
Abstract
Background:
COVID-19 pandemic and the lockdown which were its consequences have resulted in both short-term and long-term implications in mental health of adolescents. This study was conducted to assess the prevalence of stress, anxiety, and depression among students in the post-COVID period and its risk factors.
Methods:
This cross-sectional study was conducted among 300 students studying grades 9–12 in government high schools and higher secondary schools in a city in South India in October and November 2021. A self-administered questionnaire containing socio-demographic data and DASS-21 scale was used. The outcome variable, namely prevalence of stress, anxiety and depression was expressed in proportion with a 95% confidence interval. The relation between an outcome variable and socio-demographic variables was determined by a chi-square test and p value <.05 was considered significant.
Results:
Mean (standard deviation) age was 15.76 (1.104) years and 50.7% were boys. The prevalence (95% confidence interval) of stress, anxiety and depression were 30.3% (25.18–35.88), 47.3% (41.57–53.15) and 56.7% (50.85–62.35), respectively. Maternal illiteracy was significantly associated with stress and depression (p < .5).
Conclusion:
Consequent to the COVID-19 pandemic, almost one-third of school-going adolescents aged 14–18 years’ experience stress and almost half of them experience anxiety and depression which is comparable to that observed before the onset of this pandemic.
Introduction
An outbreak of a novel coronavirus disease (COVID-19) spread from Wuhan, China in December 2019 and became a pandemic affecting every continent. 1 Covid infection was declared as a pandemic by World Health Organization (WHO) in January 2020 and affected people in very large numbers across the world. 2 In the state of Tamil Nadu, as a response to pandemic, lockdown was imposed and schools were closed from 23 March 2020. 3
High level of stress and anxiety are natural responses towards any sorts of unnatural situation. 4 COVID-19 pandemic and lockdown has brought about a sense of fear and anxiety around the globe. This phenomenon has led to short term as well as long term psychosocial and mental health implications for children and adolescents. 5 Specifically, isolation, engaging in online classes, social media addiction, lack of outdoor physical activity, lack of peer interaction and parental pressure have added to student stress. 6 Students felt discontinuity during the lockdown even though the state government issued various educational policies on conducting virtual teaching sessions.
A study done among international students living in China showed almost three-fourths of them experienced depression and anxiety, while half of them experienced stress. 7 There is a dearth of literature on mental status of our school students. This study was conducted with the primary objective of estimating the prevalence of stress, anxiety and depression among school-going adolescents following COVID pandemic. Secondary objective was to determine the relation between socio-demographic variables and stress, anxiety, and depression.
Materials and Methods
This cross-sectional study was conducted among students in grade 9–12 at Government high schools and higher secondary schools from three particular zones of a city in South India from October 2021 to November 2021. Healthy school children of age 14–18 years studying in class 9 to class 12 were included in the study, while those among them who did not consent and those on any long term medications were excluded. Sample size was calculated using n master software based on a study which reported a 25% prevalence of stress among students with estimated error 5% and alpha error 5%, minimum sample size was calculated to be 289. 8 Hence it was planned to include 300 students in the study. Schools covered under District Early Intervention Centre of the institution under Rashtriya Bal Swasthya Karyakram (RBSK) Programme were considered and they came under three corporation zones. We recruited 25 students from each class (IX, X, XI, and XII) amounting to 100 from each school. The first 25 names from the attendance register as per alphabetic order who were present on that day were recruited from each class. As the sample size required is 300, we visited three schools, one from each zone selected by simple random sampling from the list of schools to include the required number.
The study was commenced after obtaining approval from the Institutional Ethics Committee (No. 633/2021) and the Chief Educational Officer from Chennai Corporation. The headmaster/headmistress of the selected schools was approached and their permission was obtained. Students were briefed about the study and the parental consent forms were distributed to them. The consented students were included in the study. They were given a self-administered questionnaire containing socio-demographic variables and Depression, Anxiety, Stress Scale-21 items (DASS 21) questionnaire. 9 The socio-demographic variables included age, gender, parental education, occupation, income, socio-economic status (as per Kuppuswamy scale), number of siblings, mode of access to education, mode of recreation during lockdown and about the peer group in their neighborhood. The students were asked to mark their responses to the questions in person, in the class.
The DASS-21 scale is a set of three self-report scales designed to measure the emotional states of depression, anxiety, and stress. Each of the three DASS-21 scales contains seven items, divided into subscales with similar content. The depression scale assesses dysphoria, hopelessness, devaluation of life, self-deprecation, lack of interest / involvement, anhedonia and inertia. The anxiety scale assesses autonomic arousal, skeletal muscle effects, situational anxiety, and subjective experience of anxious affect. The stress scale is sensitive to levels of chronic non-specific arousal. It assesses difficulty relaxing, nervous arousal, and being easily upset/agitated, irritable/over-reactive and impatient. Scores for depression, anxiety and stress are calculated by summing the scores for the relevant items. Before interpreting the scores, the summed numbers in each sub-scale need to be multiplied by 2 (this is because the DASS 21 is the short form of the scale). The scores were interpreted and the children were categorized into normal (0–14)/mild (15–18)/moderate (19–25)/severe (26–33)/extremely severe stress (34 and above) depending upon their scores for stress. Anxiety and depression scores were interpreted on similar lines according to specified intervals. Those found to have moderate and severe depression, anxiety and stress were referred to psychologist at district early intervention center for detailed evaluation and intervention.
Data was entered in Microsoft Excel and analyzed using IBM SPSS statistical software version 23.0. Numerical variables were summated as mean and standard deviation and categorical variables as proportion. The outcome variable was expressed in proportion with a 95% confidence interval. The relation between outcome variable and socio-demographic variables was determined by chi-square test and p value <.05 was considered significant.
Results
The study included 300 students in the age group of 14–18 years. The mean (standard deviation) age was 15.76 (1.104) years. One hundred and fifty-two (50.7%) students were males. Forty-seven (15.9%) fathers were illiterate while the remaining were literate. Eighteen (6%) fathers were unemployed. Forty-four (14.7%) mothers were illiterate while 162 (54%) of them were employed. Majority (87.4%) belonged to lower socio-economic stratum as per Kuppuswamy classification. Sixteen (5.3%) of them did not have siblings. Only 27 (9%) children did not have any access to education. While majority (75%) had access to education through a mobile phone, the remaining used television for the same. While screen time (television and mobile games) was the recreation in majority (49%), other modalities were outdoor play (33%) and reading books (17%). Only 67 (22%) did not have any friends in neighborhood.
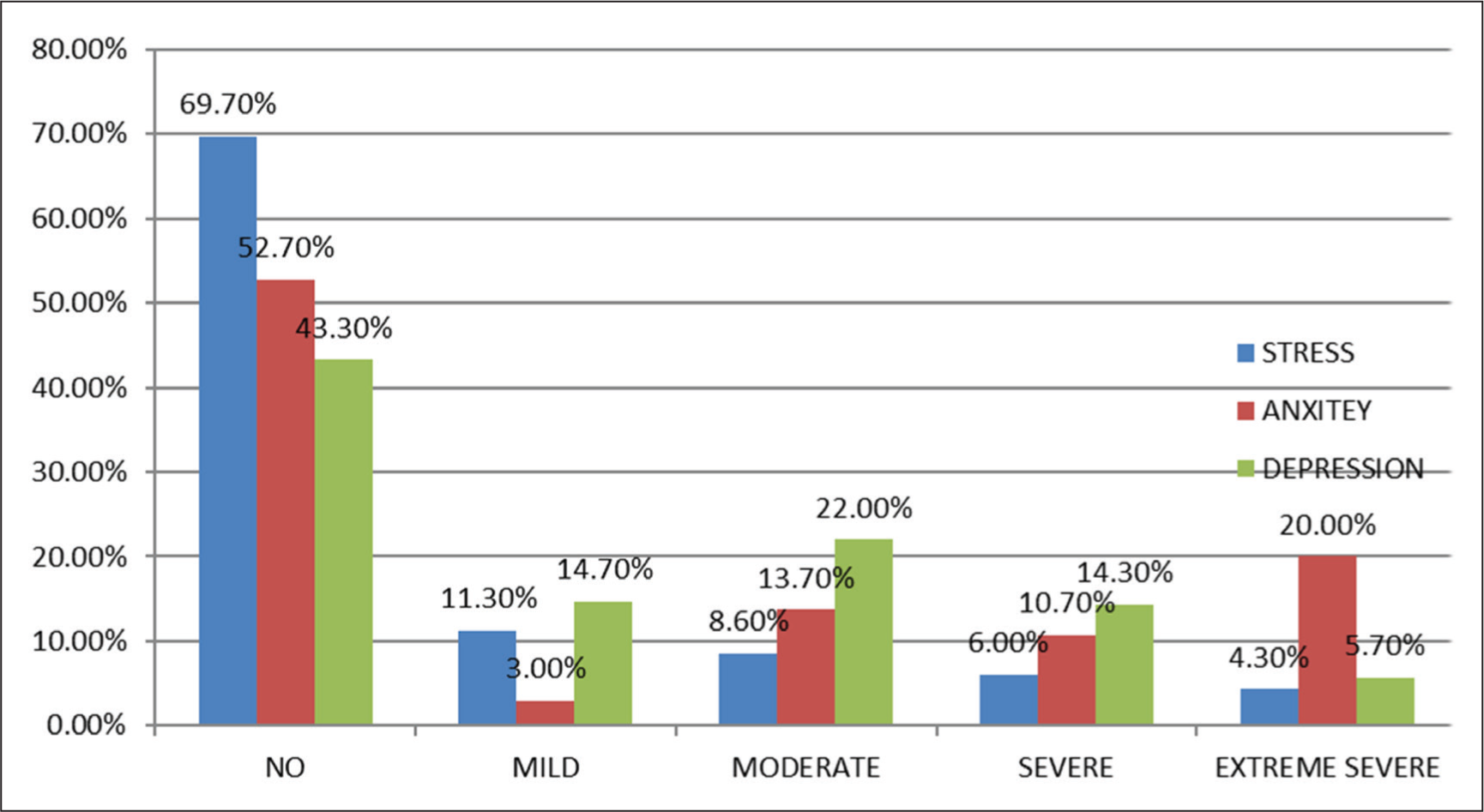
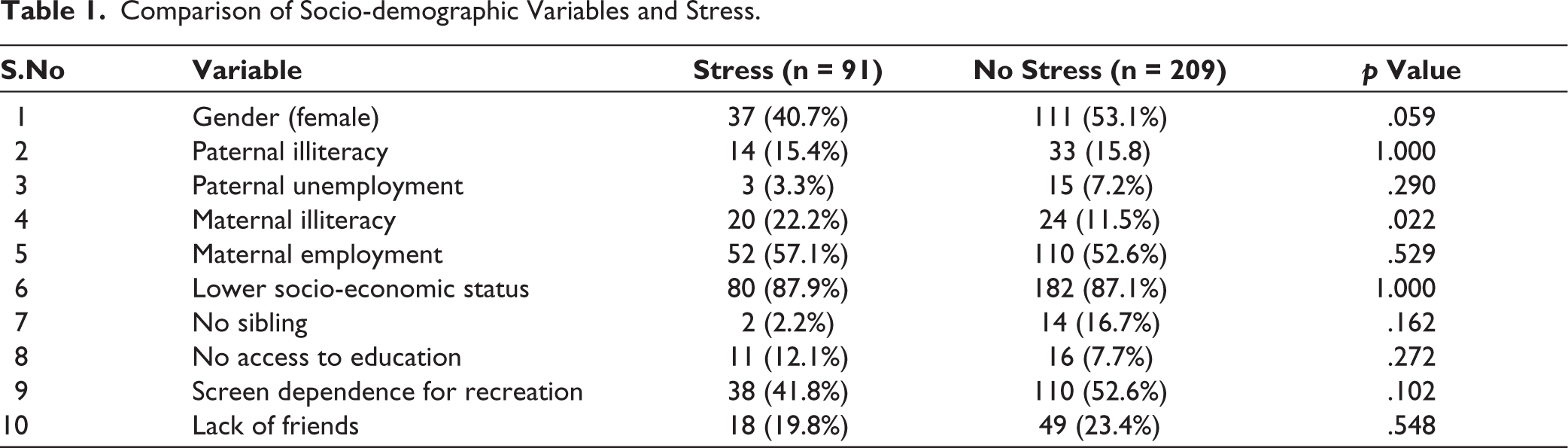
The mean (standard deviation) stress score was 10.97 (9.86). The prevalence (95% confidence interval) of stress among school students was found to be 30.3% (25.18–35.88). Thirty-four (11.3%) had mild stress, while 28 (8.6%) had moderate stress, 18 (6%) had severe stress and only 13 (4.3%) had extremely severe stress (Figure 1). Among socio-demographic factors, maternal illiteracy was significantly associated with stress in students (p = .022) which is depicted in Table 1.
Prevalence of Stress, Anxiety, and Depression in School Children.
Comparison of Socio-demographic Variables and Stress.
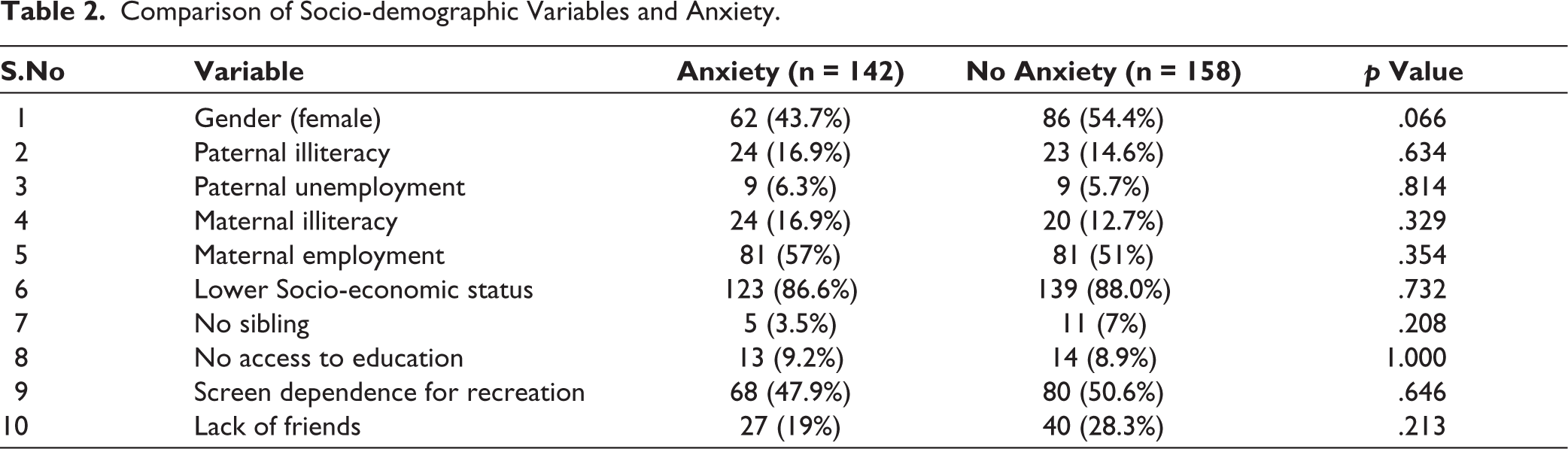
The mean (standard deviation) anxiety score was 10.01 (9.58). The prevalence (95% confidence interval) of anxiety among school students was found to be 47.3% (41.57–53.15). Nine (3%) had mild anxiety, while 41 (13.7%) had moderate anxiety, 32 (10.7%) had severe anxiety and as many as 60 (20%) had extremely severe anxiety (Figure 1). None of the socio-demographic factors were significantly associated with anxiety in students, which is depicted in Table 2.
Comparison of Socio-demographic Variables and Anxiety.
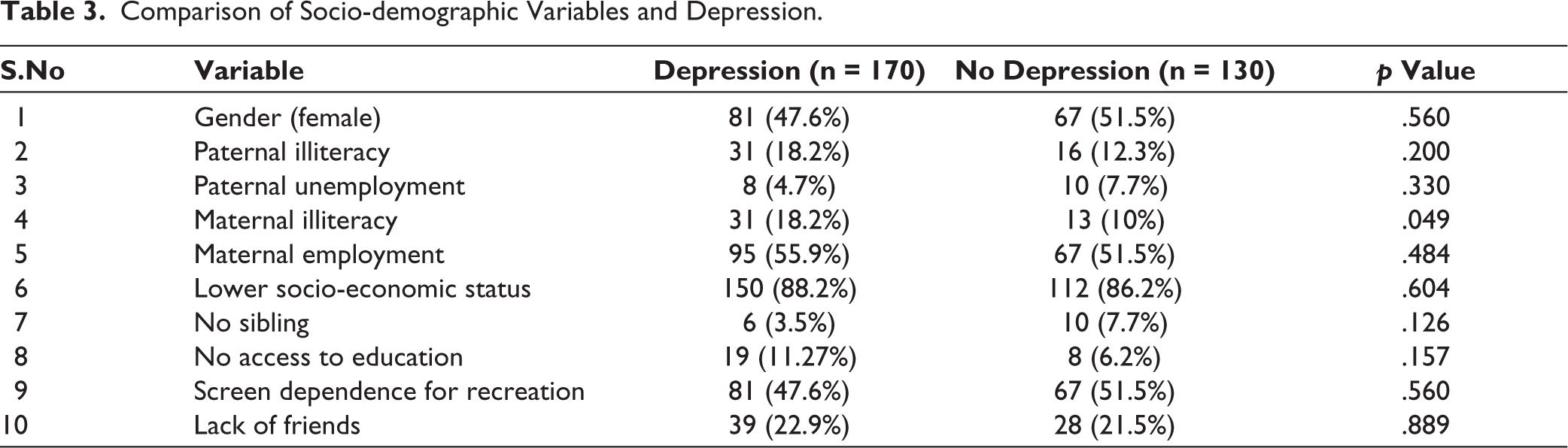
The mean (standard deviation) depression score was 12.00 (9.36). The prevalence (95% confidence interval) of depression among school students was found to be 56.7% (50.85–62.35). Forty-four (14.7%) had mild depression, while 66 (22%) had moderate depression, 43 (14.3%) had severe depression and 17 (5.7%) had extremely severe depression (Figure 1). Among socio demographic factors, maternal illiteracy was significantly associated with depression in students (p = .049), which is depicted in Table 3.
Comparison of Socio-demographic Variables and Depression.
The other socio-demographic variables namely gender, paternal illiteracy, paternal unemployment, maternal employment, socio-economic class, absence of sibling, lack of access to education, screen as a mode of recreation and lack of friends in neighborhood did not show any association with stress, anxiety or depression.
Discussion
Adolescence is a transitional phase from child to an adult. During this phase, lots of physical, psychological and behavioral changes take place which contribute to various mental health issues. Mental health problems like depression, anxiety and stress can lead to various behavioral issues at school or home, increases involvement in health risk behaviors like substance use, alcoholism and can lead to reduced academic performance in schools. 10 Worldwide around 10%–20% of children and adolescents are estimated to be affected by mental health issues. First step in addressing these issues is quantification of the problem.
This study was done on high and higher secondary school students to quantify their level of stress, anxiety and depression in the post-covid era. Stress, anxiety and depression were encountered in 30%, 47%, and 57% of school students respectively. Maternal illiteracy emerged as a significant risk factor of stress and depression in school children.
The burden of stress, anxiety and depression in our school students is similar to that reported among undergraduate students of Bangladesh, but lesser than that reported in Brazil and China.11–13 Chinese studies reported a prevalence of stress, anxiety and depression rates of 58.5%, 76.6%, and 73.4% respectively. 7 Such high rates in China are understandable as China was the epicenter of the pandemic. The relatively lower prevalence of mental issues was noted in our study despite the fact that very high number of covid-19 cases and mortality were reported in our country, especially during second wave. This could be attributed to the swift pandemic response actions taken by our government, the faith of people in Government, coping mechanisms contributed by cultural and ethical values of our people and a stable family structure prevalent in our country.
Studies done prior to onset of covid pandemic in various parts of our country have shown varying rates of stress, anxiety and depression. A study done in Manipur showed least prevalence rates of stress, anxiety and depression at 21%, 24%, and 20%, respectively. 13 Studies done in metropolitan cities like New Delhi and Pune showed a higher rate of mental health issues.14,15 A study done in state of Tamil Nadu in pre-covid era has shown higher rates of stress, anxiety and depression of 39%, 64%, and 56% respectively. 16 Another study has shown still higher rates of 25%, 87%, and 74%, respectively. 17 Such higher rates of mental health issues in pre-covid era could be attributed to academic stress of children which is very high in our state compared to other parts of the country.
The mean DASS scores of stress, anxiety and depression in a study done in the same region were more than that reported in our study. 18 When analyzing the severity of mental health issues in our study it was noted that around 10% had severe and extremely severe stress, 20% had severe and extremely severe depression and 30% had severe and extreme anxiety. This is a matter of concern and these children need counselling to prevent progression into mental disorders.
Among socio-demographic factors, maternal illiteracy was significantly associated with stress and depression in school children. It is a well-known fact that maternal education has positive relation with health outcomes of children. 19 This study reiterates that this effect is not confined to physical health, but extends to mental health. That is the reason why female literacy is considered as one of the key factors in calculating development index of any country. Maternal illiteracy results in poorer parenting skills leading to mental health issues in children.
This study has identified mental health issues in sizeable number of school children. But this is not in excess of that reported by studies done in the same area prior to the onset of pandemic. In fact, it is found to be lesser than that. The possible reasons could be lesser academic stress contributed by easier evaluation methods and lesser pressure to perform due to lack of physical classes, more time for recreational activities and more family time due to lockdown. However, since one in three children have severe mental health issues, it is advisable to employ counsellors in schools who can offer counselling to children on regular basis which will go a long way in improving their mental health.
The strength of the study is that it is first of its kind done in our population done using a prevalidated and reliable instrument. The main limitation of this study is the data on mental health status of these children prior to onset of a pandemic is not available for comparison. This is offset by the fact that there is enough published literature on this from the same region with which it can be compared. The data on confounders of mental health issues like past history of mental illness and history of mental illness in family are not available. Children belonging to only lower socioeconomic strata were included leading to selection bias. Further, the tool used, namely DASS is a screening tool and not a confirmatory tool.
To conclude, almost one-third of school-going adolescents aged 14–18 years’ experience stress and almost half of them experience anxiety and depression. Mental health issues namely, stress, anxiety and depression are encountered in a sizeable number of high and higher secondary school children in post-covid era, but not in excess of that reported prior to the onset of pandemic. Maternal illiteracy is a risk factor for stress and depression in children. The study reiterates the fact that mental health issues are found in a large number of apparently healthy and normal adolescents and hence there is a need for periodic counselling and education on coping skills in order to ensure optimum mental health in our adolescents.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent were received and obtained respectively before initiating the study from all participants.