tabulated in Table 3.
Association of EA and Items in Parent Interview Schedule.
Subjective Experience of CEA
Narratives for qualitative analysis was collected from 21 adolescents. The themes of the narratives were analyzed under the domains—context of EA, description of the act, processing of the event, feeling associated, and response to the event.
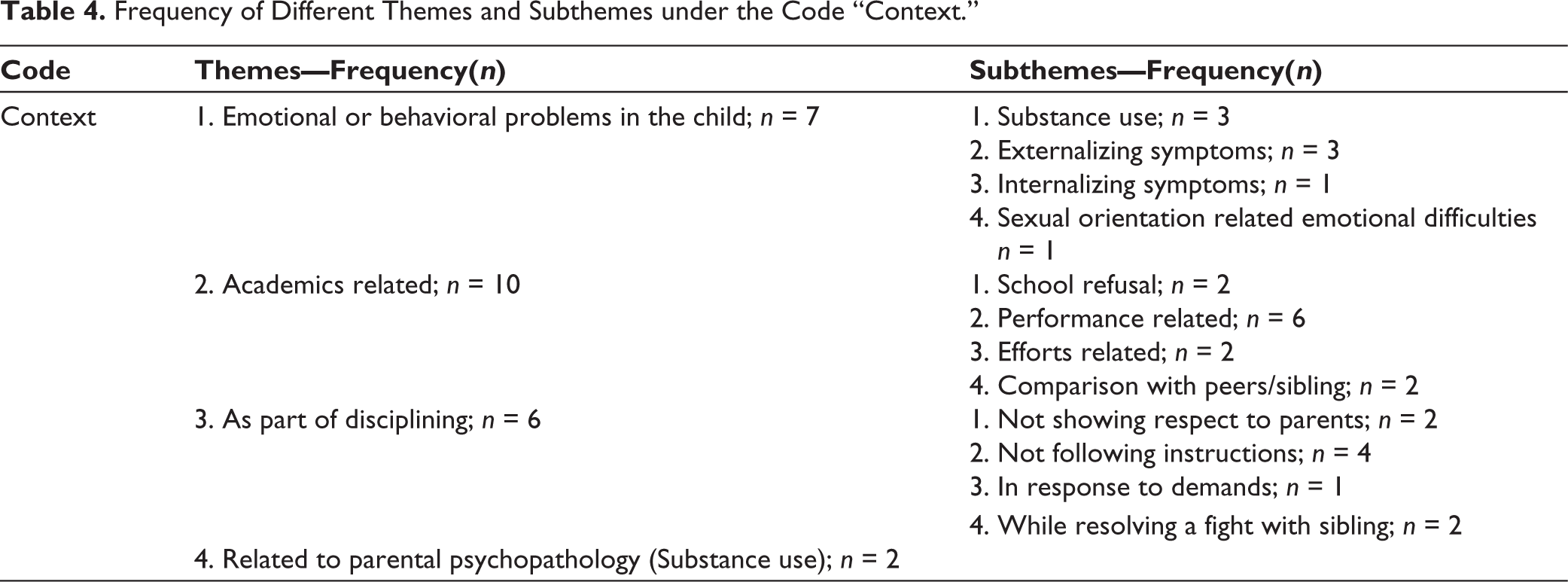
When the code “context” was analyzed, 4 themes emerged with subthemes which are mentioned in Table 4. The most commonly reported theme was Academics related (n = 10) followed by Emotional/behavioral disorder related (n = 7). Some examples of narratives related to each theme under the context are mentioned below:
“I could not do well academically, which my parents don’t accept. They yell at me and call me lazy, ungrateful and tell me that I’m a failure” (theme—academics related). “When I was in sixth standard, 1 day, I went to sleep and I overslept the next morning. I ended up missing school because of the time taken by my OCD, because of this my father told me that I was good for nothing and that money was being wasted on me. He said I was fit to be in a slum” (emotional/behavioral disorder related).
Most commonly reported themes under the code “Act” included the use of “bad words” (n = 8), making them feel unwanted (n = 7), and hurting self-esteem (n = 5).
Under the topic “processing of the event,” 3 codes were analyzed. (1) Thoughts about the event (during the event) (Process_during_event). (2) Self-attributed reason for the event (Process_reason). (3) Thoughts about event (present) (Process_think_present). Table 5 shows the frequency of various themes and subthemes under each of these codes.
Frequency of Different Themes and Subthemes under the Code “Context.”
Frequency of Different Themes and Subthemes under the Topic ‘Processing of the Event’.
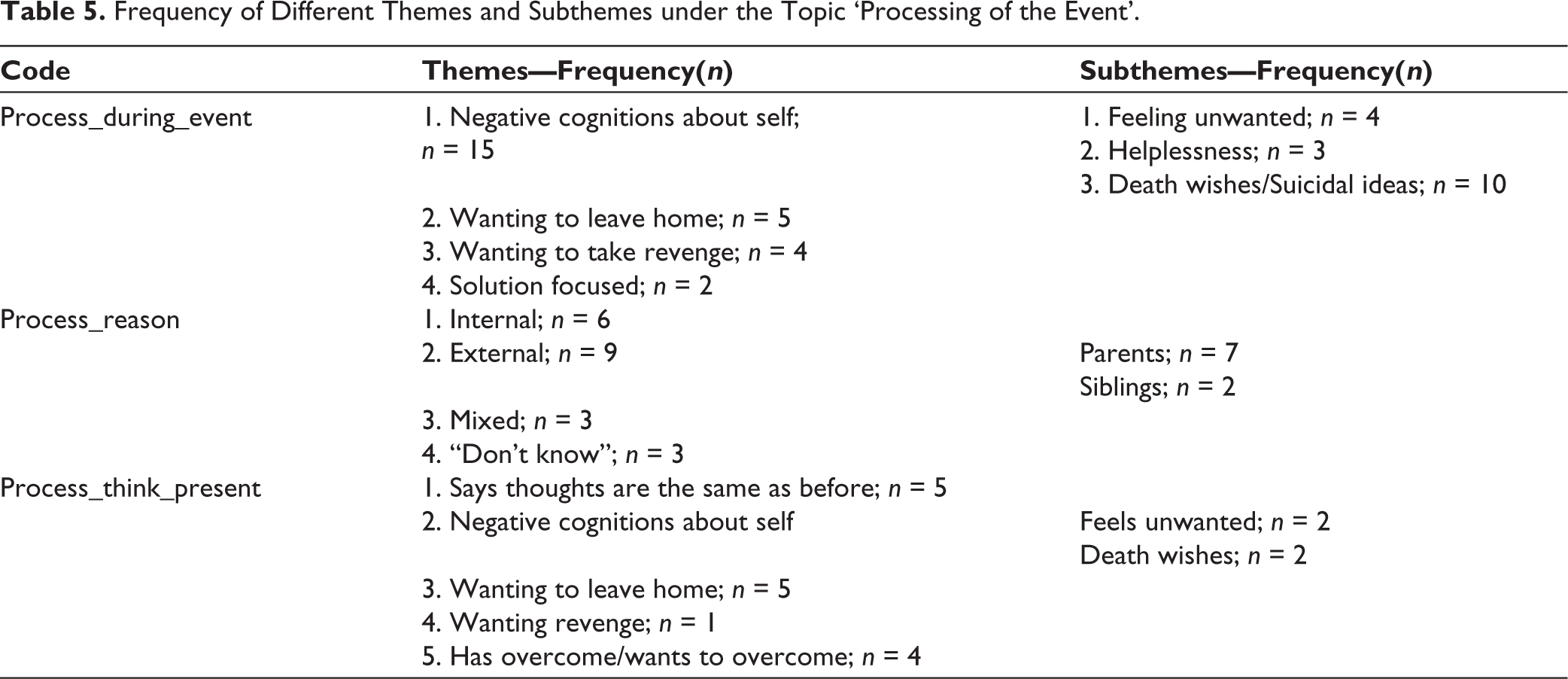
The themes commonly reported under the code “Process_during_event” were negative cognitions about self (n = 15), wanting to leave home (n = 5), and wanting to take revenge (n = 4). Some examples of these themes are mentioned below:
“I did not want to live; I felt I was a burden to my parents” “No one wants me. Even if I die it will not make any difference to them” “…. This is a headache I should get out of here”
The subjective emotions reported during the event were feeling sad (n = 16), angry (n = 10), and mixed emotions (n = 7). The response of the victims to the act of EA was Aggression (n = 10) (verbal aggression n = 5; physical aggression n = 5); Did “nothing” (n = 6); self-harm attempt (n = 4).
Discussion
Hospital Based Prevalence of EA
The current study looked at the hospital-based prevalence of EA among adolescents attending CAP services. Most of the previous studies that looked into EA among children and adolescents were community studies done in large populations.13–16 Here, in this study, we have specifically looked into adolescents aged between 12 and 18 years attending CAP services. Compared to community-based studies, this study gives an idea of the frequency of EA in a vulnerable group of adolescents. The sample was heterogenous in terms of clinical profile, with minimal exclusionary criteria with respect to diagnosis, thus giving a more generalizable picture of prevalence of EA in this population.
One of the most difficult tasks in doing research in CEA is defining EA. In this study, we have used a validated scale, ICAST-C which screens for all forms of abuse in a very comprehensive way. This is a scale which is validated in Indian population and has 52 items among which 18 items are specifically for EA. 10 Thus, compared to other studies which used scales with very few items for EA, this study has used a scale which takes a very comprehensive look at EA. This is one of the major strengths of the study.
In this study, the 1-year hospital-based prevalence of EA is found to be 82.7% (n = 67) and the lifetime prevalence of EA in the sample is 93.8% (n = 76). These rates are quite high compared to the previous community studies where the rates were in the range of 5.5% to 27.5%.13, 16, 17 But, the prevalence found in this study is comparable to some of the recent studies, for example, the school-based prevalence study of abuse among adolescents conducted in south India by Kumar MT et al., which found a 1-year prevalence of EA to be 84.5%. 18 The community study done by Nikolaidis G et al in 9 countries also found the prevalence of EA among adolescents to be in the range of 64.5% to 83.1%. 19 While comparing our results with other hospital-based studies, it is noted that the prevalence rate in this study is higher than the previous studies.20–22
Association of EA with Other Types of Abuse and Psychosocial Adversities
In this study, we could find significant association between presence of EA in the last 1 year and 1-year prevalence of neglect and physical abuse independently. The association was also true between lifetime EA and lifetime physical abuse. This is in line with previous studies which states that different forms of child abuse often co-occur.18, 23 Evidence suggest that the association of each type abuse independently with different mental health problems, and the association of multitype abuse with mental health problems are different. Those having EA with neglect and EA with physical abuse have higher chances of developing both internalizing and externalizing problems. 23 The presence of multi-type abuse also increases the burden of childhood adversity.
In this study, we have assessed the psychosocial adversities systematically using the PIS. 11 From the perspective of ecological systems theory of Bronfenbrenner, this scale helps us to capture the adversities from microsystem through to the macrosystem of the child’s environment. 24
Although statistical tests did not yield any statistically significant relationship between EA and psychosocial adversities, majority of those with EA also had abnormal intrafamilial relationships, mental illness in family and inadequate and distorted communication in the family.
One of the major take home messages from this study is how multiple adversities tend to co-occur in vulnerable population. Here, is a sample of adolescents who clinically have at least one psychiatric diagnosis and also have high rates of EA along with neglect, physical abuse as well as other psychosocial adversities like familial discord, distorted communication, and mental illness in family. If we are to go by the ACEs model, in this sample most of them have at least 1 adversity and many of them have more than one adversity in childhood thus rendering high risk for long term poor outcome in terms of mental and physical health. 25
Thus, what we intend to put across through this finding is that, EA is in itself an adversity but it often co-occurs with multiple other adversities of childhood causing higher risk for further poorer outcome.
Subjective Experience of CEA
One unique feature and strength of this study is its mixed methodology. Apart from assessing EA and its correlates using validated scale, we have also attempted to understand the lived experiences of children who has had EA.
Regarding the contexts of EA, in our sample the most common themes related to context of EA were (i) academics related and (ii) that related to emotional and behavioral problems in the adolescent. The academics related EA, if we look at the literature is prevalent and normalized in Asian culture.26, 27 Given its known prevalence in the culture and the corroboration of this finding in our study there is a need for including items related to this context in the available scales for making it culture suitable.
Another context which was common in this sample was EA related to the behavioral and emotional problems in the adolescents. This context is something which is unique to this population. From the literature, we can see that children with special needs are at higher risk for abuse, especially physical and EA. 28 Thus, there is a need for giving more attention regarding EA among this population and institute interventions for the same.
The themes under the act of EA captured in our study is comparable to those in ICAST-C. 10 The major themes were making them feel unwanted, hurting self-esteem, invalidation, and threatening most of which gets captured in the scale.
Thus, as discussed above, the acts that constitute EA is well captured in the scale used here, but it is the context of the abuse that differs. One may argue that the aim of the scale is to pick up the act and not the context. But, the context reflects the subjective meaning the adolescent gives to the act and this subjective experience determines the impact of the act upon the individual. It is very important to pick up this dimension as it influences the intervention for EA.
The other aspect of EA captured using the qualitative part of the study is the processing of the events by the adolescents in terms of thoughts and feelings and their response to the event. In this study, the major cognitions that were reported relating to the event of EA was negative cognitions about self, especially having death wishes/suicidal ideas. Among those who reported suicidal ideas related to the event, a few of them did self-harm. This is in line with the previous studies that reports high association of EA with suicidality and NSSI.29, 30 This is a very important finding from an interventional perspective, reiterating the need for identifying EA, understanding its impact on the child, and instituting specific interventions.
Conclusion
From this study, we understand that EA is highly prevalent among adolescents attending CAP services. There is also high frequency of psychosocial adversities and other forms of abuse (physical abuse and neglect) among them. Thus, we can see that that childhood adversities tend to co-occur and given its high future risk of mental and physical health sequelae, need to be addressed. Specific interventions focusing on children with significant EA as well as universal preventive programs for EA in the community need to be instituted.
Limitations of the Study
The sampling technique followed in this study is nonprobabilistic (convenience sampling) due to logistic reasons.
Majority of the patients were recruited from outpatient services; the number of inpatients in this study is less.
Since the groups with and without EA was largely skewed (4:1), identifying statistical associations with different correlates was difficult. A case-control study needs to be planned for the same.
Only adolescents were included in the study. Younger children, children with intellectual disability, and neurodevelopmental disorders who are vulnerable for EA were not included in the study.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
The study was approved by the Institutional Ethics committee of National Institute of Mental Health and Neurosciences (NIMHANS), Bengaluru on 27-02-2019 (NO.NIMH/DO/IEC(BEH.Sc.DIV)/2019). Written assent was obtained from each adolescent participant and written informed consent was availed from parents or guardians. The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.