
Abstract
Background:
The COVID-19 pandemic caused the long-term quarantine of most children and adolescents. Behavioral and psychiatric health issues with child protection need to be evaluated in disasters. The present study aimed to examine the behavioral and psychiatric status of children and adolescents during the pandemic to address the effects of the pandemic and isolation on children’s and adolescents’ behavioral and psychiatric health.
Methods:
The present cross-sectional study was carried out on 322 students aged 10–18 attending public high and elementary schools in Esfahan, Iran. The parents completed the Child Symptom Inventory-4 (CSI-4).
Results:
Findings showed that 58% of students met the criteria for all psychiatric symptoms except for autism and Asperger’s disorder, and 5% suffered from more than one comorbid category of psychiatric disorders. The most common psychiatric disorders in boys and girls were ADHD (18.5%), ODD (15%), ADHD-C (13.5%), GAD (12.8%), ADHD:HI (11.5), and MDD (10.8%).
Conclusions:
Since most participants suffered from at least one comorbid category of psychiatric disorders, developing a psychological crisis intervention is essential to protect children and adolescents from such disasters and minimize their mental health outcomes.
Background
Adolescence and childhood are the main stages of life because of the significant changes such as cognitive, physical, sexual, emotional, and social changes.1,2 Some big changes can bring mental health issues, such as anxiety and anticipation, for children, adolescents, and their families.2,3,4 Mental health conditions (eg, developmental disabilities, anxiety, childhood epilepsy, and depression) are the main determinants of health and major causes of disability and illness among children and adolescents.5,6 Therefore, understanding the needs at different stages of life can improve healthy development during childhood and throughout adolescence.7,8,9
The existing epidemiological studies showed that 10% to 20% of adolescents and children experience psychiatric and behavioral problems worldwide. 5 Fifty percent of all psychiatric and behavioral problems emerge by 14 years of age.10,11 In early life, exposure to risk factors can affect mental health and behavioral problems at the population level. Since December 2019, the new coronavirus (COVID-2019) has spread rapidly all over Iran and other countries in the world, causing an outbreak of acute infectious pneumonia. By January 2021, this pandemic killed 383,000 people worldwide. 12 This large-scale public health event brought not only the risk of mortality from the novel coronavirus but also tremendous psychological stress to people in Iran and the entire world 13 The continuous spread of strict isolation, lockdown, epidemics, and delays in colleges, universities, and schools is expected to have multiple consequences for children’s and adolescents’ behavioral and psychiatric health, such as acute and chronic stress, unexpected bereavements, overuse of the Internet and social media, extended home confinement, interfamilial violence, and brutal grief.12,13 Children and adolescents with psychiatric behavior problems are at risk of a change or break in management and care, and they may experience more intense symptoms.12,14,15,16
While several survey studies have recently addressed the negative psychological effects on health providers, patients, and older adults during the COVID-19 pandemic,15,17 there is still a lack of well-designed studies on the status of psychiatric and behavioral health conditions among Iranian children and adolescents facing this pandemic. Research on adolescent behavioral and psychiatric health conditions in times of isolation and lockdown is necessary, as a global pandemic could recur or be prolonged.15,18 According to the literature, assessing children and adolescents with externalizing and internalizing behavioral problems is critical to controlling and preventing these behaviors within a school context.12,13,15 Likewise, a better understanding of the current status of child and adolescent mental health problems in different settings (eg, community, school, families, and clinical services) helps policymakers develop public mental health services and infrastructure to meet youngsters’ and children’s needs.2,3
Therefore, the present study aimed to examine the behavioral and psychiatric status of children and adolescents during the pandemic. The findings may reveal the effects of the pandemics and isolation on children’s and adolescents’ behavioral and psychiatric health. The findings of this study are compared with the prevalence of psychiatric disorders in different studies conducted in Iran before the pandemic. This comparison is to some extent effective in explaining the differences due to the COVID-19 pandemic.
Methods
Sample Size Estimation and Sampling
The present analytical and cross-sectional study examined the mental health status of Iranian adolescents during the COVID-19 pandemic from November 2020 to January 2021. The participants comprised an independent sample, including 322 students aged 10 to 18 attending public schools in Esfahan, Iran. The students were categorized into two groups based on the type of school and education level. The first group belonged to the primary and middle education levels, for children or adolescents aged 7 to 11 years and 12 to 14 years, respectively. The second group was related to secondary education level for adolescents aged 15 to 18 years.
Students were included if they lived in Esfahan during the past nine months (the academic year in Iran) and if their parents consented to their participation in the study and had the appropriate physical conditions to complete all relevant questions. Participants were excluded if parents failed to provide an informed consent or if they suffered from a visual impairment or physical disability. In this study, assent was not obtained from students because it was a cross-sectional study. Students were not required to take any actions or practices. Likewise, the outcomes of this study that may benefit students are available in this research. The sample size was estimated using the following formula:
where the standard normal value (Z) was 5%, the accuracy (d) was 0.6, standard deviation was 4.31, and the margin of error was P <0.05. According to Heizomi et al 20 regarding mental health status in Iranian children and adolescents, the actual proportion of mental health status may not exceed 38%. Having adjusted for the attrition rate of 20%, 322 students were included in the sample size.
A cluster sampling with proportional allocation was used because the research population was composed of several subgroups (regions, sex, and age) that differed in number. In each subgroup, the number of participants was measured by their number relative to the entire population.
A total number of 12 schools were randomly selected from the public high and elementary schools in Isfahan. Initially, Esfahan was divided into three main clusters, namely, central, western, and eastern. Then, 12 schools were randomly selected from each main cluster, including 2 boys’ and 2 girls’ schools from each cluster. The first step was taken on a sample of 370 students selected proportionately to the number and sex of students in each grade. Then students in each grade were randomly selected based on a proportional allocation. Overall, 370 students were included, of whom 48 did not meet the inclusion criteria, or refused to participate. Finally, 322 students were included in the data analysis, and their parents completed the questionnaire in a written format. A copy of the demographic data questionnaire (sex, age, and living with parents) and the Child Symptom Inventory-4 (CSI-4), encoded in a closed envelope, was given to the students’ parents to fill out.
Measures
CSI-4 was a screening instrument for monitoring the most prevalent behavioral and emotional symptoms in adolescents and children, with two forms: teacher and parent report.21,22 The psychiatric symptom count procedure allows clinicians to recognize whether the adolescent or child is currently showing a sufficient number of psychiatric symptoms essential for a CSI-4 diagnosis. 23 The results showed that the parent checklist has more specificity and sensitivity than the teacher’s checklist. Therefore, we used the parent checklist, which included 17 categories of disorder symptoms and 110 items. 22 Although CSI-4 was used for less than 12 years, several studies used the instrument to monitor the most prevalent behavioral and emotional symptoms in adolescents and children, especially the parent version. 18 Furthermore, Hakimshooshtary et al 19 (2010) reported a high reliability (0.87) and high internal consistency (0.93 to 0.95) for the parents’ version in Iran for the 3 to 18 age group.23,24,25
This instrument was developed by Gadow and Sprafkin and consists of symptom classifications for the following Diagnostic and Statistical Manual of Mental Disorders (DSM-IV): attention deficit hyperactivity disorder, inattentive type (ADHD:I; 9 items); ADHD, hyperactive–impulsive (ADHD:HI; 9 items); oppositional defiant disorder (ODD: 8 items); ADHD, combined type (ADHD:C; 18 items); generalized anxiety disorder (GAD: 8 items); conduct disorder (CD: 15 items); separation anxiety disorder (SAD: 6 items); schizophrenia (5 items); dysthymic disorder (8 items); major depressive disorder (MDD: 10 items); social phobia (3 items); Asperger’s disorder (8 items); and autistic disorder (12 items). Likewise, this instrument contains single items to monitor for enuresis, encopresis, simple phobias, motor tics, vocal tics, obsessions, and compulsions. All items are scored on a two-degree scale ranging from 0 for “never/sometimes” to 1 for “often/very often,” indicating how often the disorder is observed. Esmaeil et al, tested the content validity and reliability of the parent form of the CSI-4 in Iranian children, and confirmed the sensitivity and specificity (Cronbach’s alpha: 0.78, CVI: 0.82, and CVR: 0.78). 26
Statistical Analyses
Data were analyzed in SPSS (Chicago, Illinois, version 16.0). Descriptive statistics were used to describe the respondents’ characteristics. An analysis of bivariate statistics was done to examine significant differences in disorders between different groups. A two-tailed P < 0.05 was considered statistically significant.
Ethics Approval and Consent to Participate
This study was approved by the research ethics committee of Mashhad University of Medical Sciences Research and adhered to the Helsinki Declaration in all phases of study. The participants were assured of the confidentiality of the information they provided. The study protocol was approved by the ethics committee of Mashhad University of Medical Sciences (#IR.MUMS.REC.1400.239) after gaining the required permission for the research. A written informed consent was obtained from the student’s parents. The data and materials will not be publicly open-accessed until the planned publication outputs are completed.
Results
Among a total of 322 students who were screened, 44.7% were female and 55.3% were male. The behavioral and psychiatric status of adolescents was determined based on the CSI-4 criteria. Table 1 shows the prevalence of psychiatric disorders and their differences in boys and girls. According to the CSI-4, autism and Asperger’s disorders were not diagnosed, while other disorders were diagnosed among the sample of students.
Distribution of Psychiatric Symptoms in Research Participants in Two Sex Groups.
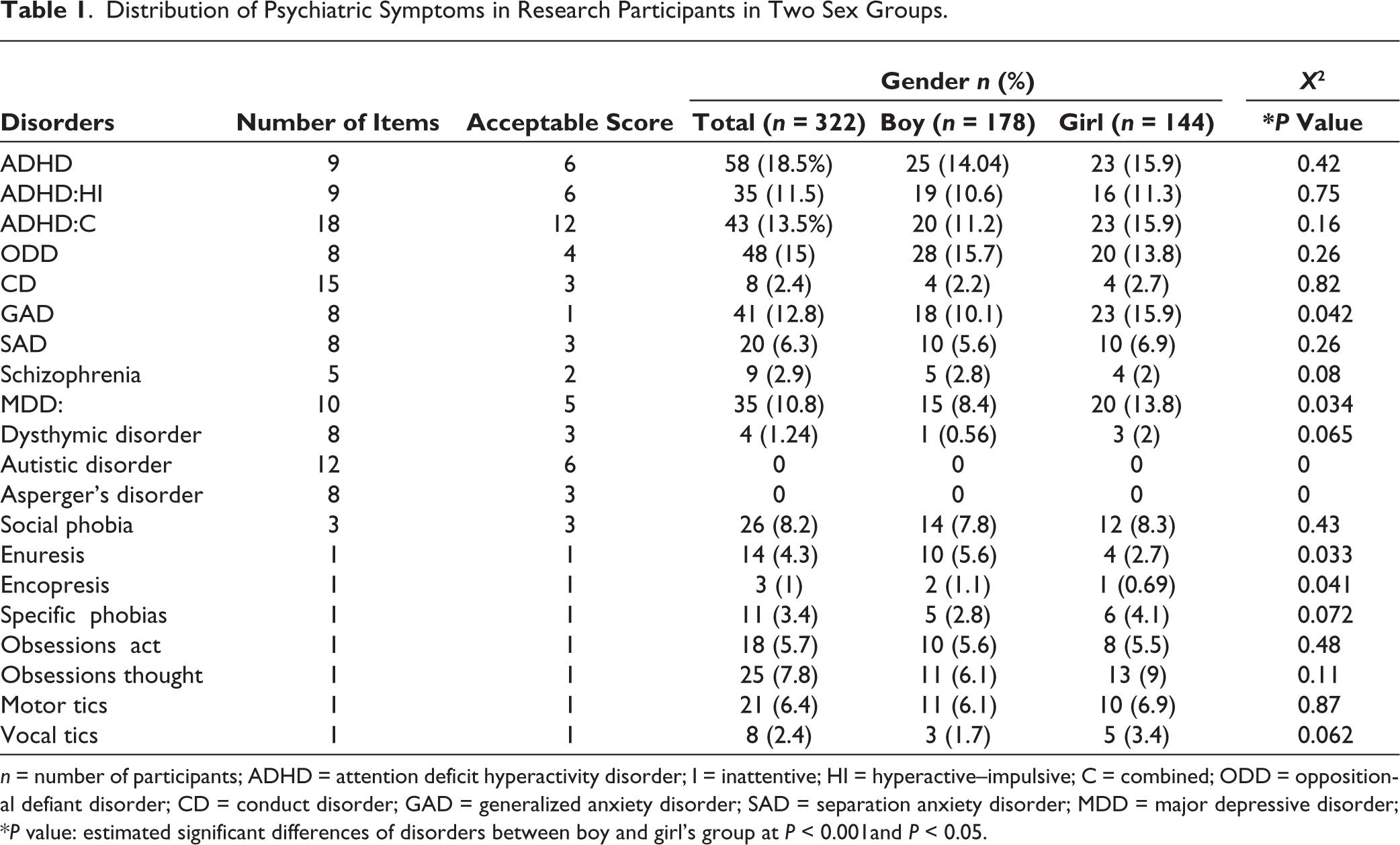
n = number of participants; ADHD = attention deficit hyperactivity disorder; I = inattentive; HI = hyperactive–impulsive; C = combined; ODD = oppositional defiant disorder; CD = conduct disorder; GAD = generalized anxiety disorder; SAD = separation anxiety disorder; MDD = major depressive disorder; *P value: estimated significant differences of disorders between boy and girl’s group at P < 0.001and P < 0.05.
The most common psychiatric disorders in boys and girls were ADHD (18.5%), ODD (15%), ADHD-C (13.5%), GAD (12.8%), ADHD:HI (11.5), and MDD (10.8%). The prevalence of other disorders in this study was lower than 10% among participants. As Figure 1 shows, 42% of students reported no symptoms, 18.5% suffered from one disorder, and 39.5 from more than one comorbid category of psychiatric disorders (Figure 1). There was a significant difference between boys and girls in terms of GAD (P = 0.042), MDD (P = 0.034), enuresis (P = 0.033), and encopresis (P = 0.041). In other words, the prevalence of GAD and MDD disorders in girls was much higher than boys, while the prevalence of enuresis and encopresis disorders in boys was significantly higher than girls. However, the prevalence of other disorders was not significantly different between the two sexes (Table 1).
Distribution of Comorbid Psychiatric Symptoms in Research Participants.
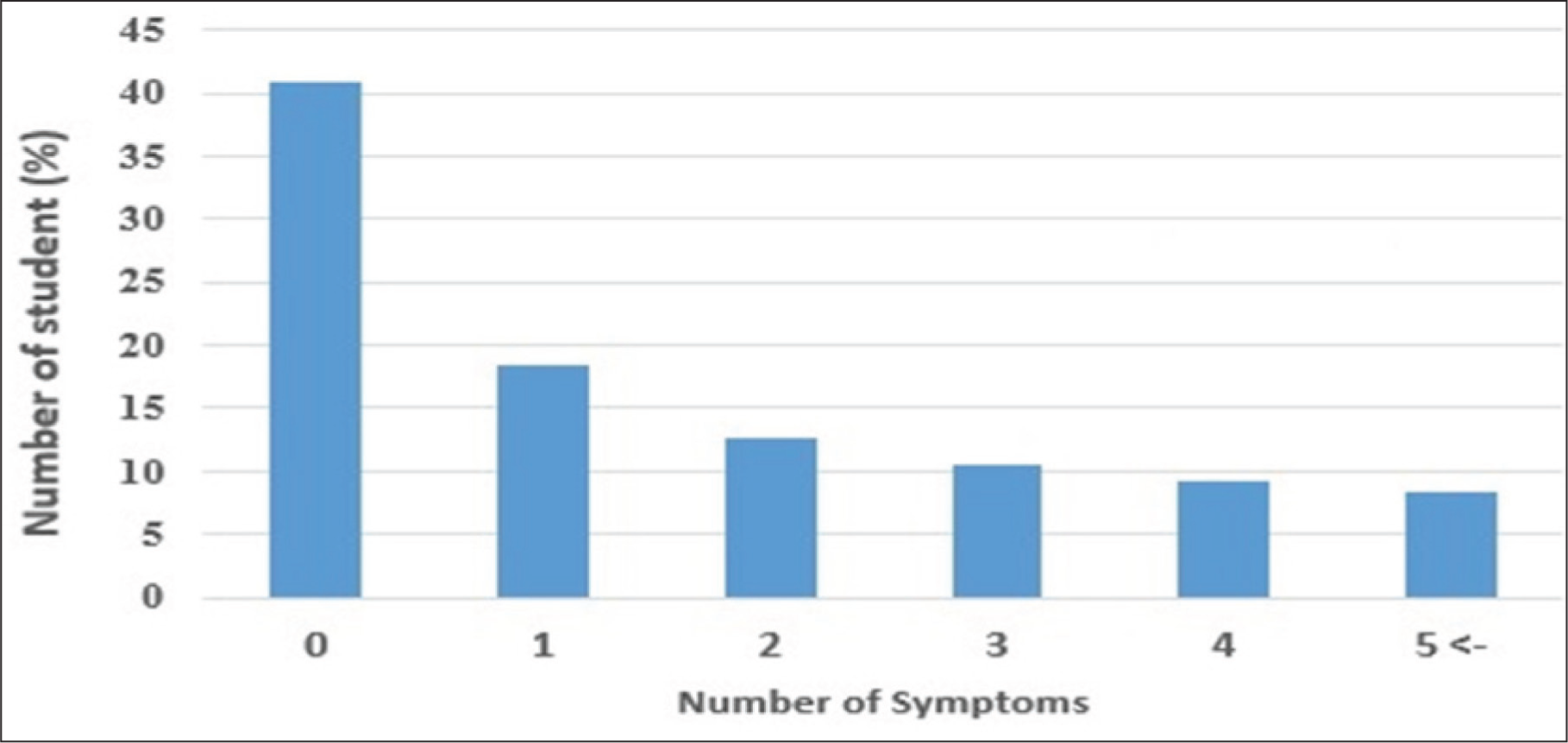
Table 2 shows the occurrence of psychiatric disorders and the differences in different age groups. The students’ mean age was 12.67 ± 3.8; 55.3% of the students were 10 to 14 years old, and 44.7% were 15 to 18 years old. As shown, the two most prevalent disorders in students aged 10 to 14 were related to ADHD, ADHD:HI, ADHD: C, ODD, and GAD. In students aged between 15 and 18, the most frequent disorders were related to ADHD, ODD, GAD, and MMD. There was a significant difference between these groups in terms of MDD (P = 0.041), enuresis (P = 0.023), and encopresis (P = 0.031). The prevalence of MDD disorders in students aged 15 to 18 years was much higher than students aged 10 to 14, while the prevalence of enuresis and encopresis disorders was significantly higher in students aged 10 to 14 compared to other students. Other psychiatric disorders were compared between the two age groups, and no statistically significant differences were observed (Table 2).
Distribution of Psychiatric Symptoms in Research Participants in Age Groups.
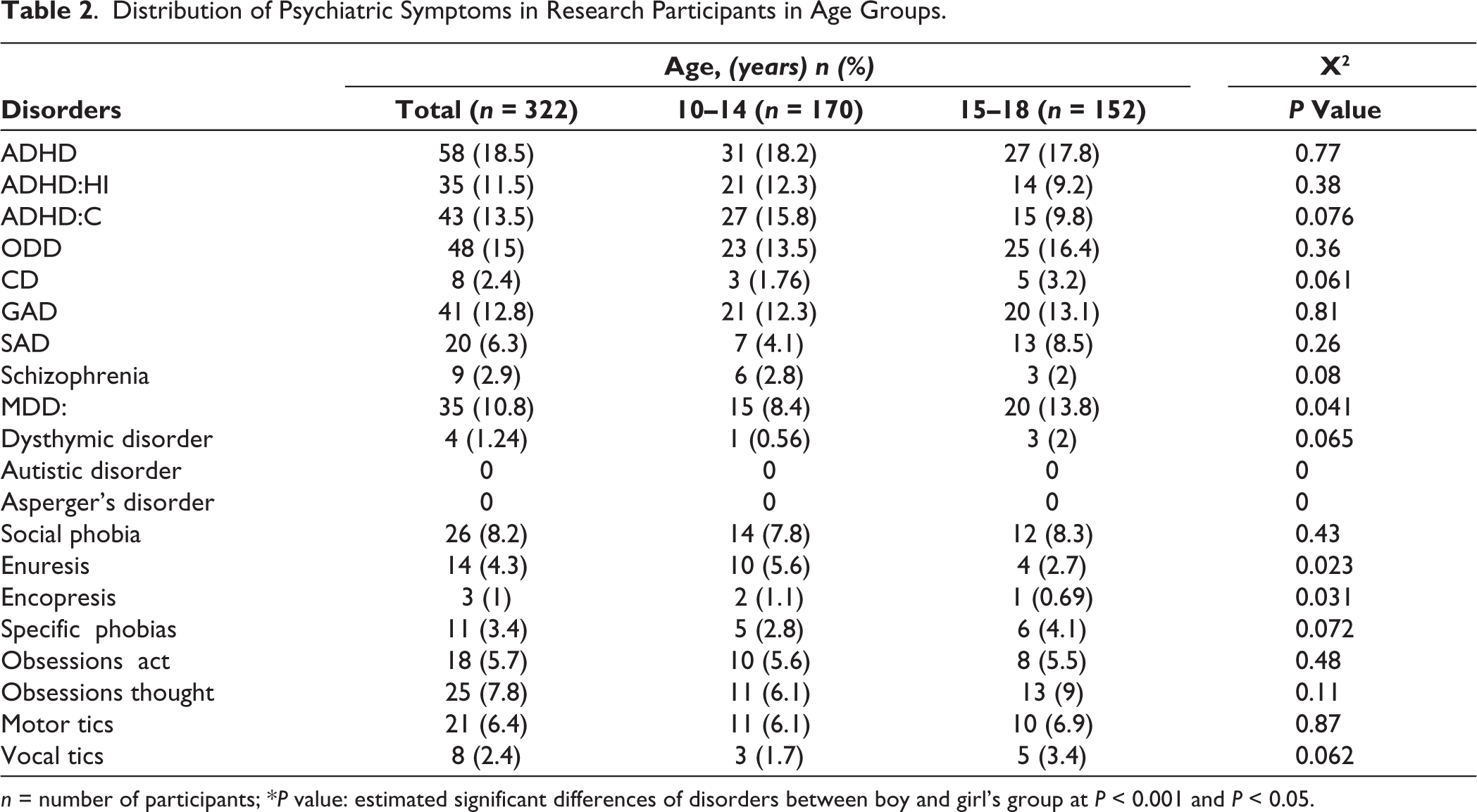
n = number of participants; *P value: estimated significant differences of disorders between boy and girl’s group at P < 0.001 and P < 0.05.
Table 3 shows the prevalence of psychiatric disorders in different studies conducted in Iran.
Distribution of Psychiatric Symptoms in Research Types Conducted on Iranian Children and Adolescents.
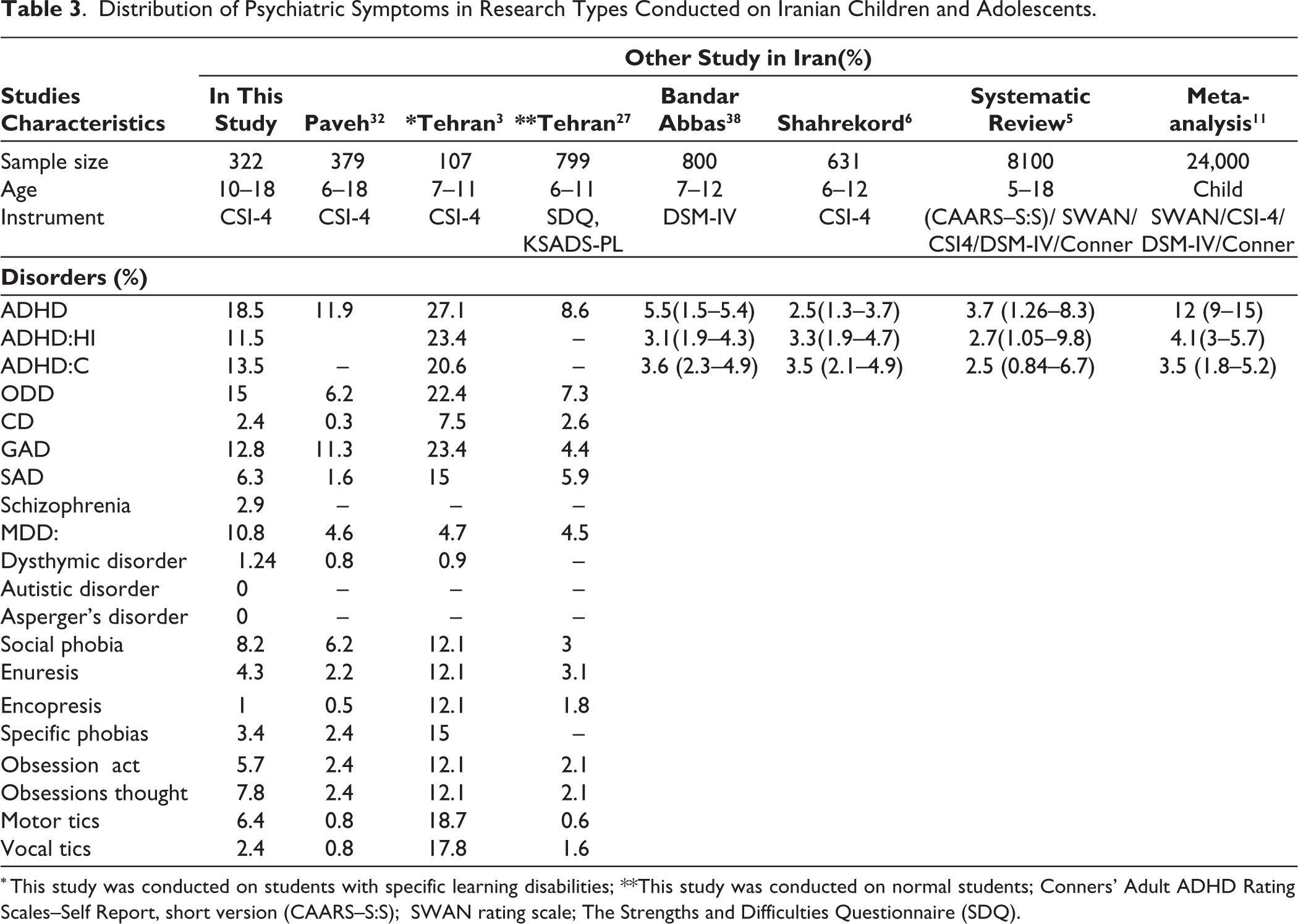
* This study was conducted on students with specific learning disabilities; **This study was conducted on normal students; Conners’ Adult ADHD Rating Scales–Self Report, short version (CAARS–S:S); SWAN rating scale; The Strengths and Difficulties Questionnaire (SDQ).
Seven studies examined the prevalence of psychiatric disorders in Iranian students from 2014 to 2019. However, two studies—systematic reviews and meta-analyses—were conducted to explore the prevalence of ADHD among Iranian students and adults. Likewise, only 3 studies reported the prevalence rates of all psychiatric disorders based on the CSI-4 in Iranian students, and other studies only examined the prevalence of ADHD, ADHD:HI, and ADHD:C. The total prevalence of all psychiatric symptoms in a body of research by Dodangi et al 23 in Paveh and Alavi et al 27 in Tehran was lower than the present finding. The trends for all symptoms were higher in the study of Karamali Esmaili et al 3 in Tehran in comparison with the present results. This could be explained by the type of research population that only included students with learning disabilities in Tehran. Likewise, the total prevalence of ADHD, ADHD:HI, and ADHD:C in the present study was also higher than other studies conducted in Iran from 1990 to 2016.
Discussion
Externalizing and internalizing behavior problems are known as the primary concerns in children and adolescents that influence their health, families, and society.28,29 Therefore, monitoring psychiatric symptoms based on valid scales and questionnaires is essential to the diagnosis of psychiatric health problems in adolescents’ lives, prevention of problems and difficulties in the future, and help individuals have a better lifestyle.1,30,31,11 The main aim of the present survey was to explore the frequency of psychiatric disorders in Iranian students during the COVID-19 pandemic.
The current study shows that 58% of students met the criteria for all psychiatric symptoms except autism and Asperger’s disorders, and 39.5% suffered from more than one comorbid category of psychiatric disorders. Several studies with different methods and instrumentations also reported the prevalence of comorbid psychiatric disorders in different regions of Iran.3,6,20,26 In Esmaili’s study, 82.8% of students with learning disabilities in Tehran were diagnosed with comorbid psychiatric disorders. 3 However, the overall frequency of comorbid psychiatric disorders in normal students in Tehran and Paveh (a western city in Iran) was estimated at 34% 32 and 27.8%, 27 respectively.
Iran is categorized as a low- and middle-income country, with 23.4 million people (31.1% of the total population) younger than 20 years of age.33,34 Although, therapeutic programs in different settings are available to manage chronic mental health problems for children, adolescents, and their families, child and adolescent psychiatric diseases are highly prevalent in Iran.34,35 According to the epidemiologic data, 16.7% to 36.4% of children and adolescents suffer from one or more psychiatric illnesses because of inappropriate public and private mental health services, educational support, and limited preventive services (such as health screening programs and interventions in early childhood).29,35 Although the Iranian government made many efforts to control the prevalence of coronaviruses, their focus was scarcely on the development of mental health services. A national survey in Iran during the COVID-19 pandemic found public mental health services (eg, health house clinics, hospitals, and telehealth resources) and private mental health services (eg, rapid transition to tele-psychiatry services and online counselling support) were not effective to enhance timely staffing and surge capacity to provide comprehensive mental care for the increased mental healthcare demands during the COVID-19 pandemic.36,37
Since most mental health issues emerge in childhood, educational support and mental health services are very important for students to treat mental diseases. 35 Likewise, the ongoing shifts in sociocultural behaviors and the rapid change in cultural and social context in Iran as a developing country could be the main factors that induce these psychiatric disorders.1,3 However, similar reports of the frequency of comorbid psychiatric symptoms in children and youngsters exist in studies worldwide. 10 In Chinese, American, and Indian adolescents, the frequency of behavioral problems was 10.5%, 21.9%, and 15.5%, respectively.5,15
Our findings revealed that, except for MDD, enuresis, encopresis, and GAD, the most common psychological disorders did not differ significantly across sexes or age groups among the students. Likewise, the findings revealed that the disorders of ADHD, ODD, ADHD-C, GAD, ADHD:HI, and MDD were the most common disorders in students. The disruptive behavior disorders (ADHD, ADHD:HI, and ADHD-C) in Iranian students have been previously discussed, and these studies confirmed the high rate of ADHD, ADHD:HI, and ADHD-C in Iranian students.3,20,26 Furthermore, two systematic and meta-analysis studies assessed the prevalence of ADHD, ADHD:HI, and ADHD-C in Iranian school-aged children and adolescents11,5. Their results showed that the total prevalence of ADHD was 3.17% in the study of Hakim et al and 12% 5 in the study of Yadegari et al. 11 Based on the biological setting and cultural context, social facility, the access rate to mental health services, and parent education and occupation showed that these differences were unacceptable.5,11
In this study, the overall frequency of all psychological disorders during the pandemic was higher than all the previous studies in Iran (Table 3). According to UNESCO surveys, 107 countries implemented school closures during the pandemic, affecting about 81.6% of the student population in the world at different levels of education. 35 There is research evidence that long-term closures have negative psychological effects on school-age children and adolescents, such as fear, anxiety, stress, hyperactivity, and depression.15,17 Students’ psychological disorders associated with COVID-19 could be due to the increasing social restrictions on individuals, sedentary lifestyle, fear of infecting family, cancellation of anticipated events, family financial loss due to lockdown, anxiety/stress/depression in parents, children’s awareness of COVID-19, parents’ intrusion and hyperarousal, and being a single child.12,13,37 Moreover, students’ mental health may be negatively affected by the suspension of semester-end final examinations, the shift of face-to-face classes to online, unavailability of computers, high-speed internet connections, and books at home.9,15 There is also evidence that school closures are the main reason for the increased psychological disorders in children and adolescents because of a lack of access to school services, such as physical activity in a natural environment, lunch, and counseling sessions.34,37 In a cross-cultural survey in Ireland and the United Kingdom, approximately 10,000 parents to children aged 4 to 18 reported substantial changes in the level of behavioral and psychological problems in their children during the lockdown. 37
Therefore, the COVID-19 pandemic can have both long-term and short-term consequences on adolescents and children’s mental health and well-being.36,37 This study attempts to provide data on the behavioral and psychiatric status of children and adolescents during the COVID-19 pandemic. Ongoing studies on evaluating indicators of adolescents and children’s mental health data, developing access to suitable mental health services, and promoting resilience and coping in adolescents and children are essential during the present pandemic or other similar conditions to support children’s well-being and stressors. It is also critical to train students on self-protection, develop effective educational interventions, and organize a psychological crisis intervention program to decrease the psychological effects of the COVID-19 pandemic.
It is notable that the limited available evidence reports specific interventions to improve mental health status among children and adolescents.34,37 Therefore, developing educational interventions specific to sex, age, and education level based on appropriate materials (comic books, videos, and infographics) and mental health-coping strategies can offer a unique solution to the improvement of the mental health status of children and adolescents. Because children and adolescents are well-informed, these modifiable strategies will be focused on worry, stress, and fear of the unknown. Research evidence shows that an intervention based on digital technology, a computerized self-help program based on cognitive behavioral therapy (CBT, BRAVE-TA, MoodGym, SPARX, and Think, Feel, and Do), and social networks are effective ways to help children and adolescents change their behavior and reappraise their thoughts within the confines of the home setting. Self-help interventions such as computerized therapy and bibliotherapy are also important to improve mental health among the young population.15,17
Limitations
The present findings are subject to several limitations. First, since a self-reported questionnaire based on parental reports has been used in this survey, the frequency of such symptoms in some samples could have been under- or over-diagnosed. A second limitation is that the present findings may not be generalizable to other countries because of cultural and social differences. Third, the physical risk factor, demographic factors (except age and sex), and teacher’s information were not examined, which biased in interpretations of present findings. Furthermore, making precise comparisons among studies is truly difficult because of the type of sampling and the assessment instruments and methods, which may influence the frequency of estimates.
Conclusion
To the best of our knowledge, the present study pioneers in documenting the frequency of psychiatric disorders in Iranian students during the COVID-19 pandemic in Esfahan, Iran, using CSI-4 criteria. Most students met criteria for all psychiatric symptoms except autism and Asperger’s disorders, and they suffered from more than one comorbid category of psychiatric disorders. The overall frequency of psychiatric disorders in students who participated in this study during the COVID-19 pandemic was higher than previous studies in Iran. ADHD, ODD, ADHD-C, GAD, ADHD-HI, and MDD were the most common disorders. The present findings suggest that educational and clinical attention be given to comorbid disorders, followed by psychosocial and pharmacological intervention programs integrated with educational strategies to reduce the psychological impact of the COVID-19 pandemic.
Footnotes
Acknowledgements
The authors wish to express their gratitude toward the vice president of research in Mashhad University of Medical Sciences.
Ethical Approval
This study was conducted after the approval and permission of Mashhad University of Medical Sciences Research Committee (IR.MUMS.REC.1400.239 at 2020/01/01) and was conducted with consideration of Helsinki Declaration in all phases of the study. Confidential data treatment was guaranteed. Written informed consent was obtained from the participants.
Declaration of Conflicting Interests
The authors declare that they have no competing interests.
Funding
The Mashhad University of Medical Sciences funded this project.