
Abstract
Background:
Nephrotic syndrome (NS) is one of the most commonly diagnosed kidney diseases in childhood, with a high relapse rate.
Aim:
This study was designed to assess emotional and behavioural problems, temperament, family environment, and evaluate the health-related quality of life in children with NS.
Methods:
This cross-sectional study was conducted at a tertiary care hospital in South India. A purposive sampling technique was used. A sample of 32 children between ages 6 and 12 years with NS—steroid-sensitive (infrequent relapsers, frequent relapsers, or those with steroid-dependent) and steroid-resistant—for more than 6 months duration and managed by the Pediatric Nephrology department were recruited. The control group of 30 healthy children was matched for age and gender. The assessment was conducted using the Strengths and Difficulties Questionnaire (SDQ), Pediatric Quality of Life Inventory™ (PedsQL 4.0), Malhotra Temperament Schedule, and Family Environment Scale. Data obtained was examined using descriptive and inferential statistics.
Results:
On the SDQ, 34.4% of children with NS indicated a total score within the clinical range. Children with NS had an overall lower score on the QOL scale (P < .003). It was found that the SRNS subtype had poor scores on SDQ (P < .023) and QOL (P < .017). The temperament of children with NS did not differ from those of healthy children. The families with NS scored lower on organization (P < .042) and control (P < .006) subscales.
Conclusion:
Children with NS have a risk of emotional and behavioural problems. It appears that children with NS have a poor quality of life. Families of children with NS were less organized and low in control. Findings indicate the need for routine psychological evaluation and intervention as they will impact the course and outcome of NS.
Keywords
Introduction
Nephrotic syndrome (NS) is a kidney disease commonly seen among children and can affect children from infancy to adolescence. 1 NS is characterized by proteinuria, hypoalbuminemia, and oedema. 2 The condition has a prevalence of 16 per 100,000 children, 3 with higher rates reported among South Asian and African ancestry.4–6
The primary treatment for NS is corticosteroids. Idiopathic NS is categorized by resolution of proteinuria (attaining remission) with steroid therapy as steroid sensitive (SS) or steroid resistant (SR). 2 NS is characterized by a relapsing course (triggered by infection) requiring reinitiation of steroid therapy. Most children with NS are steroid sensitive and respond well to steroid therapy (85%-90%); however, approximately half the children (50%) become frequent relapsers or steroid dependent.7, 8 SS NS (SSNS) has a high chance of longer remission with preserved renal function.7, 9, 10 Around 10% to 15% of children do not achieve a complete remission with steroids alone and are SR. 11 SR NS has a considerably poorer prognosis than SSNS and often results in chronic kidney disease or kidney failure.12–14
There is a risk of developing complications such as infections, thrombosis, episodes of acute kidney infections, dyslipidemia and oedema, often requiring hospital admissions. 1 Steroid therapy results in cushingoid appearance and weight gain. Long-term use and high doses of steroids may lead to growth retardation, obesity, hypertension, cataracts, and bone demineralization. 14
Behavioural changes in children with NS due to steroid therapy have been reported.15, 16 One study has shown that the prevalence of behavior disturbance in children with NS is higher (68%) as compared to healthy children (21.6%). 17 Studies indicate that in NS, children experience emotional and behavioural problems such as anxiety, withdrawn behavior, somatic complaints, hyperactivity, increased aggression, peer relationship, and poor school performance.15, 18–21
Other illness-related factors such as duration with NS, frequency of relapses, number of days on steroids and dose of steroids, immunosuppressive medication, hospital visit, and admission may impact the child’s overall quality of life.22, 23 The negative impact of health-related quality of life (HRQOL) or psychosocial adjustment in this condition has been documented.24–26 All children with NS receive steroids at diagnosis; therefore, it is hard to distinguish whether the effect on psychological well-being is due to the treatment process or the disease itself. 27
Temperament is a stable characteristic from birth and may also play a role in psychosocial outcomes. 28 Some early studies have reported that children with physical illness tend to have more challenging temperaments29, 30 and how understanding temperament can guide children’s treatment. 31 Additionally, parents’ daily routines may get disturbed because of repeated hospital visits, school absenteeism, and the cost of treatment, all having implications on parental and family functioning.32–34
The socioeconomic and cultural backgrounds in which children are brought up, religious affiliation, parenting styles, communication, families’ styles of coping, perception of health and treatment could have an implication on a child’s psychological functioning and quality of life.35, 36 Psychosocial problems are most likely to attain importance during unpredictable changes in physical health, 37 and treatment variables could also influence a child’s psychosocial issues. Various studies in children with NS have focused on behavioural issues and the impact of the illness on the quality of life. Parents express concerns about their child’s physical changes in clinical practice, such as weight gain and swelling. The visit to the hospital, the requirement to take medications, dietary changes, and changes in daily activities, including schooling and illness-related uncertainty, may impact children’s emotions and behavior, self-esteem and peer relationships. 27 In addition, factors such as a child’s temperamental style and family environment could also influence behaviors and the treatment process. Therefore, our study aims to understand the psychosocial functioning of children with NS. We looked into the children’s emotions, behaviors and overall HRQOL. We examined the temperament of the children and their family environment. We also tried to see the association, if any, between behavioral problems and clinical characteristics. Thus, efforts to look at the psychosocial issues of these children help in early identification and intervention that will lead to better outcomes.
Methodology
Study Design and Participants
The study is a cross-sectional study conducted in the outpatient clinic at a tertiary care hospital in South India. The sampling technique used was purposive sampling. A clinical group of 32 children with NS between 6 and 12 years of age— steroid-sensitive (infrequent relapsers, frequent relapsers, or those with steroid-dependent) and SR—for more than 6 months duration and managed by the Pediatric Nephrology department were recruited from OP care. Children with global developmental delays or other medical, neurological, or psychiatric illnesses were excluded. The control group of 30 healthy children without global developmental delay or suffering from medical or psychiatric condition were recruited from the community using convenient sampling. It matched the clinical group based on their age and gender.
Measures
The sociodemographic and clinical details were collected using a semi-structured pro forma developed for the study and chart review.
Ravens Coloured Progressive Matrices (CPM) 38 and Standard Progressive Matrices (SPM) 39 measure nonverbal intellectual functioning and rule out children with intellectual disabilities. Children above 11.11 years were administered the SPM.
Strengths and Difficulties Questionnaire (SDQ). 40 It is a short behavioral screening questionnaire for children aged 3 to 16, consisting of 25 items and 5 subscales measuring emotional symptoms, conduct disorder, hyperactivity, peer problems, and prosocial behavior. Items are rated on a 3-point scale ranging from 0 (not true) to 2 (certainly true). Combining the first 4 subscales gives a total difficulties score (ranging from 0 to 40), indicating psychosocial problems. The parent version of the SDQ was used for this study.
The Pediatric Quality of Life Inventory™ generic core scale (PedsQL 4.0) 41 was used to evaluate HRQOL in children. It is composed of 23 items that measure physical (8 items), emotional (5 items), social (5 items), and school (5 items). Parents report children’s functions on a 5-point scale ranging from 0 to 4. The responses are reverse scored and linearly transformed to a 0 to 100 scale. The higher the score, the better the quality of life. The physical functioning scale is the same as the total physical score. The total psychosocial score is a computed mean of the emotional, social, and school functioning subscales. In addition, the computed mean of the emotional, social, school functioning, and physical scales gives a total summary score. The parent proxy report was used for the study.
Malhotra Temperament Schedule (MTS) 42 is an Indian adaptation of Thomas and Chess’s temperament questionnaire. It measures 5 temperament dimensions: sociability, emotionality, energy, distractibility, and rhythmicity. Each dimension consists of 5 items that explore the child’s routine activities. The items are rated on a 5-point Likert scale. Scores of 1 and 2 indicate lower, 3 indicates average, and 4 and 5 are higher than average frequency and intensity of the concerning behavior. The mean score in each temperament dimension is used for analysis.
Family Environment Scale (FES) 43 is an Indian adaptation of Moss and Moss’s FES, consisting of 69 items, 3 dimensions, and 8 subscales. The relationship dimension consists of 4 subscales—cohesion, expressiveness, conflict, and acceptance and caring. The personal growth dimension includes 2 subscales of independence and active recreational orientation. The dimension of system maintenance includes 2 subscales of organization and control. Each subscale has many positive and negative statements. There are 5 responses to each statement: strongly agree, agree, neutral, disagree, and strongly disagree. All positive items are scored as 5, 4, 3, 2, 1 and negative items are in reverse order.
Procedure
The study was undertaken after obtaining institutional ethics approval. Data for the clinical group were collected from June 2019 to November 2019 at the Pediatric Nephrology clinic. After obtaining consent from the treating Pediatric Nephrologist, children who met the inclusion-exclusion criteria were recruited and explained the nature of the study, confidentiality, and the right to withdraw. Written informed consent was taken from parents and informed assent was obtained from children. No incentives were provided for participating in the study.
In the first meeting, the researcher focused on building rapport with each child. The timing for the research assessment was coordinated so that their appointment with the treating team remained undisturbed. A brief evaluation was carried out with either of the parents regarding the child’s birth and developmental history. Then, the CPM or SPM was administered depending on the child’s age. Further assessments were carried out if the score was within the normal range (25th percentile). The PedsQL, SDQ, MTS and FES were administered to the parent (either father or mother, present at the evaluation). The assessment was done individually on the parent and child. The time taken for evaluation was 2 hours. A total of 8 families from the clinical group declined participation—the reason for not participating included lack of time and discomfort in completing psychological surveys.
Data for the control group were also collected during the same time frame. Children were identified from the community. Parents and children were explained about the study. Written consent was taken, and informed assent was obtained. An appointment was fixed for the evaluation. Developmental history was obtained from the parents, followed by administering the tools. In this group, 2 families refused participation stating time constraints.
Data Analysis
Descriptive statistics such as mean, median, standard deviation, range, frequency, and percentages were calculated for data obtained from sociodemographic and clinical datasheets and the assessment tools’ scores. The chi-square test or Fisher exact was done to compare the potential association between categorical variables. Student t-test was used to analyze the statistical difference between the 2 groups. Kruskal-Wallis test was used to analyze statistical differences between 3 or more groups for nonparametric data. Pearson’s correlation was applied to see the association between psychological and clinical variables. Statistically significant values were reported for P values less than or equal to .05, and P values less than .01 were considered very significant. The data were analyzed using IBM SPSS statistics (version 22.0. Armonk, NY: IBM Corp).
Results
Sociodemographic Profile
The clinical group consisted of a majority of males (n = 23, 71.9%) from nuclear families (n =22, 68.8%) and hailing from the urban background (n = 26, 81.3%). Their mean (±SD) age at evaluation was 8.91 (± 2.19) years. The mean (± SD) number of years of schooling was 5.34 (± 2.09). 17 (53.1%) families belonged to modified Kuppuswamy’s 44 lower-middle socioeconomic status, 7 (21.9%) belonged to upper-lower, and 2 (6.3%) belonged to lower socioeconomic status, whereas 5 (15.6%) and 1 (3.1%) belonged to upper-middle and upper socioeconomic status.
In the control group, half of the sample (50%) was male, from nuclear families (n = 26, 83.3%) and all (100%) belonged to the urban background. The mean (± SD) age at the time of evaluation was 9.29 (±2.21) years. The mean (± SD) years of schooling were 5.62 (± 2.08). A total of 13 (43.3%) families belonged to lower-middle socioeconomic status. More than half belonged to upper-middle and upper socioeconomic status (13% and 43.3%).
Clinical Characteristics
Clinical characteristics were assessed by collecting information from parents and reviewing case files and treatment details (Table 1).
Clinical Characteristics of Cases with Nephrotic Syndrome (N = 32).
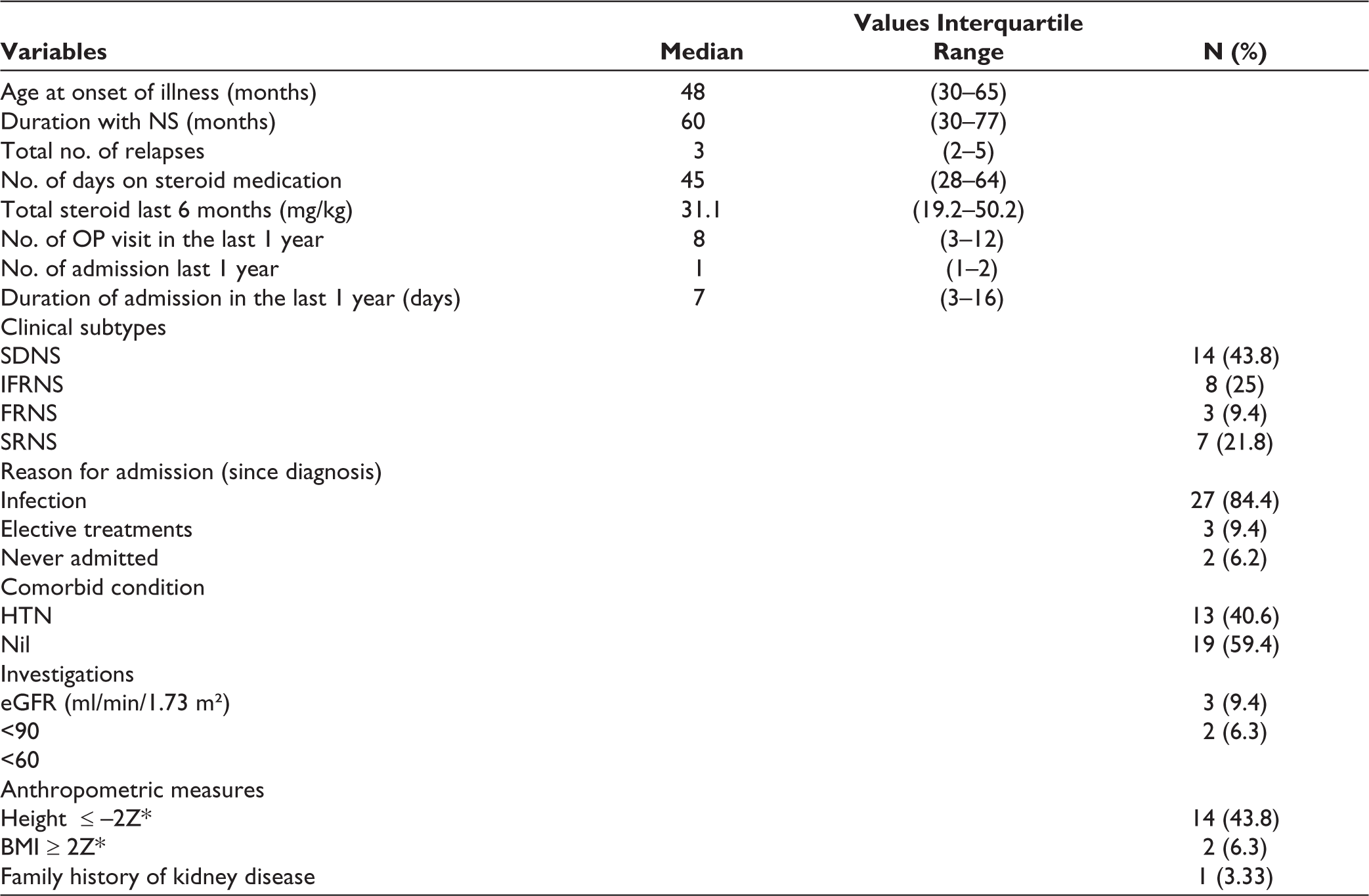
Abbreviations: SDNS, Steroid Dependent Nephrotic Syndrome; IFRNS, Infrequent Relapse Nephrotic Syndrome; FRNS, Frequent Relapse Nephrotic Syndrome; SRNS, Steroid Resistant Nephrotic Syndrome; HTN, hypertension; eGFR, estimated glomerular filtration rate; BMI, body mass index.
Emotional and Behavioural Problems
Table 2 indicates significant differences between children with NS and healthy children on the total difficulties score (P < .01) of SDQ and its subscales, emotional disorder (P < .005), conduct disorder (P < .003), and prosocial (P < .02). A higher percentage of children in the NS group fall under the abnormal category in total difficulties score (34.4%), emotional problem (28.1%), conduct problem (37.5%), and prosocial (21.9%) when compared to the healthy group total difficulties score (26.7%), emotional problem (20%), conduct problem (6.7%), and prosocial (0%).
Differences in Emotional and Behavioural Problems Between Children with NS and Healthy Children.

*P ≤ .05 considered significant.
The severity of emotional and behavioural problems was categorized based on the SDQ cut-off scores.
Quality of Life
There was a significant difference between the 2 groups in quality of life. On the PedsQL, for the physical dimension, the mean (±SD) for children with NS was 68.26(±19.94), and for the healthy children, it was 81.25 (±18.40) (t = –2.66, P < .010). On the psychosocial dimension, the mean (±SD) for children with NS was 65.52 (±14.72) vs 74.88 (±12.95) for healthy children (t = –2.65, P < .010). The mean (±SD) of the total score for children with NS was 66.47(±14.39) and 77.10 (±12.35) for the healthy children (t = –3.12, P < .003).
Temperament
Table 3 shows no significant differences concerning temperament between children with NS and healthy children.
Differences in Temperament Between Children with Nephrotic Syndrome and Healthy Children.

P ≤ .05 considered significant.
Family Environment
Table 4 shows the different subscales of family environment where significant differences between families of children with NS and healthy children are only in organization (P < .042) and control (P < .006).
Differences in Family Environment Between Children with NS and Healthy Children.
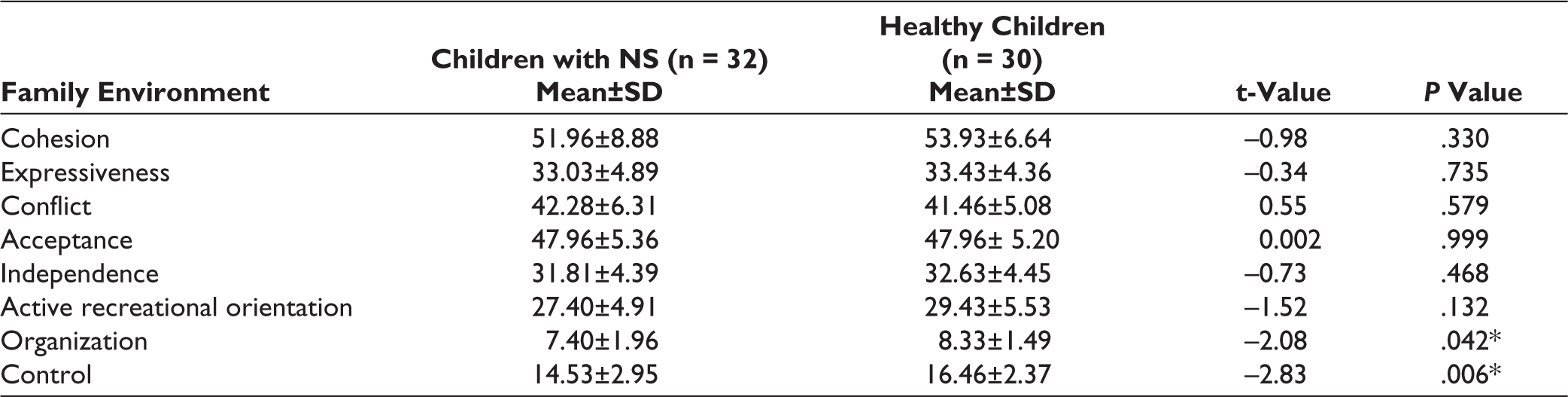
*P ≤ .05 considered significant.
Association Between Psychosocial Factors and Clinical Characteristics
The effects of clinical variables (gender, onset of illness, duration with NS, types of NS, dosage of steroid, total number of relapses, and number of admissions) on emotions and behavioural problems, quality of life, temperament, and family environment were examined. We found that children in the SRNS group had a higher clinical and borderline range for emotional and behavioral problems as indicated on the SDQ (P value < .023) and had lower scores on the QOL physical domain as compared to other NS groups (P < .017). On the TMS, rhythmicity was associated negatively with the frequency of relapse (r = –0.386, P < .029), and hospital stay (r = –0.350, P < .049). On the FES, a negative association was seen between the family organization with the age of onset (r = –0.430, P < .014); however, the total dose of steroids was positively associated (r = 0.548, P < .001). No significant findings were found between other psychosocial outcomes and clinical variables.
Discussion
More than half the children with NS were boys in the present study. The pattern of representation of male participants has been reported in other studies.19, 20 A possible reason could be that males appear to be more affected than females at a ratio of 2:1 in children. 1 It is also possible that the girl child receives less medical attention. 46 The age and average years of education were comparable to healthy children. Children with NS in the study were similar in age to those found in other studies.21, 27, 47 Most children with NS were from families belonging to lower-middle socioeconomic status compared to healthy children. Families’ socioeconomic status with NS was similar to another study. 48 Half the children with NS were from urban settings and most belonged to nuclear families. This information helps in understanding social factors and circumstances that impact health care.
In our study, children with NS had an early-onset and long duration of illness. The subtype was predominantly SDNS. Almost all of them routinely received corticosteroids, resulting in side effects such as growth retardation, hypertension, obesity, cushingoid features, and cataract. Children also had to follow up regularly with medical professionals, some requiring multiple admissions due to infections and relapses. They had to undergo multiple treatment procedures such as blood tests, assessing proteinuria, monitoring BP, measuring weight, and, in some cases, peritoneal dialysis. In addition, there are restrictions on dietary and everyday activities. All these have an impact on psychological well-being. These findings are similar to findings from other studies.17, 49
Studies have indicated an association between clinical-related variables and psychological problems in children with NS.17, 50 Similar to other studies,20, 51 our study found that children in the SRNS group had a higher risk of emotional and behavioral problems and poor physical health. Regarding temperament, rhythmicity was one variable negatively associated with the frequency of relapse and hospital stay. It may be that children with NS already had a predictable and adaptable pattern of physical functions, thus responding well to treatment and taking a shorter time to recover. We also found that family organization was negatively associated with the age of onset. The earlier onset of the illness often leads to early identification and intervention of the disease and helps families learn to manage it better. We also found that the total dose of steroids was positively associated with the family organization, indicating that medication could perhaps lead to better health, thereby adding more structure to families. The disease on the psychological outcome might be different if more samples were studied.
In the present study, both children with NS and healthy children exhibited the risk of emotional and behavioral problems. A systematic review and meta-analysis study conducted in India reported the prevalence of psychiatric disorders in children and adolescents in the community to be 6.46% and 23.33% in school. 52 However, children with NS indicated higher emotional and behavioral problems. On the SDQ, nearly half the sample of children with NS exhibited higher emotional and conduct disorders and less prosocial behavior. Ghobrial et al. 20 reported that those children with SRNS had lower prosocial scores but higher scores on emotional problems, peer problems, and overall total scores. The prevalence of significant conduct problems in cases was reported in another study. 48 Other studies have also noted higher behavioral problems in children with NS than in controls.18, 19, 27, 53
The QOL of children in the clinical group was also poor compared to healthy children. In our study, children in the clinical group scored lower on the physical and psychosocial (which comprises the emotional, social, and school) domains. Ruth et al. 23 reported impairment in the social functioning subscale of children with SSNS compared to normal children. However, a study conducted at a teaching hospital in South India found that children with NS had significantly higher QOL in physical, emotional, and social functioning domains than children with other chronic illnesses due to proper medication and regular follow-up. 49 Similarly, Eid et al. 51 found that the idiopathic NS group had significantly higher QOL scores than the chronic nonrenal illness group but significantly lower than the healthy control group.
Studies of temperament in chronically ill children have clinical significance since temperament may influence how the child perceives a situation and adjust to the illness.54, 55 Parents view chronically ill children as temperamentally more difficult than healthy children. 29 Physically sick children who were low on distractibility were likely more predisposed to developing psychological problems and may take longer to recover from distress. 56 However, our study did not find any difference in temperament between children with NS and healthy children. It is plausible that children in the study have a more adaptable temperament, hence lower psychological issues when facing illness and medical-related stressors. This is one future area studies must consider and develop knowledge on temperament in childhood kidney disease as no literature is available.
Our assessment of the family environment provided a general understanding of the family of children with NS. Our findings indicated significant differences in organization and control dimensions, suggesting that families of children with NS are less structured and less flexible. Although not significant, we also found that the scores of children with NS in family dimensions such as cohesion, expressiveness, conflict, independence, and achievement orientation were slightly poor compared to healthy families. Thus, it is possible that the illness can likely be a source of stress, leading to a slight change in the family structure.57–61 On the contrary, some studies have indicated that a positive family environment helps children and families adjust better during illness.15, 62, 63
We consider our study preliminary; hence, the study has several limitations. The small sample size limits the generalizability of the findings. The age range of children could have been more comprehensive. Analyzing various domains and subscales on measures could have given a better picture. The effects of education and parents’ socioeconomic status could have impacted the reported outcomes and limited the interpretation of the results to some extent. In the study, the questionnaire was addressed by either of the parents. Hence, the response might vary, and it would be interesting to compare the maternal and paternal responses separately. Finally, multicenter and longitudinal studies can only answer specific essential questions.
Despite these limitations, the study helps understand the psychosocial consequences of NS and provides some valuable directions for future research. Hence, the recommendation would be that all children are screened for psychological and social issues, and intervention is instituted as early as possible to avoid dysfunction and disability.
Conclusion
Children with NS have emotional and behavioural difficulties and, overall, poor quality of life. The illness also impacts the family’s setting up rules and structure, which are essential for planning responsibilities and activities. From a clinical perspective, findings emphasize the need for psychological support for these children regardless of disease severity or treatment modality.
Footnotes
Author Contributions
Each author has made substantial contributions to the manuscript.
AA: Conceptualization, methodology, data collection, writing—original draft, formal analysis.
VR: Conceptualization, methodology, writing—review and editing, supervision.
PP: Conceptualization, methodology, writing—review and editing, supervision.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was undertaken after approval from the institutional ethics committee (IEC Study Ref No. 207/2017) at St. Johns Medical College (SJMC).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was a part of the doctoral research of the first author, supported by the University Grants Commission-Junior Research Fellowship under Grant 333/ (NET-JAN 2017).
Informed Consent
Written informed consent from the parents and oral assent from the children were taken before initiating the study.