
Abstract
Background:
Anxiety is one of the most common mental disorders among school-going children and adolescents worldwide. Multiple factors like internalization of the symptoms, lack of proper objective assessment, societal stigmatization, and influence of parental pressure may alter the prevalence and incidence.
Aim:
The current study is done to identify the prevalence of anxiety disorders in school children and their associated risk factors.
Method:
A total of 550 students (266 boys and 284 girls), studying in grades 8 to 12 in urban and rural schools chosen by stratified random sampling, were subjected to a questionnaire survey by the team of trained investigators using “Screen for Child Anxiety and Emotion-related Disorder (SCARED)—child Version.”
Results:
Total prevalence of anxiety assessed using the SCARED scale was 51%. The prevalence of subtypes of anxiety disorders was also identified viz, generalized anxiety disorder—16%, panic disorder—23%, school phobia—17%, separation anxiety—31%, and social phobia—13%. All the disorders showed higher incidence in girls (P < .01).
Discussion:
The anxiety disorders were associated significantly with students from rural schools, those studying in the Tamil medium, those staying in hostels, students who had mothers who were employed, and living in extended family environments. Students who walked to school and who had neither of their parents as caregivers were more likely to have panic disorder, school phobia, social phobia, and separation anxiety disorder.
Conclusion:
This study documented a higher prevalence of anxiety disorders and subtypes and highlighted the factors associated with anxiety disorders in school students of the adolescent age group.
Introduction
Adolescent problems with internalizing behaviors are mostly associated with social withdrawal, dysphoria, and anxiety. 1 Anxiety, a natural human emotion, prompts a proactive and adaptive response to threatening or stressful situations. Anxiety can destabilize a person and push them into dysfunctional conditions in extreme situations. When anxiety arises in the absence of a challenge or stress, when it is out of proportion to the challenge or stress in terms of duration or severity, when it causes significant distress, and/or when it causes psychological, social, occupational, biological, and other impairments, it is considered pathological. 2 Anxiety disorders are one of the most common mental disorders among school-aged children and adolescents worldwide. 3 It is linked to a slew of detrimental consequences for children and adolescents’ social, emotional, and academic development. 4 Poor social and coping abilities, which often lead to avoidance of social interactions, loneliness, low self-esteem, fears of social rejection, and trouble developing friendships, are some of the specific impacts of anxiety.5–7 Avoidance of school reduced problem-solving abilities, and poor academic achievement has all been identified as negative outcomes.8–10
With the current school paradigm in India, where parents and society put pressure on kids to succeed, anxiety and accompanying psychological issues are unavoidable. 11 The incidence of these disorders is underreported due to multiple factors such as internalization of the symptoms, lack of proper objective assessment, societal stigmatization, and influence of parental pressure which prevents these children/adolescents to seek help. 12
In India, high educational expectations of parents and coercion for academic achievement are the most well-recorded causes of anxiety among school children and adolescents. 13 Individuals rely on the results of the secondary examination because it is the primary criterion for future admission to a high-quality senior secondary school and a selected academic stream. Hence, there is fierce competition among students since the number of places in these educational institutions is fewer than the number of students who apply. According to the National Crime Records Bureau (NCRB) report, in India, failure in examinations was accounted for about 1.4% of the suicides. 14
Even though children account for over 41% of India’s population (census 2011 projected statement), 15 child mental health care has gotten little attention in terms of service, research, and training. In developed countries, health professionals have major concerns about child and adolescent psychopathology. 16 Mental health disorders impact 10% to 20% of children and adolescents each year, and psychiatric morbidity accounts for 5 of the 10 primary causes of disability in children and adolescents aged 5 and up.17, 18 In developing nations, however, mental and psychiatric care for children lag behind those for adults.16–21 According to a few surveys undertaken in India, 7% to 30% of children under the age of 12 require either diagnostic or ongoing mental care.22–24
Anxiety in children and adolescents is influenced by a variety of sociocultural and family-related factors. The middle and lower socioeconomic status are found to be reported with a higher prevalence of anxiety disorders.25–28 Family-related factors like primary caregiver, siblings, type of family, parents’ education and employment, and school-related factors like type and location of schools, mode of commute to school, medium of instruction are associated with the development of anxiety disorders.26, 27, 29, 30 Maternal occupation has not been reported as a factor in the development of anxiety states among children 13 and children of employed mothers are more independent and confident than children whose mothers are unemployed.31, 32 Though previous studies have stated the possible factors related to anxiety disorders, very few studies have related them to the subtypes and considered family and school-related factors holistically.
The purpose of this study is to determine the prevalence of anxiety disorders in school students aged 13 to 17 years of both genders, as well as the pattern of these disorders concerning various school- and family-related factors.
Material and Methods
This cross-sectional questionnaire survey was initiated after obtaining clearance from the Institutional Ethics Committee and Review Board. Consent from the parents and assent from the students were obtained after getting permission from the school principals. A total of 550 students of both gender in the adolescent age group (13-17 years) were included in the study. Sample size calculated by the statistician considering prevalence of 30% (previous studies showed prevalence ranging from 10% to 49%), with a confidence limit of 5% and design effect of 1.5 (for stratified sampling method) was 484. Since we included all the students in the sections, the final sample size was 550. The schools were chosen after stratification by stratified random sampling method, in a way that two schools in urban setup and two schools in the rural setup were included and all the students from grades VIII, IX, X, XI, and XII were included. Based on the history, students who were previously diagnosed with a psychological disorder and those who were on treatment for the psychological disorder and/or other common psychosomatic illnesses were excluded from the study.
The Screen for Child Anxiety and Emotion-related Disorder shortly abbreviated as SCARED—child version was utilized in this study and it is known to have good reliability, convergent, and discriminant validity. 25 The scale consists of 41 questions that explain a situation and the student is expected to answer the frequency of it in the last 3 months using a Likert-type scale. Each item has a score and individual scores are added to note the presence of anxiety. Scores for specific questions are added to find the presence of generalized anxiety disorder, panic disorder, social anxiety disorder, separation anxiety disorder, and school phobia or significant school avoidance as per DSM-IV-TR criteria. In addition, this scale provides a cut-off to identify adolescents who are at risk of developing symptoms. A total cut-off of score ≥25 is considered to be screen positive, which indicates the presence of one or more anxiety disorders. Further, the scores also give a distinction between moderate anxiety (25-29) and severe anxiety (30 and above). The questions regarding different disorders are not arranged in a particular order but are distributed randomly to avoid bias in answering. For getting a response from Tamil medium students, the SCARED scale was translated into Tamil by a Tamil professor and then back to English by 2 bilingual researchers to ensure that the meaning of each word was fixed. The translated instrument was pilot tested among a sample of the study population who were not included in the statistical analysis and the validity of the same has been verified.
Following an introductory session about the study, the students were asked to fill the general proforma with questions regarding sociodemographic details and details on parents’ education and occupation, type of school, medium of instruction, siblings, primary caregiver, mode of commutation, and history of illness. They were then asked to answer each item in the SCARED questionnaire. Whenever the students had doubts, they were clarified by the trained team of investigators on a one-to-one basis. SPSS version 17 was used to analyze the data. The categorical data were analyzed using the chi-square test. Statistical significance was defined as a probability value of less than 0.05.
Observations and Results
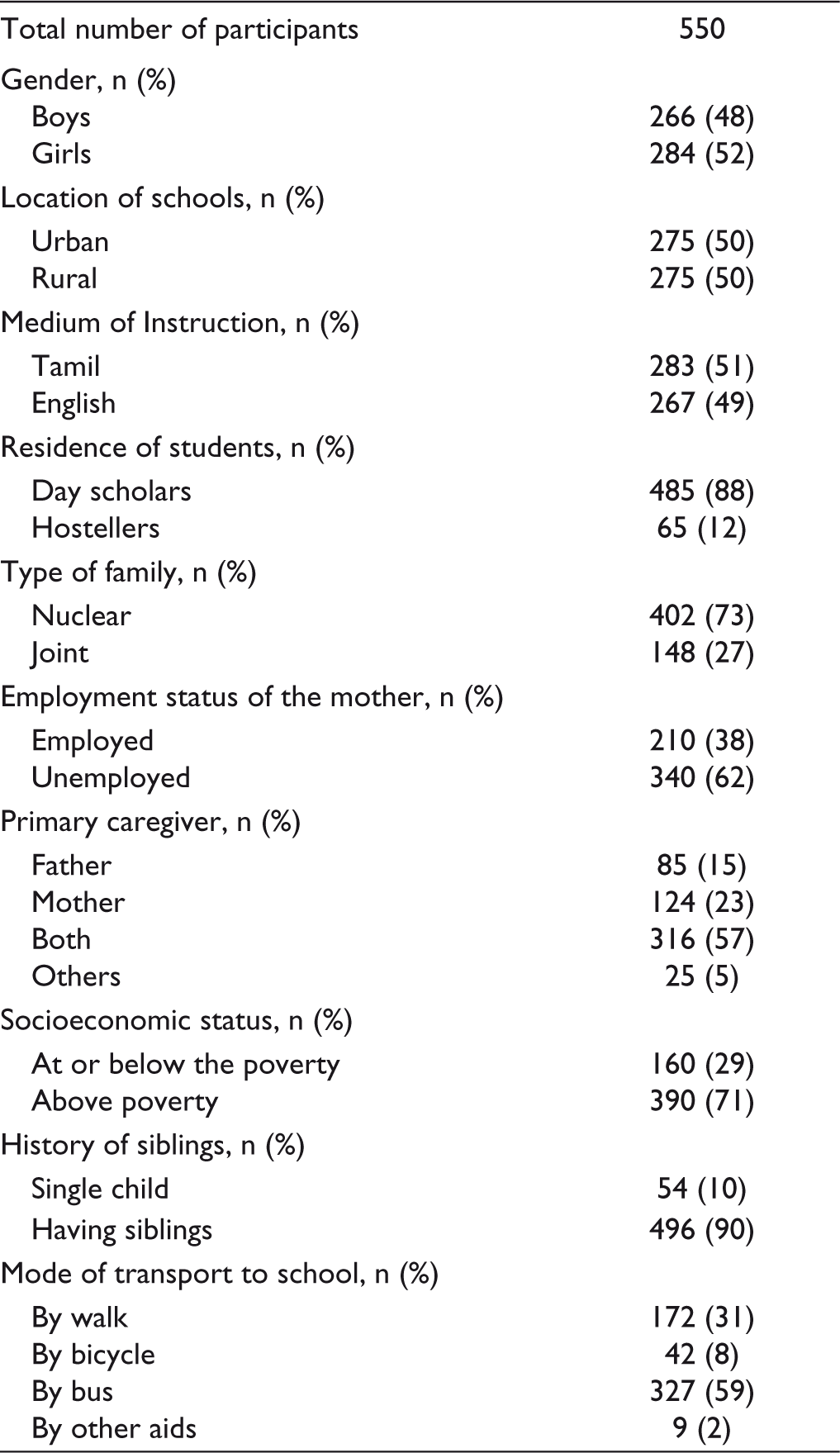
In total, 550 students (266 boys and 284 girls) participated in the study. Table 1 shows the sociodemographic characteristics of the participants.
Sociodemographic Characteristics of the Study Participants
The scores of the SCARED scale were calculated using the scoring system and analyzed using percentage analysis for estimating the prevalence of anxiety disorder and its subtypes. The same is depicted in Figure 1. The pie chart of Figure 1 explains the prevalence of various subtypes of anxiety disorders which were classified according to the scores stated in the SCARED scale. Separation anxiety is the most common followed by panic disorder. The bar diagram shows the classification of anxiety disorders based on the severity. The percentage of students having moderate and severe anxiety is 16.7 and 34, respectively.
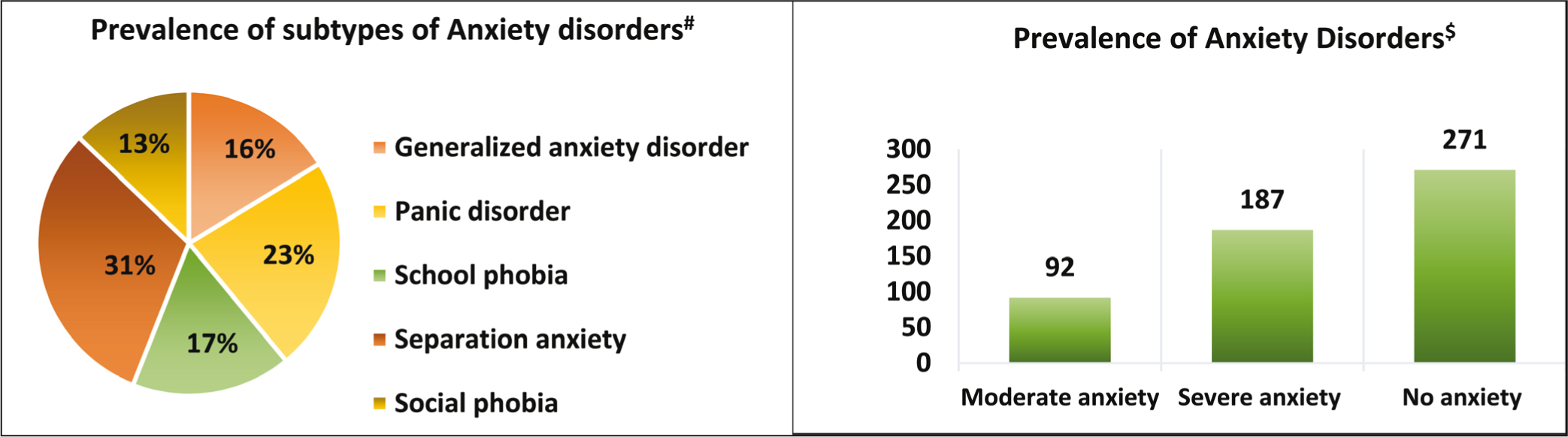
Table 2 explains the factors that have been known to be associated with anxiety. These include gender, location of schools, medium of instruction, the residence of students, type of family, employment status of the mother, primary caregiver of the student, and mode of transport of the students to school. These factors were analyzed for various subtypes of anxiety disorders by chi-square analysis. The prevalence of severe anxiety and its subtypes like generalized anxiety, panic disorder, school phobia, and social phobia were found to be significantly higher in girls than in boys. Students in rural schools had significantly higher anxiety scores for severe anxiety, panic disorder, and school phobia. Significance for all the above-mentioned factors was found at the level of P value less than 0.01.
Factors Influencing Anxiety Types in Students
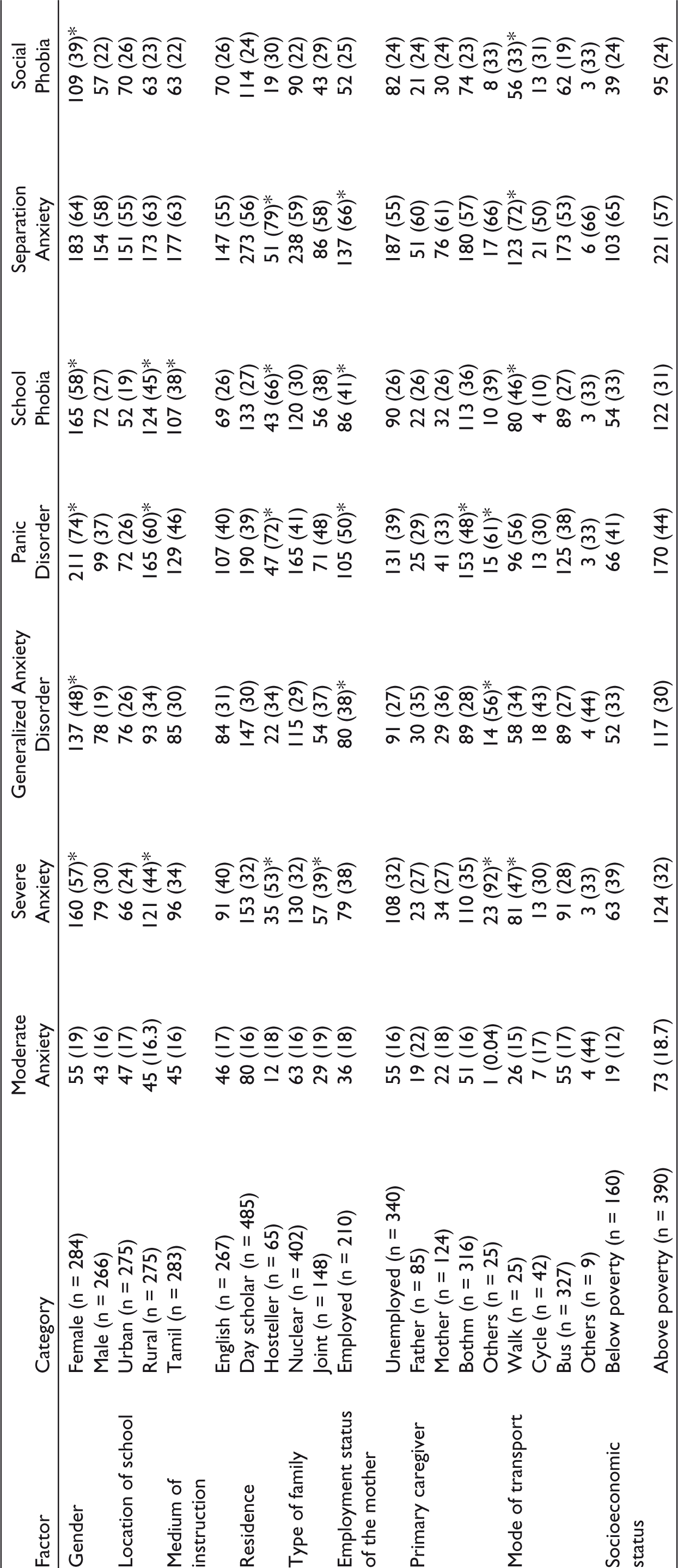
The values inside parentheses represent the percentage of students.
On comparing the influence of medium of education with the anxiety disorders, it was found that students studying in Tamil medium had significantly increased scores for school phobia than students in English medium. Students staying in hostels showed significantly higher scores for severe anxiety, panic disorder, school phobia, and separation anxiety when compared with the day scholars. Students who live in extended family environments had significantly severe anxiety. Students who have their mothers employed showed higher scores for generalized anxiety disorder, panic disorder, school phobia, and separation anxiety. When the primary caregiver was neither the mother nor the father, there was a significant prevalence of severe anxiety, generalized anxiety disorder, and panic disorder. A significant percentage of anxiety was present when the students attended school by foot, especially for panic disorder, school phobia, social phobia, and separation anxiety disorder.
Anxiety scores of students who were the only child in the family were compared with those who have siblings and it was found that there was no significant difference. The students’ socioeconomic level was shown to have no significant correlation.
Discussion
This study explored the prevalence of anxiety among the school students of the adolescent age group in South India, its subtypes, and its association with a variety of possible risk factors.
Prevalence of Anxiety and Related Disorders
The total prevalence of anxiety disorders in this study is 51%, of which 16.7% is moderate anxiety and 34% is severe anxiety. This is a higher value when compared to other previous studies done in various regions of India across a wide range of timelines in which the prevalence of anxiety ranged from 10% to 25%.26, 28, 33–35 One study by Al-Gelban 29 is in line with the present study showing a prevalence of 48.9% of anxiety among male students. On comparing these studies with the current study, the prevalence of subtypes of anxiety disorders was also found to be higher.
The higher prevalence in the current study may be attributed to the presence of highly ambitious students with a highly competitive nature since the students were approaching board exams. The survey instrument used in the referred studies were the Revised Child Manifest Anxiety Scale, 34 SPENCE Children Anxiety Scale, 35 self-reported questionnaire, 33 and SCARED Scale. 28 Also, the criteria for the classification of anxiety disorders varied from International Classification of Diseases-10 26 to International Classification of Mental and Behavioral Disorders 35 while the current study has used DSM-IV-TR criteria. Because of the different sample sizes, different survey instruments, and different diagnostic criteria used in the previous studies, a wide range of prevalence was observed.
Gender Differences
This study showed that females are more affected than males with a female to male ratio of 1.8. This observation is supported by other studies.3, 33, 36–38 Few studies argue that males are more affected with anxiety and depressive states than females.13, 35, 36 The higher prevalence of anxiety disorders in females in the current study may be due to conflict between older cultural practices in India, the growing public awareness on female education, and widespread domestic changes brought about by globalization.
Urban-Rural Differences in Anxiety Scores
Some of the previous studies on childhood anxiety disorders have stated that the children in urban school setups have greater anxiety disorders than children from rural setups26, 39, 40 and another study has found no significant difference between students from urban and rural schools. 34 However, we found that a greater prevalence of anxiety disorders was found among students from rural schools. The scores for severe anxiety disorder, panic disorder, and school phobia were significantly higher in students from rural schools when compared with those from urban schools. This may be because of the lack of awareness on mental health, lack of medical facilities for early assessment, and treatment in the rural setup.
Effect of the Medium of Education on Anxiety Scores
The current study showed significantly increased scores for school phobia in children studying in Tamil medium when compared to children studying in English medium. This observation is supported by another study which showed a similar increase in anxiety scores for children studying in Bengali medium compared to English medium. 13 This difference, particularly in the prevalence of school phobia, maybe because of the apprehension regarding the fact that the world of information is controlled by English, and prospective work chances in English-speaking countries are many. Also, the students from Tamil medium may be having apprehension regarding the upgradation of learning resources in Tamil compared to the resources in English.
Effect of Residence of the Students and Mode of Commutation to School on Anxiety
The present study highlights that those students staying in hostels showed significantly higher scores for severe anxiety, panic disorder, school phobia, and separation anxiety when compared to day scholars. This may be due to the different environment, lack of physical and mental support from parents, and trepidation toward the school authorities. Many studies have documented an increase in anxiety disorders in boarding schools.29, 40
The day scholars who attended school on foot, had significant panic disorder, school phobia, social phobia, and separation anxiety disorder. This may be explained by the fact that the time consumed for walking may affect the school entry time and also the students may be encountering judgmental societal pressure which may lead to anxiety.
Type of Family, Siblings, Primary Caregiver, and Employment Status of the Mother
In general, this study observed an increase in the prevalence of anxiety in students hailing in extended families. This finding was supported by a study by Banga 30 and contradicted by Mandaknalli and Malusare. 33
In addition, the absence of a parent as the primary caregiver was significantly associated with the prevalence of severe anxiety, generalized anxiety disorder, and panic disorder.
We also noted the prevalence of different types of anxiety disorders was higher in children of employed mothers. The mother’s absence and lack of opportunity for discussion on emotional issues could be contributing to the escalated feelings of anxiety among students of employed mothers. This may be because, in extended families, the attention from the parents, especially the mothers, toward their children was diluted by other factors. Also, the attention may not be given to children in particular because of the increased responsibilities and shared resources. As previously described by Anitha et al, increased scores for all anxiety disorders were observed in children with one or more siblings even though this is statistically significant. 41 This may be because of sharing of love, affection, care, and resources from the parents.
Effect of Socioeconomic Status on Anxiety Disorders in Children
The majority of studies have postulated that anxiety is more common in low- and middle-income groups of people when compared to high-income groups.26, 33, 42, 43 The current study could not find any statistically significant difference in socioeconomic status, though, in few subtypes of anxiety disorders like school phobia, generalized anxiety disorder, and separation anxiety were found to be higher in students from lower socioeconomic statuses. Also, the number of students in low and high socioeconomic groups was not comparable.
Conclusion
We found a higher prevalence of anxiety disorders and subtypes in school students of the adolescent age group when compared to many previous studies. This study has highlighted that female gender, rural schools, native language (Tamil) as the medium of education, extended family environment, hostel accommodation, employed mothers, primary caregivers being other than parents, and walking to school as being significantly associated with increased anxiety scores in school students.
Limitations
The role of teachers, religious beliefs, and cultural practices has not been evaluated in this study. These factors may be considered as a lead for future studies in the evaluation of anxiety among adolescents.
Footnotes
Author Contributions
All the authors were involved in the conception of the work, acquisition, analysis, and interpretation of data, drafting of the report, and manuscript. All the authors uniformly approved the final version prepared for publication.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This is a study done for the Indian Council of Medical Research (ICMR)—Short-term Studentship (STS) Program by Dr Pavithra T, Dr Anbarasi M, and Dr Rajkumar G, when Dr T Pavithra was a prefinal year MBBS student at Chennai Medical College Hospital and Research Centre, Trichy (now named as Trichy SRM Medical College Hospital and Research Centre).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.