
Abstract
The Protection of Children from Sexual Offences (POCSO) Act (2012) is a progressive legislation enacted in accordance with the child protection policies of India, with a basic premise of gender neutrality and with due consideration to the aspects of child development in complex and difficult judiciary processes. Deposition of the child survivors is a critical part of the POCSO trial processes. It is of paramount importance to consider the developmental and mental health aspects of children and how that would influence their understanding of the judicial processes and mental health consequences during judicial proceedings. Despite the guidelines and support measures for child-friendly court procedures, the courtroom experience can be intimidating for children causing stress and in turn negative mental health impact, and preparation interventions are of immense help in this context. We present two case vignettes where court preparation interventions were used to help children to feel empowered and confident, and minimize the impact of re-traumatization experienced in recounting their abuse experiences and consequently, enabling children to provide accurate testimony in the court.
Introduction
The Protection of Children from Sexual Offences (POCSO) Act (2012) is a child-centric and child-rights-based legislative framework in India. 1 The POCSO Act is a progressive legislation enacted in accordance with the child protection policies of India, with a basic premise of gender neutrality and with due consideration to the aspects of child development in complex and difficult judiciary processes. Deposition of the child survivors is a critical part of the POCSO trial processes. Proceedings of the criminal justice system, especially the courtroom experience can be intimidating for children.2,3 It is of paramount importance to consider the developmental and mental health aspects of children and how that would influence their understanding of the judicial processes and mental health consequences during judicial proceedings.4,5
The first guidelines for recording of evidence of vulnerable witnesses (defined as a child less than 18 years of age), in criminal matters were put forth by the Delhi High Court, with prime objectives of eliciting and securing complete, accurate, and reliable evidence from vulnerable witnesses and minimizing harm as a consequence of participating in the judicial process. 6 The Supreme Court of India has directed all the state high courts to set up vulnerable victims deposition centers within their jurisdiction as per the Delhi High Court guidelines. 7 It has been since recognized by the Supreme Court of India, and the definition of vulnerable witnesses is expanded to include age and all victims of sexual assault irrespective of gender, witnesses suffering from mental illness, and any other disability such as speech or hearing impairment among others. 8
The guidelines and structured protocols for recording the evidence of vulnerable witnesses include identification of stressful factors of the adversarial criminal justice systems, such as multiple depositions, delays and continuances, arranging pre-trial visits to the court, meeting the judge, and provision of legal assistance such as allowing the presence of a support person and court-appointed facilitator during the deposition. 6 The child-friendly court procedures include in-camera trial, not coming face-to-face with the perpetrator, recess during deposition, and allowing a comfort object such as books, toys, etc. All questions to the child, including cross-examination shall be put only through the court. These child-friendly measures are in place to avoid and minimize re-traumatization and secondary victimization of the child. Despite the support measures, the courtroom experience can be intimidating for children causing stress and in turn negative mental health impact, and preparation interventions are of immense help in this context.
We present two case vignettes where court preparation interventions were used to help children to feel empowered and confident, and minimize the impact of re-traumatization experienced in recounting their abuse experiences and consequently, enabling children to provide accurate testimony in the court. Informed consent was obtained from the parents and informed assent was obtained from the adolescents themselves prior to drafting this case series.
Case Vignette Description
Case Vignette 1
Ms. K is 14 years old, and studying in eighth standard. K had been abused by two unknown perpetrators when she was six years old, and a case was immediately registered under the POCSO Act. K was diagnosed to have Attention Deficit Hyperactivity Disorder and Posttraumatic Stress Disorder (PTSD) with difficult temperament in the background. She received intensive inpatient treatment at the child psychiatry ward. She was under follow-up and received psychotherapeutic interventions based on developmentally appropriate principles (initial trauma work using play-based strategies, followed by developmentally focused work on self-regulation, and support for academic difficulties) until she was 10 years of age. During longitudinal follow-up, K was noted to have emotional and behavioral dysregulation in the context of interpersonal relationships, challenges in maintaining peer relationships, and academic difficulties. She would often utter words like “I will kill them,” “there are snakes here,” and these utterances had recurrent themes of abuse and aggression. Over the course of eight years, K showed some improvement in self-regulation.
The child was summoned to testify in court for the first time when she was 14 years of age. She presented with intense arousal, anxiety regarding “attending the court,” fear of having to recollect details of the abuse, and “having to miss preparations for her eighth std half-yearly exams” due to the court proceedings. She expressed her concerns regarding “not being aware of what she should do in the court,” “why should she recollect details of the abuse that happened many years earlier,” and “fear of identifying the wrong person as the perpetrator” given the undue time lapse.
Case Vignette 2
Ms. S is 11 years old, studying in sixth standard. At the age of 7, S presented to the child psychiatry clinic with crying spells, expressing suicidal ideas and feelings of guilt after the recent disclosure of a long-standing intrafamilial child sexual abuse. On initial evaluation, S was noted to have ambiguous emotions and cognitions about herself and the perpetrator: “I am a bad girl” versus “they did something dirty to me,” “I am at fault” versus “they are responsible for what happened to me.” She was diagnosed to have depression and PTSD and was treated on an inpatient basis for two months.
Psychotherapeutic interventions included trauma-focused cognitive behavior therapy using developmentally appropriate techniques and supportive work with parents. Over a period of eight months, the child showed improvement in her symptoms, with return to premorbid socio-academic functioning. However, she continued to have frequent intrusive memories related to the abuse events presenting as somatic symptoms and periods of anger outbursts. She often expressed anger towards the perpetrators saying, “I want to go and ask them, why they did this to me,” “I want to shout at them and punish them.”
The child was summoned to the court to testify for the first time, three years after filing the first information report. She reported for follow-up along with her parents with concerns of increase in intrusive traumatic memories and “not wanting to attend court.”
Court Preparation Interventions for Child Witnesses
The children were seen for court preparation interventions about a month before the deposition and the sessions were spaced over two weeks. The initial sessions focused on facilitating stabilization of the child’s mental health, so as to provide a sense of calmness and control for the child. Simple exercises such as relaxation strategies, playing games, and stories were practiced and children were reminded to use them whenever they experienced anxiety/intrusive memories. This was followed by “setting the context”—priming about the legal processes, the concept of justice and injustice, and the role of the judicial processes in obtaining justice. Trauma work during the intensive treatment phase was consolidated, specifically in areas focusing on self-concept, healing, and recovery. 9
Drawings were used to give children a geographical orientation of the courtroom, the spaces where the judges and lawyers will occupy, and ways in which the child’s safety will be ensured in the courtroom (e.g., the presence of police personnel in the courtroom). Discussions regarding child-friendly procedures were taken up. This was done to introduce the concept of the courtroom in a non-threatening and less intimidating manner and to increase familiarity.
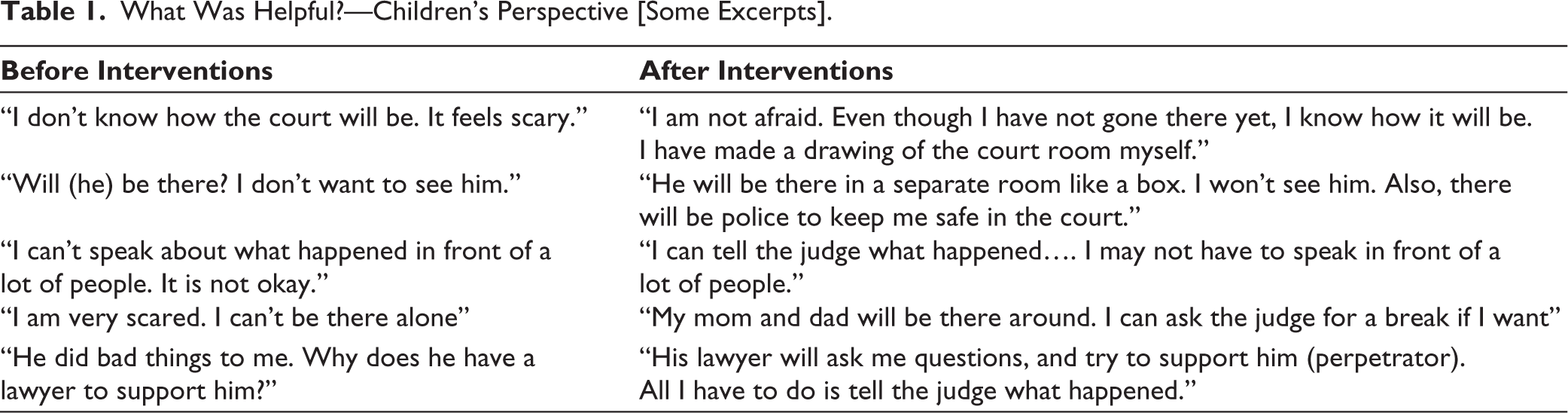
One of the most critical phases during the child’s deposition is describing the offense. Providing details of the abuse incidents are essential to assess the nature of the abuse and punishments in accordance to the POCSO act.1,4,9 Desensitization through games of naming body parts, including names for private parts was used, to help children be comfortable to describe the abuse events. “Telling all that they can remember in as many details as possible to help the judge understand what happened,” and “saying I don’t know for questions that they do not know answers for” were discussed. Children were empowered to face the hostility of the defense and their concerns about the consequences of deposition were addressed. Table 1 describes excerpts from children regarding concerns related to court proceedings before and after the interventions.
What Was Helpful?—Children’s Perspective [Some Excerpts].
Discussion
The objectives of the court preparation interventions are to address emerging mental health concerns, reduce re-traumatization, and help children to feel empowered and confident to provide accurate testimony in the court. In the above-described cases, the significant time lapse from the initial registration of the case posed enormous stress for the children. Both children had a negative mental health impact, and this is relevant as it impacts the child’s ability to recollect and recount their experiences in the court and could potentially impact their credibility as witnesses.4,9,10
Child development and child rights frameworks form the crux of the court preparation interventions. Introducing concepts related to the court proceedings and the role of the child as a witness is essential to enable and empower children. In accordance with the right to participation, supporting the child in developmentally appropriate ways to understand the court proceedings that are beyond expected for their developmental and chronological age, will enable children to participate in the optimal way they can.
Alongside discussions about court proceedings, it is essential to look out for emerging signs of emotional and behavioral sequelae of trauma. Affect regulation, enhancing skills for coping with distress and discussing with children, ways in which they can utilize in the courtroom, the armamentarium of skills that helped them earlier would help enhancing sense of control. Familiarity of the courtroom and a sense of safety were perceived to be helpful by the children. Desensitization of anxiety and taboo related to describing the offense and using the right lexicons to describe the nature of the offense will help children to provide a more accurate testimony. Using developmentally appropriate methods that suit the needs and vulnerabilities of the child is crucial for court preparation interventions to be helpful. Debriefing after the deposition and providing continued mental health support as required are essential processes.
Conclusion
While the trial outcomes cannot be modified, supporting children in helpful ways during the process is actionable. Mental health professionals working with children and adolescents have to familiarize themselves with the strategies to prepare children to face the courtroom procedures as part of the trial under the POCSO Act, 2012.
Footnotes
Acknowledgements
The authors would like to acknowledge the families who consented to their case summaries being included in this paper.
Authors’ Contribution
Dr Harshini Manohar contributed the case summaries, conceptualized the paper and drafted the manuscript Dr Eesha Sharma and Dr John Vijay Sagar reviewed and contributed to the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Informed assent and written informed consent was obtained from all the patients and their parents respectively.