
Abstract
Somatic Symptoms or Medically Unexplained Symptoms are commonly found in children and adolescents. These symptoms generally reflect the underlying psychological distress and cause significant distress to the child. Presenting symptoms include abdominal pain, headaches, and musculoskeletal pain. The nature of illness prompts multiple visits to clinical setups, burdening the existing health resources. Risk factors include individual, family, and environmental factors. Most stressful factors are seen to arise from day-to-day problems in children like academic problems, bullying, familial disharmony, temperamental traits, abuse, financial constraints, and parenting issues. Psychiatric and physical comorbidities are prevalent. During the assessment, it is pertinent to rule in positive signs and keep in mind the common psychiatric/physical differentials. Management includes a multidisciplinary approach involving the child and family. An overall visualization of the biopsychosocial framework of the child is done to cater to specific needs. Psychoeducation remains a key strategy, while incorporating behavioral management. This includes promoting strengths and positive behavior in child, gradual reduction in secondary gains, promotion of general well-being, focus on a well-rounded schedule incorporating different activities, and relaxation training. Psychosocial factors are worked upon at length while enhancing coping skills. Familial factors are taken into consideration and home environment may be improved. Comorbidities if present can be managed with medications. The goal is functional recovery and rehabilitation, which can be time taking and requires patience from the treating team.
Introduction
“Medically Unexplained Symptoms” (MUS) or “persistent bodily complaints for which adequate examination does not reveal sufficiently explanatory structural or other specified pathology” describes individuals presenting with pain and discomfort in general practice and secondary care.1, 2 MUS or somatic (physical) symptoms can be manifestation of underlying emotional and psychological distress. The term “Somatization” can be used to describe an amalgamation of clinical and behavioral features denoting that the person is experiencing psychological distress through physical (somatic) symptoms. These may not be explained by pathological findings, although the person may attribute this to a physical illness and seeks medical help. In somatization, the production of symptoms is usually not under conscious control; however, in children and adolescents it is particularly difficult to establish the level of conscious control. 3 Unexplained physical symptoms lead to difficulty and distress, impairment in daily functioning and repeated healthcare- seeking behaviours. 3 Symptoms can occur at different grades of severity and distress. When multiple symptoms coexist concurrently, underlying psychological problems should be suspected. Somatic symptom disorder, conversion disorder, dissociative disorder, chronic fatigue syndrome, and fibromyalgia are all disorders comprising of prominent somatic symptoms.
These symptoms can be found in all age groups. They are more prominent in females. They have a prevalence of 2% to 10% in children. 3 The commonly observed symptoms include pain in early childhood. In adolescent age group, conversion symptoms are more likely. 3 Presenting symptoms in childhood are recurrent headaches, musculoskeletal, and abdominal pain. Abdominal symptoms increase in frequency from 3 to 9 years of age and then steadily increase up to adolescence. Headaches are less common in pre-schoolers than in older children or in adolescents. In females, pain disorder has an age at onset of 11 to 19 years, whereas males have an age at onset under 13 years.2, 3
Preschool children presenting with frequent somatic symptoms are more likely to have emotional and behavioral problems. They are also at increased risk of psychological problems later on especially when placed in stressful situations.4, 5 They often have difficulties in regulating their emotions, coping with stress, and managing their problems in day-to-day life.
The nature of these symptoms is impairing, persistent, and mostly physical in nature. Due to repeated physical symptoms the primary point of contact for treatment remain physicians, pediatricians, and neurologists. The nature of illness and help seeking behaviors prompt multiple investigations and treatments before they reach a psychiatric set up. Often, resistance is observed from patients regarding a psychological basis of the symptoms. This leads to over burdening of health resources, wastage of monetary resources of the family, and delay in adequate management of the patient. 5
Etiology
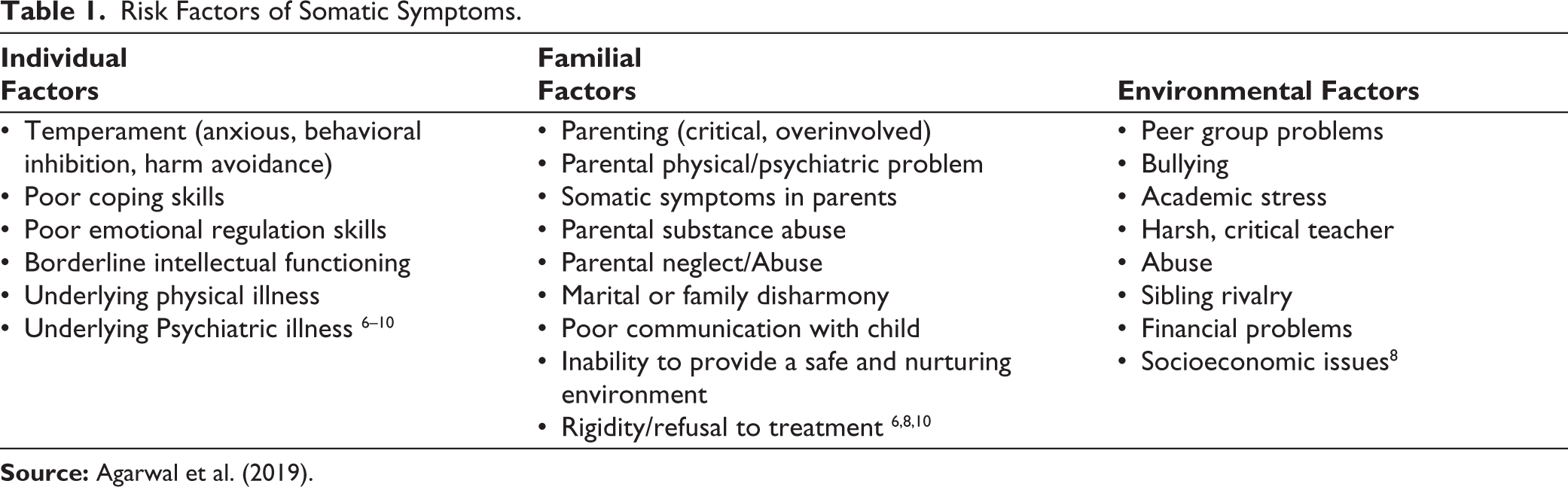
Somatic symptoms can present with underlying physical or psychiatric illness. Visualization of multiple impacting factors helps in formulating the case. These can range from individual, familial, environmental, to sociocultural factors (Table 1). They may be predisposing, precipitating, and perpetuating factors. 3
Risk Factors of Somatic Symptoms.
Comorbidities
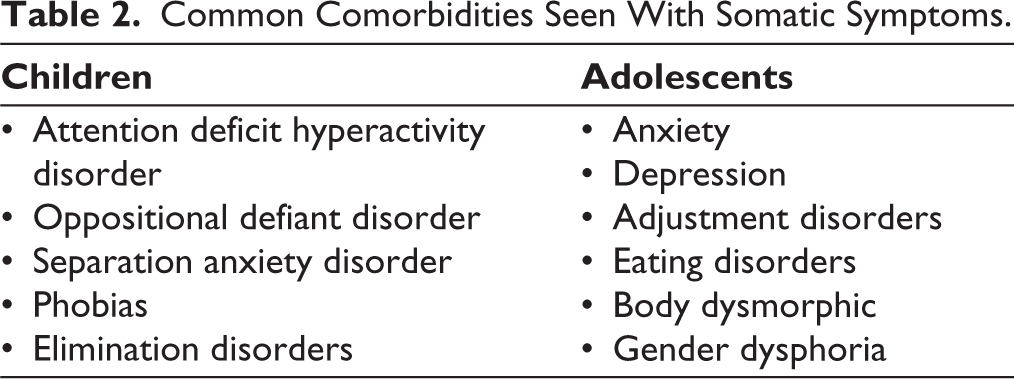
Somatic symptoms often occur with comorbidities especially in children with chronic symptoms (Table 2). These could be physical or psychiatric comorbid illness. It is crucial to differentiate what symptoms are congruent with the said physical illness as it forms an important aspect in treating the child. About one-third to half patients are seen to present with psychiatric comorbidities.3, 11, 12 The number of comorbidities also increase, as the severity of the symptoms increase. Delineating the primary psychopathology becomes pertinent. Addressing and adequately treating them becomes a crucial aspect during the management.
Common Comorbidities Seen With Somatic Symptoms.
Differential Diagnosis
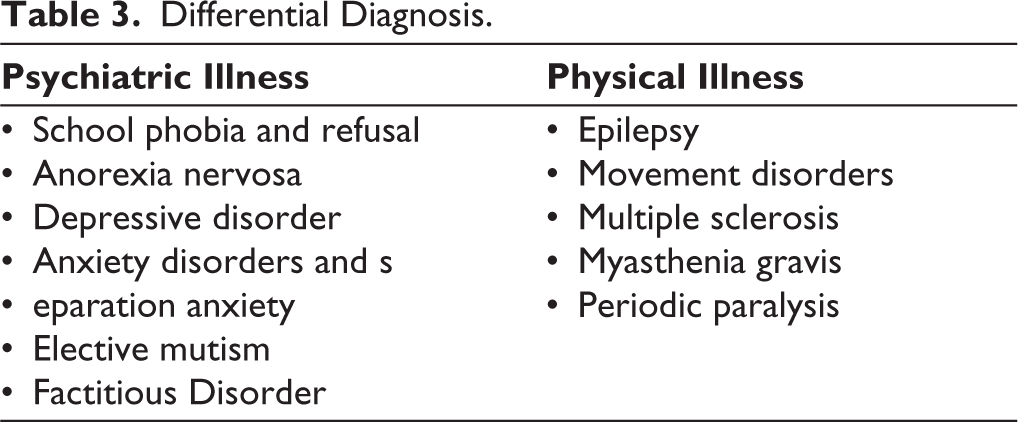
Similarly, as somatic symptoms can mimic a plethora of physical and psychiatric illness, it is necessary to differentiate the primary etiology and proceed accordingly.3, 8, 11, 12 Somatic symptoms could be the manifestation of underlying physical of psychiatric illness (Table 3).
Differential Diagnosis.
Assessment
For a thorough assessment of somatic symptoms, multiple informants and sittings can be considered. A joint assessment with pediatrician would be good though often not possible. A detailed history, and physical and mental status examination should be done. Things which should be kept in mind while doing evaluation include account of current symptomatology, temperament, intelligence, coping skills, strengths, parenting styles, family functioning, schooling, and peer relationships. History of abuse and self-harm should be taken. At the same time it is important to screen for many comorbid psychopathology and concurrent physical illness. When the child classifies for more than one psychiatric illness, the primary pathology should be established. The emphasis should not just be on ruling out organic factors but ruling in of positive symptoms to establish a diagnosis. Emphasis should be given to the various psychosocial factors present in the child’s life, which can be classified into a biopsycho- social framework. Screening family members especially for psychiatric illness or personality disorders becomes a part of the evaluation as well. The presence of a role model, if any should be highlighted. A visualization of all the factors in the child’s life helps in formulating the case holistically and forms the basis for effective management.12–15
Management
A multimodal approach is required for effective management in all spheres. A multidisciplinary team should be formulated for thorough evaluation of all the somatic complaints of the patient. They can comprise of clinicians, psychologists, social workers, physiotherapists, occupational therapists, and school teachers along with patient and family. The treatment usually consists of 2 parts—early treatment directed toward symptom removal and long-term treatment directed toward the resolution of stressors and prevention of further episodes. A comprehensive management plan can be devised catering to the specific problems faced by the child.14–18
The primary focus should be on psychoeducation. Communicating the diagnosis and moving from a medical model to psychological model of illness could be difficult for family to understand initially.16, 18 At the same time, acceptability and readiness to understand a psychological model of the illness to the family can be assessed. Addressal of family’s concerns should be done. If needed, extended family members can be engaged as well. Avoid any confrontation with the family regarding the acceptance of diagnosis. It should be acknowledged that the child has real symptoms and sufferings but the reasons could be psychological. Harmlessness of the symptoms should be emphasized repeatedly. It should be explained that the symptoms in the absence of serious physical disease are common. Mind body relationship can be explained in detail especially taking example of any recent episode or like when someone is anxious, he/she may have palpitations. Stressor, although small in magnitude, mostly arise from day-to-day issues but could have a deep impact on the child. Additionally, discouraging the use of offensive terms and promoting child friendly language should be kept in mind.14, 15 Building up rapport with the child is key to a good therapeutic relationship. The aim becomes to promote positive behaviors and focus on the strengths of the child (Table 4).
Behavioral Management.
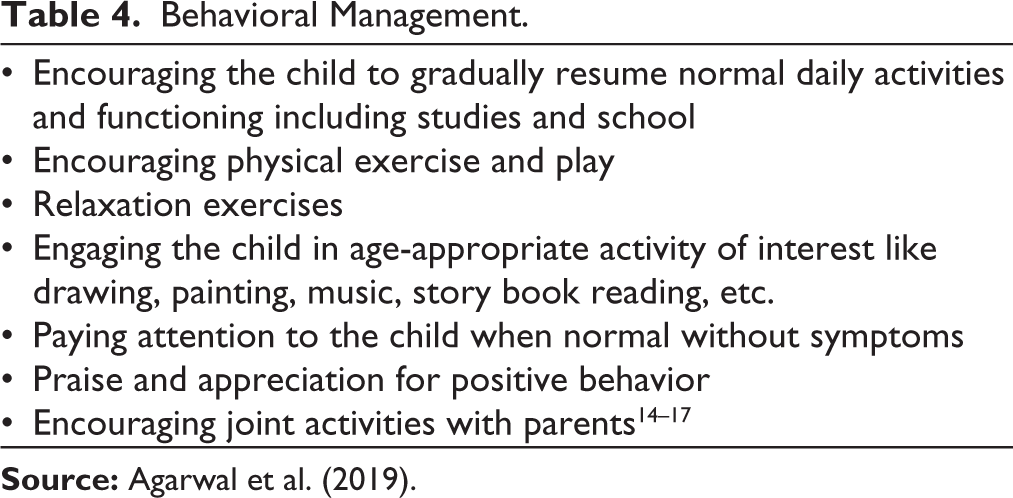
Reduction in secondary gains is not advisable very early in the treatment and without adequate explanations to the family. The reduction of gains should be a gradual process. The psychosocial factors leading to symptoms must be discussed in detail with patient and family. The focus should be on finding realistic solutions to the problems and work done on them. This could also involve the child’s coping skills and need changes to be done in the external environment. Liaising with school authorities in children with academic problems can be fruitful for the child in long-term. In those cases, where the factors for stress have been revealed privately, consent should be taken before disclosing to family. The strengths of the child can be emphasized during this process. Encouraging children to find confidantes—parents/siblings to share problems and find solutions in the future. Enhancing communication between children and parents are other avenues which should be explored.8, 16, 17, 19–21
Ruling out comorbidities and their adequate mana- gement, medication should only be used in cases with con- comitant behavior problems, anxiety and depressive disorders. Psychotherapy can be used in children with history of trauma, abuse, and self-harm. Family focused interventions can be used in dysfunctional family setups and chronic symptoms. For maladaptive temperamental traits and coping skills, effective psychotherapeutic techniques can be taught. Cognitive Behavioural Therapy can also be planned. Recent studies have suggested the use of physiotherapy and occupational therapy for children presenting with specific motor symptoms. An overall promotion of rehabilitation and functional recovery of the child should be our goal.19–21
Hospitalization is advised if there is any doubt in the diagnosis, symptoms are severe, family is very distressed, symptoms are chronic and resistant. 14
Case Vignette
Miss B was a 15-year-old girl, third birth order, semi urban, middle socioeconomic status and joint family with her grandfather and uncles. The main decision maker of the family was her grandfather. The child was promoted to Class 10th 8 months ago. She presented with complaints of episodes of abnormal body movements followed by unresponsiveness for 3 years, which exacerbated for the last 6 months. Additionally, she complained of weakness, headache, reduced appetite, and occasional abdominal pain. Intermittently she also has difficulty sleeping. For last 3 years, she has taken consultations from various doctors, emergency services, and multiple anti epileptics, anti-psychotics, and anti-depressants. Once, the family was explained that she might be suffering from a psychiatric illness. Her grandfather refuted this and decided they would take her to a higher center, even if it meant spending much more money than they can afford. Faith healing was done simultaneously. Multiple blood and radiological investigations were done which were within normal limits. She was referred from neurology to psychiatry. There was no psychiatric or physical comorbidity. She has not been attending school for the last 4 months. There were frequent disagreements between her mother and her aunts. Everyone was afraid of her grandfather; all his commands and decisions were obeyed in the house without any rebuttal. He often criticized the family members especially the children over trivial issues in front of the entire family. Her father was strict and often pressurized her to do well in academics. At times, her father beat her when the child scored less marks. He constantly compared her with her siblings and belittled her in front of others. She was not able to communicate with her father as she felt he would scold her. She was extremely pampered by her siblings, mother, and grandmother as she was the youngest in the family. They fulfilled all her wishes and demands. Her mathematics teacher was extremely strict and often made fun of students in class. He did not entertain doubts and at times gave harsh punishments to students. He had been her teacher for the last 3 years and had started to pick on her in class for 6 months as she was poor in mathematics. Temperament denoted temper tantrums, low frustration tolerance, and the patient becomes anxious easily. She was sensitive to criticism, had frequent demanding behavior. The child has an interest in dancing and likes to paint in her free time. She was very good in craft (which were discouraged by her father). On general physical and systemic examination, no abnormalities were present. She had low self-esteem, was apprehensive regarding the future. She acknowledged being stressed but could not attribute it to her symptoms. She felt she was unable to regulate her emotions. Her intelligence seemed average on clinical evaluation. Stressor was revealed to be scholastic issues in the form of difficulty in understanding English, Science, and Mathematics since she joined class 10th but felt scared to ask for help. Role model was present—history of similar complaints in a girl in her class. She improved with treatment and during the course of treatment she made this beautiful craft (Figure 1). She could indulge in craft for hours together without any symptoms. She learned this without any training at home watching YouTube videos.
Craft Made by Miss B.

Conclusion
Somatic symptoms are commonly found in children and adolescents. About 10% to 15% children go in chronic illness. A thorough assessment requires envisioning a biopsychosocial approach and working on specific issues. Assessment should include the temperament, intelligence, coping skills, and psychosocial factors faced by the child. A multidisciplinary approach has proven to be most effective in management of these cases. The treatment process often may become long and tedious and requires patience. The mainstay of management is psychoeducation, focusing on positive behaviors, strengths, and behavioural management. The involvement of family members and working as a unit is key. Tremendous amount of psychological work has to be done with patient and family for positive results. Addressal of family’s concerns and treating any psychiatric illness in family is important as well. Harmlessness of the symptoms should be reiterated and psychoeducation is crucial at every step. Screening and managing comorbid conditions with medication, if need be, is necessary.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent from the parent and assent from the child was taken for publication of case vignette.