
Abstract
Purpose:
To develop and validate an oro-motor/sensory training module for addressing feeding challenges in preschool-aged children with autism spectrum disorder.
Method:
The present qualitative study was carried out in three phases: conceptualization, development, and validation of the oro-motor sensory training module. A total of 30 participants (15 speech language pathologists [SLPs] and 15 occupational therapists) treating children with autism spectrum disorders with a minimum of 5 years of experience validated the developed module. Descriptive and inferential statistics were done to see the reliability of the validation.
Results:
The overall rating of both groups of validators showed excellent reliability. Positive feedback was obtained for the module from the validators.
Conclusion:
The module can be a resource for SLPs and other professionals.
Introduction
Adequate nutrition during infancy and early childhood is critical for children’s health and development. The development and growth of an individual are heavily influenced by feeding behavior. Feeding is the act of eating, taking, or being given nourishment. It is heterogeneous, consisting of other complications like food aversions, selectivity, and partial to total food refusals. 1 Emotional development depends on feeding methods that are enjoyable and comfortable for both mother and child. 2 Concerning suitable feeding methods, the mother and family should be motivated, encouraged, informed, and supported.
Feeding behavior in children is influenced by various factors, including social, environmental, emotional, sensory-motor development, food type, and taste. 3 Feeding and swallowing problems are common in young children and infants, and about 80% of children with developmental disorders exhibit feeding and swallowing problems. 4 They develop exertion with feeding and swallowing from various medical conditions, congenital problems, or combinations of these factors.
Oro-motor skills are associated with the function of the lips, cheeks, jaw, and tongue, which play an essential role in a child’s speech and feeding development. Compared to other motor systems, oro-motor skills are more proactive (they respond to tactile stimulation as early as the seventh week of gestation) and not fine-tuned until the age of 6 or 7 years. 5 It comprises stabilizing the head and trunk in a sitting position with or without help and beginning motions with hand–eye coordination at the gross motor level. 6 Oro-motor and sensory deficits interfere with the sensory problems and motor movements affecting the lips, tongue, and jaw. Oro-motor problems are seen frequently in children with autism spectrum disorder (ASD). 7 The prevalence of feeding problems is greater than 90% in children with ASD. 8 Extreme food selectivity and refusals are problematic mealtime behaviors in children with ASD. These children have poor sensory and motor processing, which leads to eating disorders such as mechanical eating, food pocketing, scooping (shoveling), gulping, not chewing, throwing, spitting, or vomiting food, avoidance of specific utensils, and excessive rejections. Children with ASD also demonstrate oral sensitivity (oral hypersensitivity and hyposensitivity). Oro-motor and sensory deficits thereby affect swallowing and feeding in children. As feeding issues are one of the most critical concerns of the parents of these children, it is essential to combine both oral sensory and motor processing strategies and work hand in hand to improve the feeding and swallowing skills of children with ASD. Hence, improving oro-motor and sensory deficits is vital to improving overall feeding skills.
Oro-motor and sensory therapy use various strategies to facilitate awareness, strength, coordination, movement, and endurance of oral articulators (lips, tongue, cheek, and jaw), providing exercise to activate muscle function, stretching, providing sensory stimulation to each oral muscle, and stimulating the physiology of oropharyngeal mechanisms. Oro-motor treatment also enables jaw stability, extension, flexion, rotatory function, and improved range of motion. Oro-sensory treatment improves oral awareness and sensory integration by improving alertness before and after feeding, the child’s tolerance of minimal pressure, movement on the face, and touch response. It provides techniques to reduce oral aversion behaviors within and outside the oral cavity. It broadens the child’s food repertoire in terms of consistency, temperature, volume, and taste. It establishes feeding and drinking by altering feeding utensils. Effective intervention requires an understanding that the behavior of children with ASD is the outcome of a constellation of neurological abnormalities rather than deliberate acts of noncompliance. 9 Speech language pathologists (SLPs) must consider the unique and clinically specialized features of ASD while conducting assessments and interventions.
Although the variability of this population can make the clinical process more complex, it should motivate the SLPs to collaborate with other professionals so that the child with ASD can benefit from the collaborative team effort in the development of feeding skills. 9 As a result, this study focused on developing and validating an oro-motor/sensory training module for addressing feeding challenges in preschool-aged children with ASD.
Methods
The present qualitative study was conducted in three phases. The study protocol had undergone the required ethical procedures and was approved by the Institutional Ethics Committee on December 4, 2020 (reference no: 2212/IEC/2020).
Phase I: Conceptualization of the Module
In phase I, the domains or contents included in the oro-motor sensory intervention module were developed, focusing on feeding issues in children with ASD based on existing literature, practical knowledge, and experiences. The domains were chosen after a thorough conceptual and empirical evaluation and discussions with expert SLPs and occupational therapists (OT) using an unstructured facilitative approach. Experts were allowed flexible interaction with the researcher to obtain deep insights into the principles, opinions, observations, and practices of the oro-motor sensory intervention module, and data was documented. The identified domains and content were used to frame a checklist for content validation by experts in the field, which consisted of three sections:
Section 1: Oro-motor issues related to feeding problems in children with ASD, contains six domains with 29 items. Section 2: Oral sensory issues related to feeding problems in children with ASD, contains six domains with 15 items. Section 3: Indirect stimulation for feeding problems in children with ASD, contains eight items.
The checklist was validated using a 4-point Likert scale (zero indicating strongly disagree, one indicating disagree, two indicating agree, and three indicating strongly agree). The rating was based on the level of support for each domain relevant to oro-motor sensory issues associated with feeding problems in children with ASD. An open-ended question was also provided for the SLPs to give any suggestions or feedback that could be added to the module. The developed checklist was then given to five SLPs with at least 5 years of working experience in oro-motor sensory training related to feeding problems in children with ASD.
Phase II: Development of the Intervention Module
Based on the ratings and feedback obtained from the phase I content validation, the domains for the module were selected, and the module was prepared. The various steps involved in the development of the intervention module started with the outline of the manual, the development of the activities and material, reviewing the activities and items, conducting a task analysis, and the rearrangement of tasks based on the increasing complexity level. Based on the ratings provided by the SLPs, the essential tasks for oro-motor sensory intervention were selected and arranged in order of increasing complexity. The intervention module contained 10 chapters, which are as follows:
Introduction: a brief description of the overall development of feeding skills and oro-motor sensory development in typically developing children. Feeding issues in children with ASD. Assessment tools include the protocol for identifying the strengths and weaknesses of the child’s feeding abilities. General instruction for therapists and parents during feeding intervention. Prefeeding play activities for the child to get prior exposure to food items of different texture, color, and taste to improve their knowledge of food during play activities. General posture during feeding, depending on the child’s age, general development, and individual needs for comfortable seating during feeding. Indirect stimulation for feeding problems focuses on oral alertness, awareness, readiness, and responsiveness before oral feeding, improving feeding endurance for prolonged feeding, adaptation of food change during feeding, and oral aversion behaviors. Oral sensory activities for improving oral mechanism awareness, alertness, and tolerance before and after feeding (for hyper/hypo and mixed sensitivity), techniques for reducing feeding aversion, and improving food acceptance during feeding with instructions and illustrations. Oro-motor activities targeting tonicity (hyper/hypo and mixed tone), the motor ability of lips (oral awareness, lip seal, lip closure during swallow), tongue (tongue protrusion, retraction, lateralization), and jaw (oral awareness in jaw, jaw stability, jaw retraction, protrusion, grading, rotary chewing). Activities for establishing feeding and drinking by altering feeding utensils (spoons, cups) were also included. Activities to improve self-feeding, such as fine motor skills, meaningful interaction with caregivers, improving culturally appropriate social routines for mealtimes, and experiencing new sensations, including different textures and temperatures. Additional activities for children with ASD exhibiting food selectivity, food preferences, repetitive neophobia, drooling, gulping, choking, and improving mealtime routine. The appendix contains materials that can be used during feeding therapy, an assessment protocol, data sheets for tracking mealtime behaviors in the child, data sheets for recording food preferences, and an oral hypersensitivity scale. Additional resources for therapists have been listed, which can be recommended to the parents.
The resources for the module were chosen based on the applicability, validity, and feasibility of activities with children with ASD. All the tasks and activities were given out in a way that the therapists could understand the aim of working on the specific domains, the rationale for the goal, and the materials that could be used, as well as other materials that could be useful and viable for the Indian population based on familiarity, cultural context, and the use of objects in everyday life.
Phase III: Validation of the Developed Intervention Module
The developed intervention module was then subjected to content validation to ascertain its feasibility. A total of 30 experts (15 OTs and 15 SLPs) currently treating children with ASD were considered for the content validation. A convenience snowball sampling method was used for the selection of validators. The following inclusion criteria were used for the selection.
SLPs and OTs with at least 5 years of work experience treating oro-motor and sensory problems in children with ASD.
SLPs and OTs with additional oro-motor/sensory or feeding intervention training.
For the content validation, an evaluation form was developed, which consisted of two sections: Section I contains 30 questions under three subsections: (a) content, (b) production quality, and (c) possible benefits. The questions in the sub-section (a) were based on understandability, accuracy, update, technical terms, clarity, usage of the manual without a facilitator, simplicity, adequate instructions, accurate techniques, usage of vocabulary, target population, bias-free, respect for race and culture, and scope of information. Under subsection (b), questions were based on creativity and originality, appropriate props, quality, phase, the transition of each frame, sections in the module, titles, legibility, professionalism, organization, and structure. Subsection (c) was based on the necessity of modules, usage, resource material for non-SLPs, newly acquired knowledge, relevancy after 5 years, and training for SLPs.
Section II contains four open-ended and closed-ended questions for obtaining an overall impression of the module. It included questions related to the highlights, suggestions, and overall impression of the module. A 4-point Likert rating scale (0-strongly disagree, 1-disagree, 2-agree, and 3-strongly disagree) was used for rating the checklist. Modifications in the module were based on the ratings and suggestions the SLPs and OTs provided.
Statistical Analysis
Statistical analysis was done using SPSS software version 23. Descriptive statistics of mean and SDs were calculated for the ratings obtained from SLPs and OTs. Also, Cronbach’s alpha test was used to determine the reliability of the ratings. In addition, the relationship between ratings of SLPs and OTs for each question was calculated using the Chi-square test.
Results
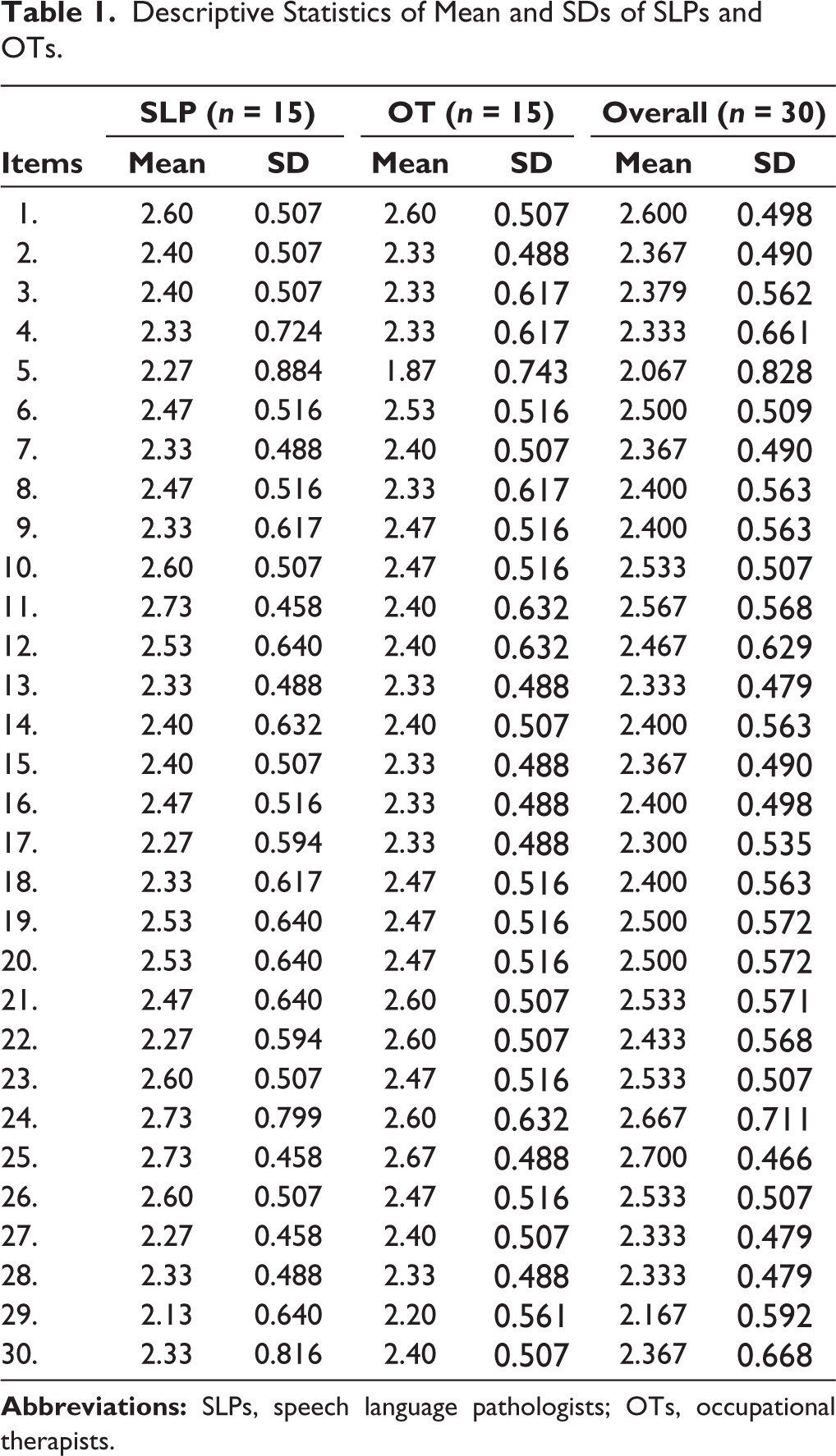
The mean and SD for SLPs (n = 15) and OTs (n = 15) for 30 questions showed ratings ranging from agree to strongly agree. Similarly, the overall mean and SD for both SLPs and OTs (n = 30) for 30 questions ranged from agree to strongly agree (see Table 1).
Descriptive Statistics of Mean and SDs of SLPs and OTs.
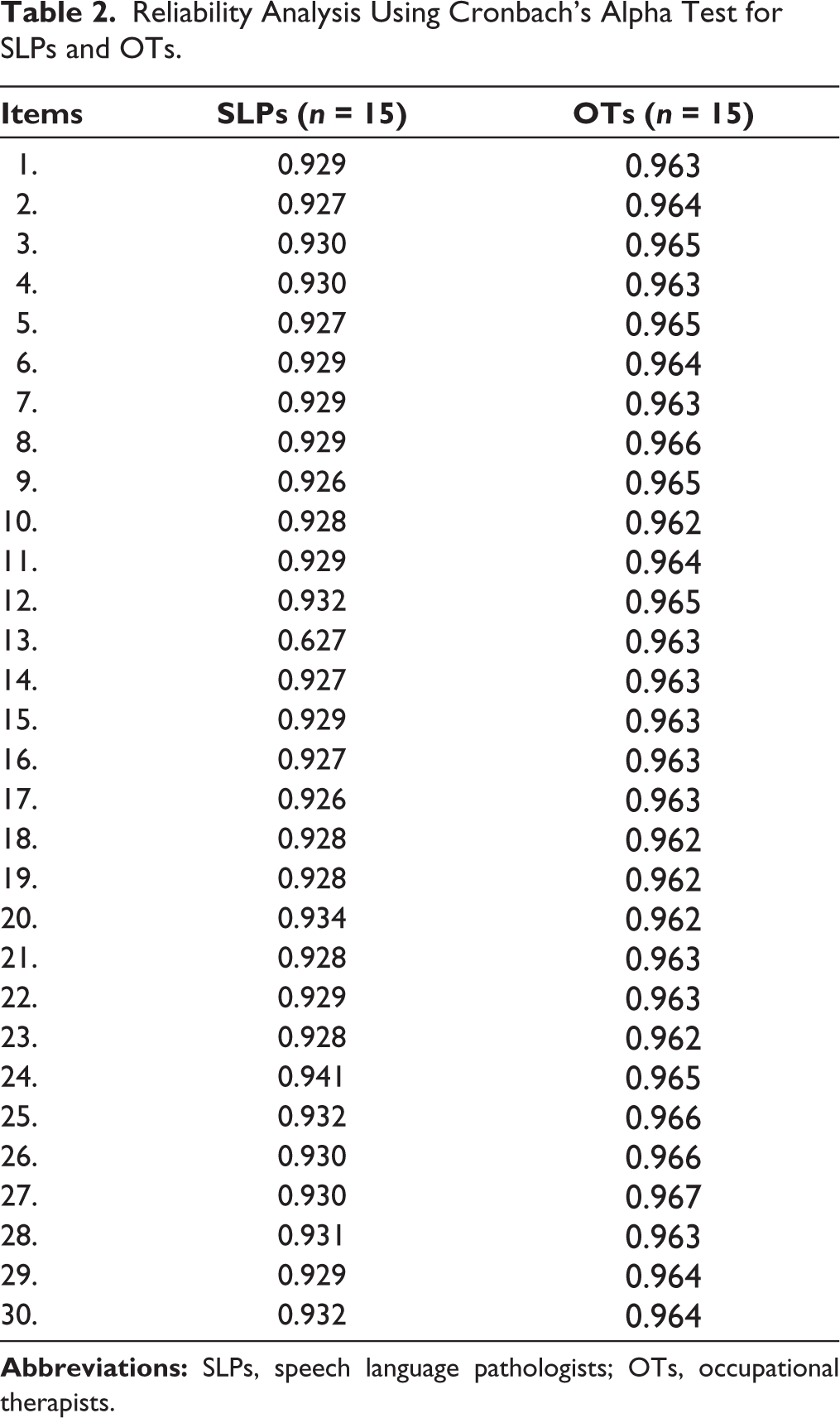
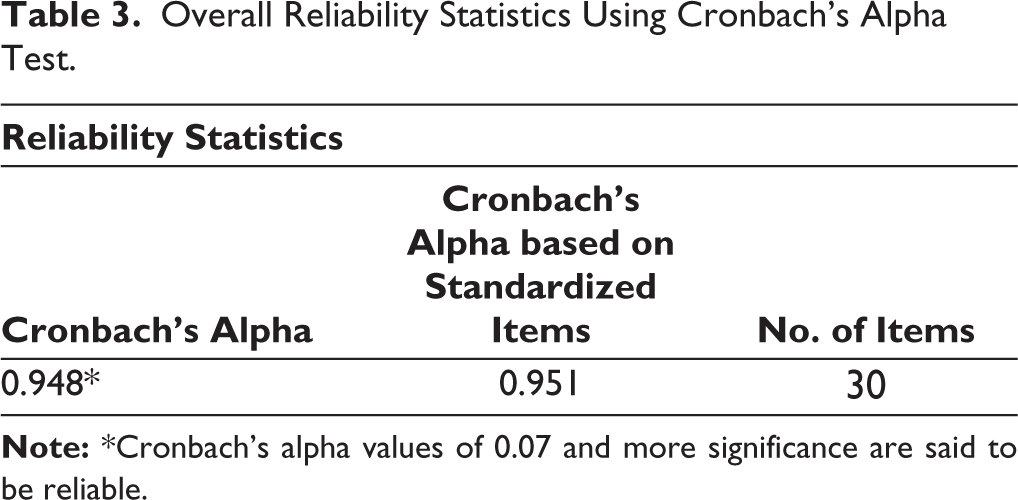
The Cronbach’s alpha for SLPs (n = 15) and OTs (n = 15) for 30 questions ranged above 0.70 (see Table 2). The overall reliability between SLPs and OTs was 0.948, which shows excellent reliability (see Table 3).
Reliability Analysis Using Cronbach’s Alpha Test for SLPs and OTs.
Overall Reliability Statistics Using Cronbach’s Alpha Test.
Discussion
A child’s behavior around food and feeding activities impacts his or her dietary intake, nutritional status, and growth. In the early stages of development, children with ASD are diagnosed with sensory processing disorders and motor impairments related to feeding. Various elements influence these children’s proper eating development. Understanding these children’s oral sensory and motor issues is crucial to designing appropriate intervention approaches and specific goals that lead to a better prognosis. 10 A treatment program should be facilitated by using a combination of both motor and sensory approaches that are suitable for the natural environment and maintaining techniques to enable the child’s self-feeding skills.
Careful manipulation of food, mealtime environment, and nutrient content of the diet has shown successful results in food acceptance (new foods). Despite the widespread use of behavioral and sensory integration strategies in therapeutic settings, there still needs to be more research with sufficient controls to back up anecdotal findings. 11 As a result, the current study aimed to create a module focusing on intervention for oro-motor sensory, and other feeding problems in children with ASD.
The developed module contained information regarding feeding, oro-motor sensory development in typically developing children, and oro-motor/sensory therapeutic strategies. It also focused on the assessment protocol and inventories to understand the parent’s perspective on feeding issues exhibited by these children and pre-feeding play activities, which will be helpful for the child to explore food before meal time. The goal, rationale, and activities for oral sensory and motor problems, indirect stimulation of feeding, and data sheets (Mealtime Behavior Data Sheet and Food Preference Data Sheet) are provided that can be used for monitoring progress, documentation of mealtime behaviors and food preferences, and appropriate pictures with general instructions to be followed were given. The validators provided positive feedback regarding the module’s content, feasibility, adaptability, and usage. However, it was suggested to mention the risks and precautions to be considered during feeding therapy and to include chapters for parents and caregivers.
Two significant oro-motor sensory challenges accompanying ASD include speech disorders and feeding problems. Children with ASD exhibit unusual feeding behaviors related to oral sensitivity and psychological or emotional behavior toward food, leading to nutritional deficiency. Several studies have identified feeding issues with ASD children regarding drooling, limited food selection based on color, texture, consistency, smell, and intestinal problems. Hence, there is a significant need for oral stimulation targeting the articulating surface of the speech element, increasing muscle coordination, gratifying sensory demands, or lessening sensory overload, which may control feeding and eating behavior. 12 Hence, oro-motor sensory stimulation may assist in the advancement of both speech and feeding issues in ASD children. Therefore, the current organized stepwise graded module was developed to benefit therapists in assessing, setting goals, and identifying activities to support feeding problems in children with ASD. This module also provides a better means to document the progress.
Conclusion
The current study has provided a content-validated oro-motor/sensory module. The study highlighted the need for intervention for oro-motor sensory skills related to feeding problems in children with ASD. The module can be a resource material for SLPs and other professionals.
Future Direction
The developed module is in the process of efficacy testing using randomized control trials with objective outcome measures on children with ASD with feeding issues.
Footnotes
Acknowledgements
We are grateful to the Dean of Medical and Dr. Savitha V. H., Professor and In-charge Head of Audiology and Speech-Language Pathology, for their support in accomplishing this study. We also extend our gratitude to all the validators of the study.
Authors’ Contributions
All three authors contributed substantially to the conception and design of the study, data interpretation, and manuscript drafting. The first author was responsible for data acquisition and analysis. The second and third authors contributed significantly to concept formation, manuscript preparation, the review process, data analysis, and interpretation. All of us agree and approve the final manuscript being submitted.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Informed Consent and Ethical Approval
The study was accorded Ethical Committee Approval vide Institutional Ethics Committee SRM Medical College Hospital and Research Centre, SRMIST, Kattankulathur, with the reference No. 2212/IEC/2020 dated on 04.12.2020.
Verbal Informed Consent was taken from all the participants. The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki.