
Abstract
Background:
Child sexual abuse (CSA) is a trauma that creates havoc in the personal and social lives of CSA survivors. The survivors in Kerala, India, struggle amidst the cultural background that silences CSA. Rehabilitation efforts in the state are channelized through government-run shelter homes that serve as the second home for CSA survivors.
Method:
We used a correlational research design with purposive sampling. From shelter homes in Kerala, 267 female participants (age range: 10-18 years, mean age: 16 years) were recruited. A personal data sheet and an emotional health questionnaire (EHQ) were used to collect data. Spearman rank correlation coefficient, linear regression, Kruskal–Wallis H test, Mann–Whitney U test, and Dunn’s post hoc test were used to analyze data.
Results:
Positive relationships among the emotional health variables namely aggression, anxiety, and depression were found, whereas a negative relationship existed between these variables and resilience. Further analyses found that the emotional health variables significantly predicted the resilience among survivors of CSA. In addition, there exists significant differences in resilience based on sociodemographic variables, such as age, duration of stay, and friendships, but resilience did not vary based on the religion and birthplace of survivors.
Conclusion:
Results suggest that participants experience moderate levels of emotional distress. Provision for integrated psychological support is recommended in the present rehabilitation process in Kerala. The mentoring relationships developed in the institutions are found to be instrumental in building confidence and hope in the participants, which is reflected in the trends in their resilience scores.
Keywords
Introduction
Childhood is a period of growth and development across multiple domains–physical, psychological, and social–that are interrelated. 1 The optimal climate for this developmental phase involves safe, stimulating environments at home and school that facilitate positive interaction patterns with the social world. 1 Inadequate and harmful environments that perpetuate neglect and abuse result in long-standing vulnerabilities and maladjustments throughout the life of the child. Unfortunately, it is estimated that globally, 1 out of every 2 children (2-17 years) experience some form of violence–interpersonal, self-directed, or collective–each year.2, 3 UNICEF data indicate that globally 15 million adolescent girls of age 15 to 19 years have been forced into sexual contact and data from 30 countries show that only 1% of them sought professional help. 4 This suggests the danger posed by sexual violence against children together labeled as child sexual abuse (CSA) and affirms the central place for CSA in research, policy-making, and sustainable development.
The World Health Organization (WHO) 5 defines CSA as “the involvement of a child in sexual activity that he or she does not fully comprehend, is unable to give informed consent to, or for which the child is not developmentally prepared, or else that violate the laws or social taboos of society.” The nature and elements of sexual abuse and abusive relationships are usually traumatic, it blocks normal psychosocial develop-ment and could culminate in psychosocial maladaptation. 6 Individuals with a history of CSA are found to develop psychopathological conditions like posttraumatic stress disorder, depressive symptoms, particularly, suicidal idea-tions, anxiety disorders and panic episodes, hyperarousal, substance use, and personality disorders, and have issues in social functioning that reflect in lack of trust, reduced social contact, less satisfying relationships, and issues with relationship adjustment. 7
Adverse consequences of CSA are mediated by survivors’ resilience, that is, their ability to bounce back from an adverse situation and cope with the trauma. Three interactive factors together contribute to the development of resilience–characteristics of the child, the family, and the social environment. 8
Several protective factors have been identified to promote resilience including internal factors such as optimism, external attribution of blame, education, spirituality, and socioeconomic status; family factors such as family social support, stability of the family, positive parenting, relationship quality, and presence of a confidant; and community factors like social support, community involvement, and school safety.9, 10 Among CSA survivors living in the foster care system, it was observed that optimism, positive peer influences, educational expectations, natural mentoring relationships, and a sense of belonging have a strong impact on their resilience.11, 12
The context of Asian countries, including India, is intricate because cultural values silence and even threaten the disclosure of CSA, which leads to underreporting and unreliable prevalence data.13, 14 The individual, family, community, and societal factors that serve as the determinants of CSA have been found to be interspersed with patriarchal societal norms and gender-based power differentials prevalent in India. 15 Madu, 16 in a study of 722 undergraduate students found that under one-third of the respondents reported experiences of sexual abuse. Alarmingly, 68.2% of female victims and 83% of male victims of CSA did not perceive their experience as CSA. This largely depended on the culture-specific perceptions and attitudes that operate in two main ways. Firstly, some cultures may see this type of behavior as normal and within the range of expected behaviors within that culture. Secondly, many families see CSA as taboo and associate it with threat and shame, which results in many cases of CSA not being reported to health care workers and the police. 16 The culture-specific perceptions and attitudes about CSA are also reflected in several internal issues faced by CSA survivors including self-blame, internalization of sexual experiences, feelings of regret, powerlessness, helplessness, and insecurity, and most importantly, not perceiving their experience as abuse at all.16–18
The scenario in Kerala, the southern state of India, is a clear replication of the Indian context. Prevalence studies based on primary and secondary data indicate that there is a disturbing hike in the sexual abuse of girl children in Kerala, a larger part being perpetrated by people familiar with the abused children.19–21 In 2013, the Government of Kerala set up shelter homes across the state that serve as rehabilitation centers for survivors of CSA and human trafficking. With the objectives of protection, prosecution, and prevention, the survivors in these homes are given health, education, and employment facilities to improve their status in society and reintegrate them by focusing on their life skills and creativity.
Presently, there are 13 shelter homes across Kerala that protect survivors of CSA who have been legally involved in Protection of Children from Sexual Offences (POCSO) cases. These homes serve as short-term shelters for CSA survivors, who have reported their abuse and are undergoing judicial trials. The legal processes may go on for a longer duration, and the survivors are not sent back to their homes unless the safety and security of their family and home environments are verified by Child Welfare Centers. In these homes, rehabilitation services are provided with the objective of social integration of these survivors. Such services are monitored using individual care plans developed after assessing the social, educational, economic, medical, and psychological status of each inmate. Later on, education, vocational training, life skills training, and psychological support are provided based on the individual child’s requirements. Depending on the rehabilitation services, delays in judicial trials, and safety concerns regarding the home environments, there is wide variability in terms of the duration of a survivor’s stay in these shelter homes. Some inmates are reported to be staying even after 18 years of age as their families are not found to be safe places for them.
Multiple factors like the cultural milieu of Kerala founded on patriarchal norms and gender-based power structures, the resultant trauma associated with the judicial and rehabilitation process, and the breadth of consequences of CSA, particularly the discrimination and exclusion, influence the well-being of CSA survivors. Hence there is a pressing need for investigating the factors that can promote positive adaptation and resilience among CSA survivors in Kerala. The complex and dysfunctional family environments of CSA survivors, that even perpetrate abuse, raise the need for evaluating the effectiveness of institutional care.
The objective of this study is to identify the emotional and sociodemographic factors that influence resilience among CSA survivors under institutional care in Kerala. Overcoming the methodological problems of sample selection bias and the absence of validated assessments of CSA, 15 this study targeted the inmates of Kerala’s government-run shelter homes for CSA survivors, who have been legally involved in POCSO cases.
Method
Participants
The study is part of a research consultation project, funded by the Department of Women and Child Development, Government of Kerala, aimed to explore the psychosocial profiles of institutionalized young girls and propose a model for enhancing support and societal integration. The study was approved by the Ethics Committee, Department of Psychology, University of Kerala. After completion of the project, the findings were presented before the representatives of the funding agency, and permission was granted for publication.
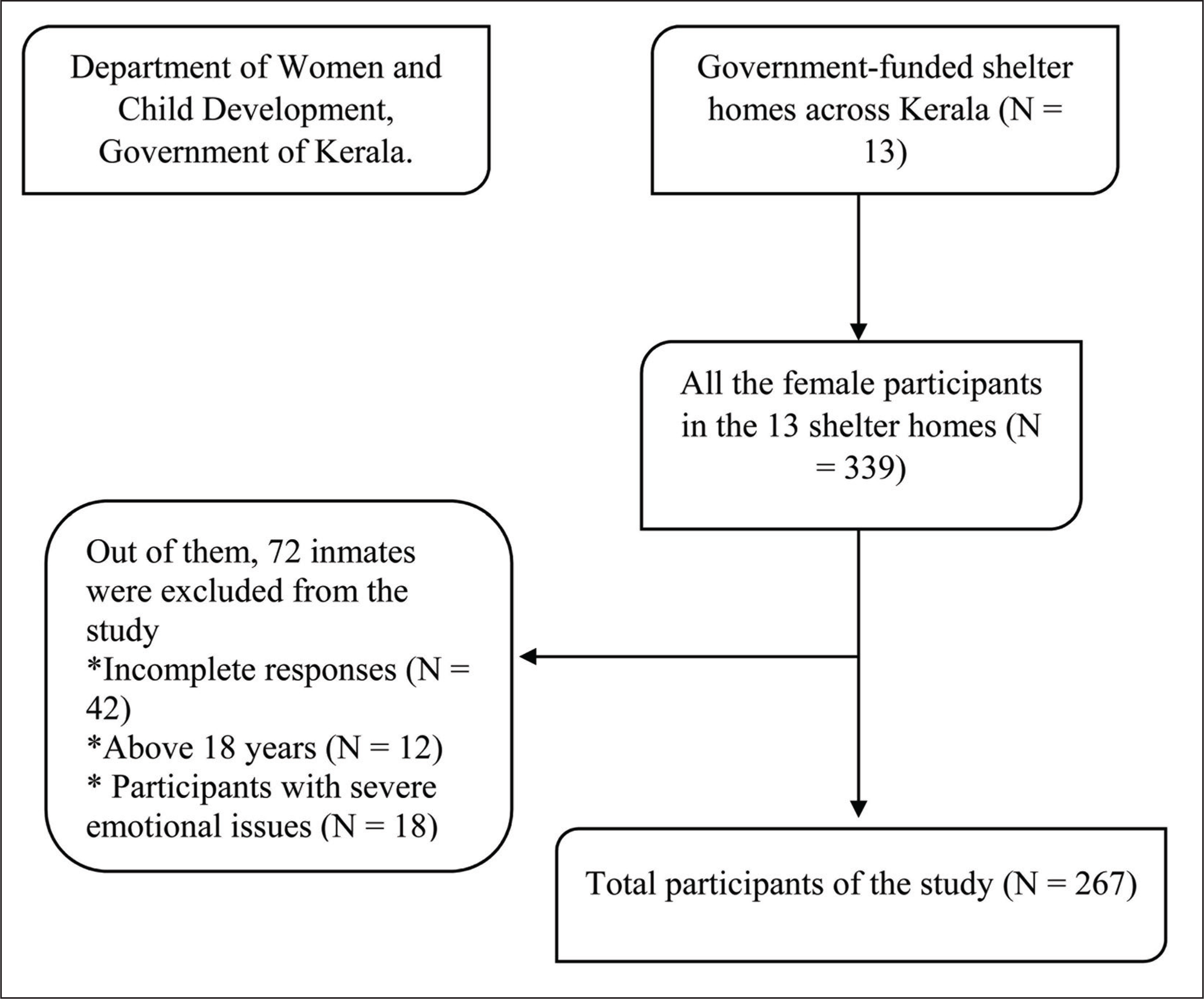
It is a correlational study using purposive sampling in which 339 female participants, who are inmates of the 13 government-funded shelter homes across Kerala, were selected. Out of them, inmates who were above 18 years of age (N = 12, 3.5%) and who gave incomplete responses (N = 42, 12.3%) were excluded. Some participants (N = 18, 5.3%) exhibited serious psychological disturbances during the assessment and their data are not included in this study, as they were not in a condition to cooperate with the assessment. Thus, the sample of this study included 267 participants, as seen in Figure 1.
Selection of Participants for the Study
Procedure
Participants were assessed during a summer camp organized for all the inmates of the shelter homes. Before the assessment, approval was sought from the institutional authorities and informed consent was obtained from the participants. Research assistants were given a two-day orientation and training program to familiarize themselves with the assessment tools. Because the study participants are on judicial trial and have experienced extreme trauma, research assistants also talked with the wardens and house administrators of shelter homes to better prepare them for data collection. On the days of the camp, the research assistants, under the supervision of research associates and the principal investigator of the project, interviewed the participants individually after establishing rapport with them.
No questions about their abuse history and trauma were asked. During the conduct of the assessment, the service of clinical, medical, legal, and community health professionals was sought, when needed, because the physical and psychological conditions, family backgrounds, and legal proceedings varied widely among the participants. Participants were assured of their anonymity and confidentiality of the information they gave. Their participation was completely voluntary and assessment sessions were discontinued if participants were unwilling to respond.
Instruments
A personal information sheet was used to collect the sociodemographic details of the participants including their age, birthplace, religion, duration of stay at the institution, and presence of friendships.
Emotional Health Questionnaire (EHQ)
The emotional health questionnaire was developed exclusi-vely for this study by Thomas et al 22 to measure anxiety, aggression, depression, and resilience among the participants. The EHQ has 4 dimensions, anxiety, aggression, depression, and resilience, and consists of 50 items on a 5-point rating scale. The reliability of the instrument was 0.898 for the anxiety items, 0.872 for the aggression items, 0.888 for the depression items, 0.822 for the resilience items, and 0.908 for the overall items.
Process of Tool Validation
The process of developing EHQ began with seeking knowledge, skill, and experience from experts who were dealing with CSA. The literature review focused on CSA contributed to the construction of the first-round questionnaire.
Face Validation
With expert guidance, face validation of the items was carried out.
Content Validation
All items derived from the literature were subjected to the process of content validation, to guarantee the content validity of the instruments. Content validation was done by 32 experts drawn from the field. The incorporation of expert opinions, recommendations, and a brief discussion with the home managers and caretakers of CSA survivors in shelter homes resulted in the preparation of the final tool. The tool was designed to assess emotional health with 50 items.
Statistical Analysis
The data collected from the participants were scored and organized for data analysis. The collected data were subjected to statistical analysis using Statistical Package for Social Sciences (SPSS) 25. Each variable in the study was examined separately using univariate analysis, normality, frequency distribution, mean, and standard deviation. As the data lacked a normal distribution, Spearman rank correlation coefficient, linear regression, Kruskal–Wallis H test, Mann–Whitney U test, and Dunn’s post hoc test were used to analyze correlation, predictive role, and comparisons among the emotional health and demographic variables.
Results
The sample of the study included 267 participants, who were inmates of the shelter homes across Kerala. Inmates staying in the home for a duration of 1 month to 96 months were part of the study and their ages ranged between 10 and 18 years.
The majority of the participants 62.9% (168) were between the age of 16 and 18 years. About 71.2% (190) of them belonged to the Hindu religion and most of them 61% (163) were from villages. About 43.8% (117) of the sample constituted participants who have been residing in the shelter homes for the duration of 3 months to 1 year. About 97.8% (261) of the participants had friendships and reported having good friends.
Among the participants, 37.8% (101) exhibited an average level of aggression and 36.3% (97) reported average scores on the anxiety scale. Among them, 37.8% (101) of the sample reported very low levels of depression. Also, 58.4% (156) of the participants reported having high resilience.
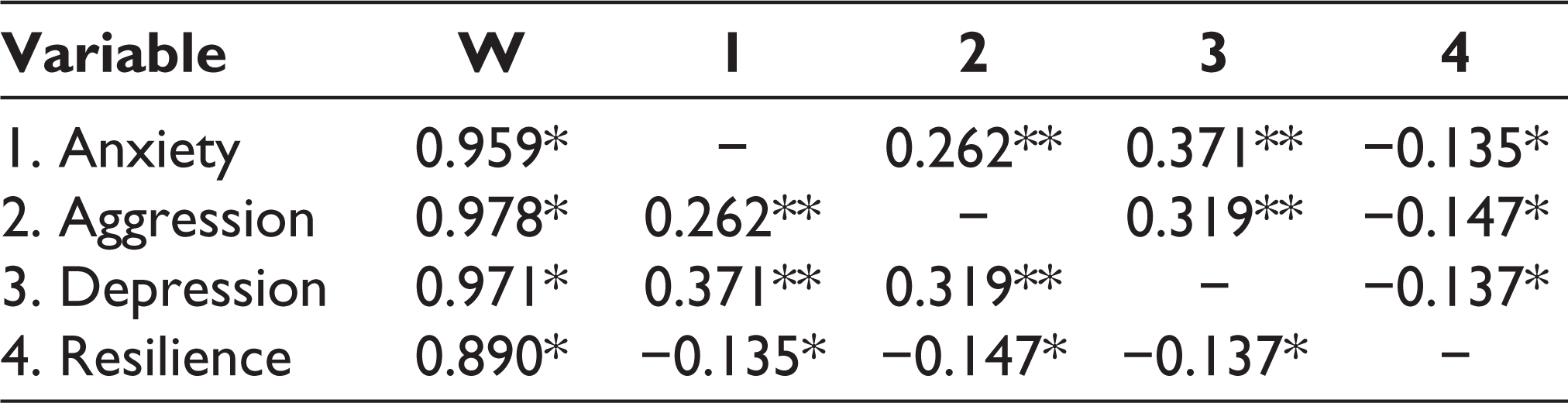
Spearman rank-order correlation was used to analyze the relationship between the emotional health scales namely anxiety, aggression, depression, and resilience among the participants (Table 1). A significant positive relationship was found between anxiety and aggression (r = 0.262, P < .01) as well as anxiety and depression (r = 0.371, P < .01). Also, aggression and depression are positively related (r = 0.319, P < .01). Resilience is found to be negatively related with anxiety (r = −0.135, P < .05), aggression (r = −0.147, P < .05), and depression (r = −0.137, P < .05).
Relationship Between Emotional Health Scales Among Survivors of CSA
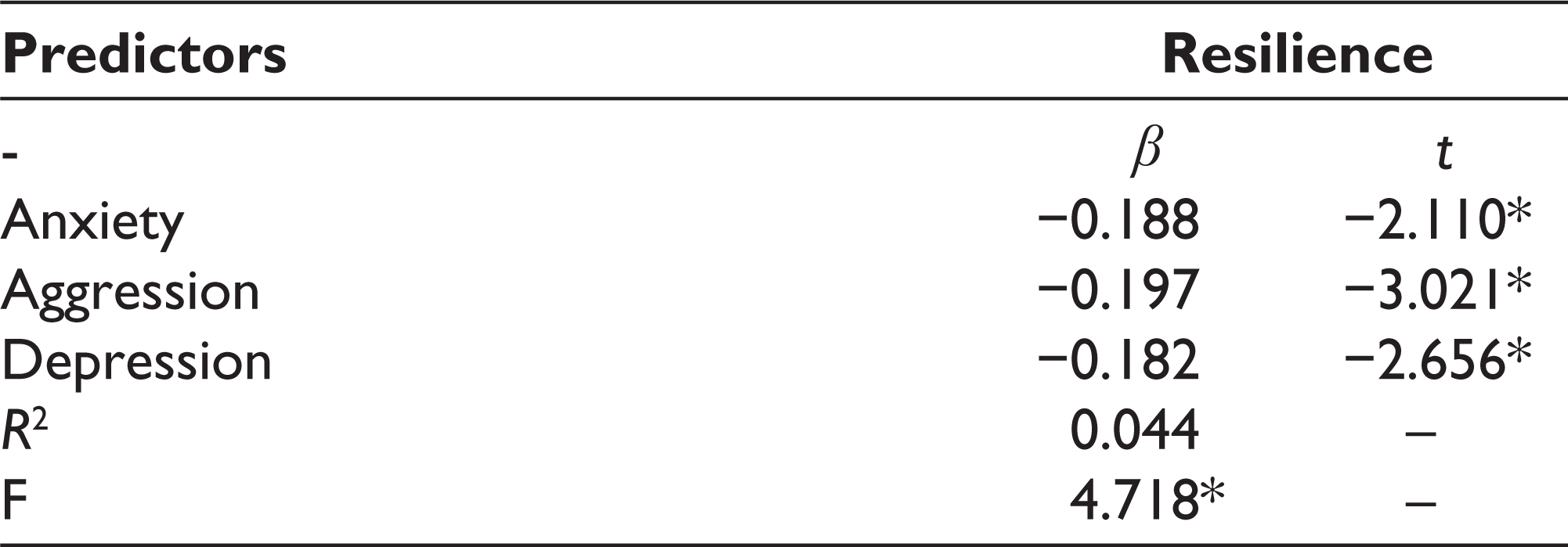
In order to understand the predictive role of anxiety, aggression, and depression on resilience, linear regression was carried out (Table 2). Anxiety (β = −0.188, t = −2.110, P <.05), aggression (β = −0.197, t = −3.021, P <.05) and depression (β = −0.182, t = −2.656, P <.05) were the negative predictors of resilience and they explained 4.4% of the variance in the resilience of the participants (R 2 = 0.044, F = 4.718, P <.05).
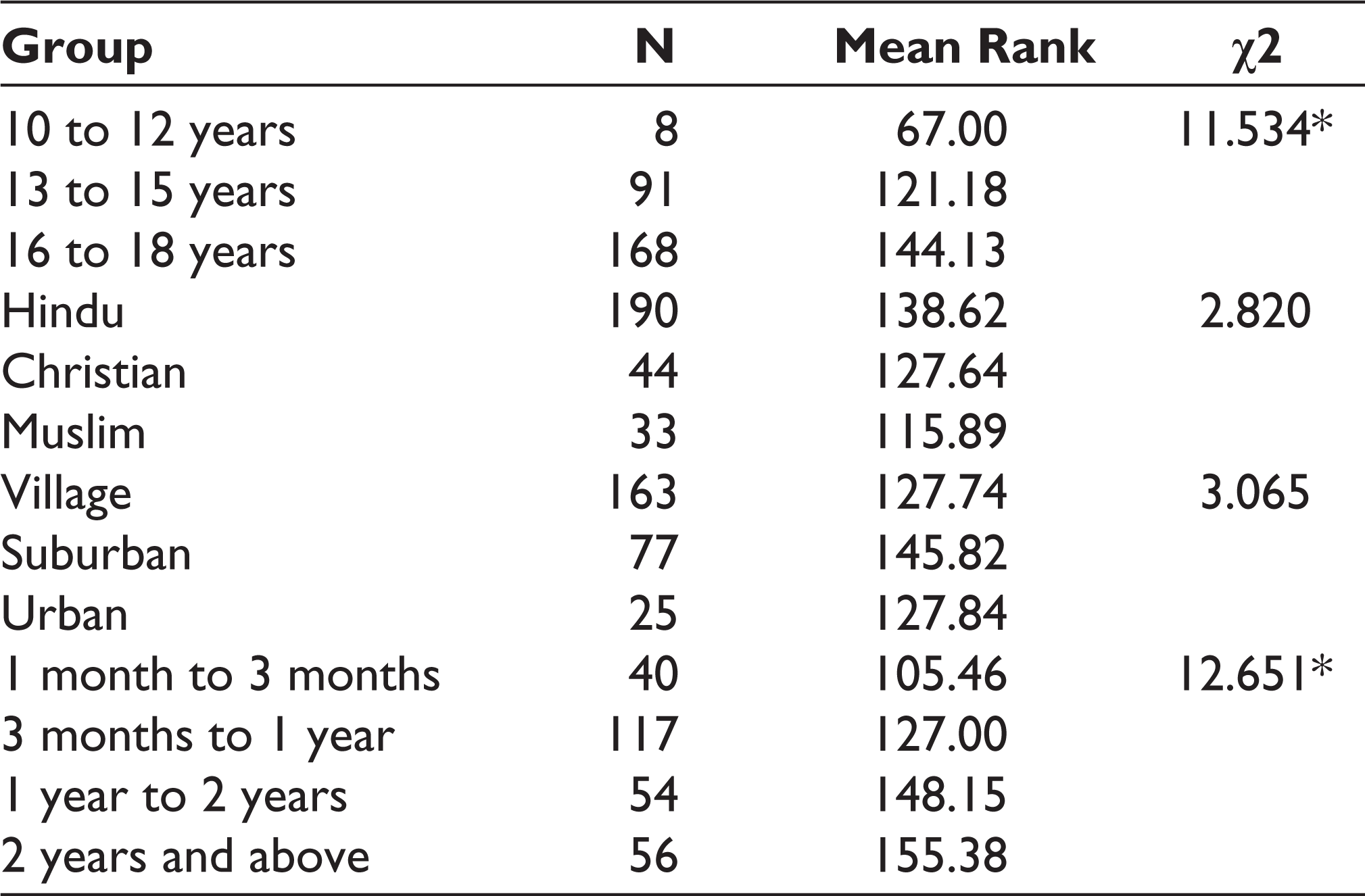
Apart from the emotional health scales, the role of age, religion, birthplace, and duration of stay at shelter homes was compared with resilience. Kruskal–Wallis test was performed (Table 3) and a significant difference was observed in resilience based on the age (χ2 = 11.534, P = .05) and duration of stay at shelter homes (χ 2 = 12.651, P = .037). While comparing mean differences to establish the role of resilience based on religion and birthplace, it was found that resilience of CSA survivors did not differ on the basis of religion (χ2=2.820, P=.50) and birthplace (χ2=3.065, P=.31).
Predicting Resilience Among Survivors of Child Sexual Abuse
Comparing Mean Differences in Resilience Based on Age, Religion, Birthplace, and Duration of Stay
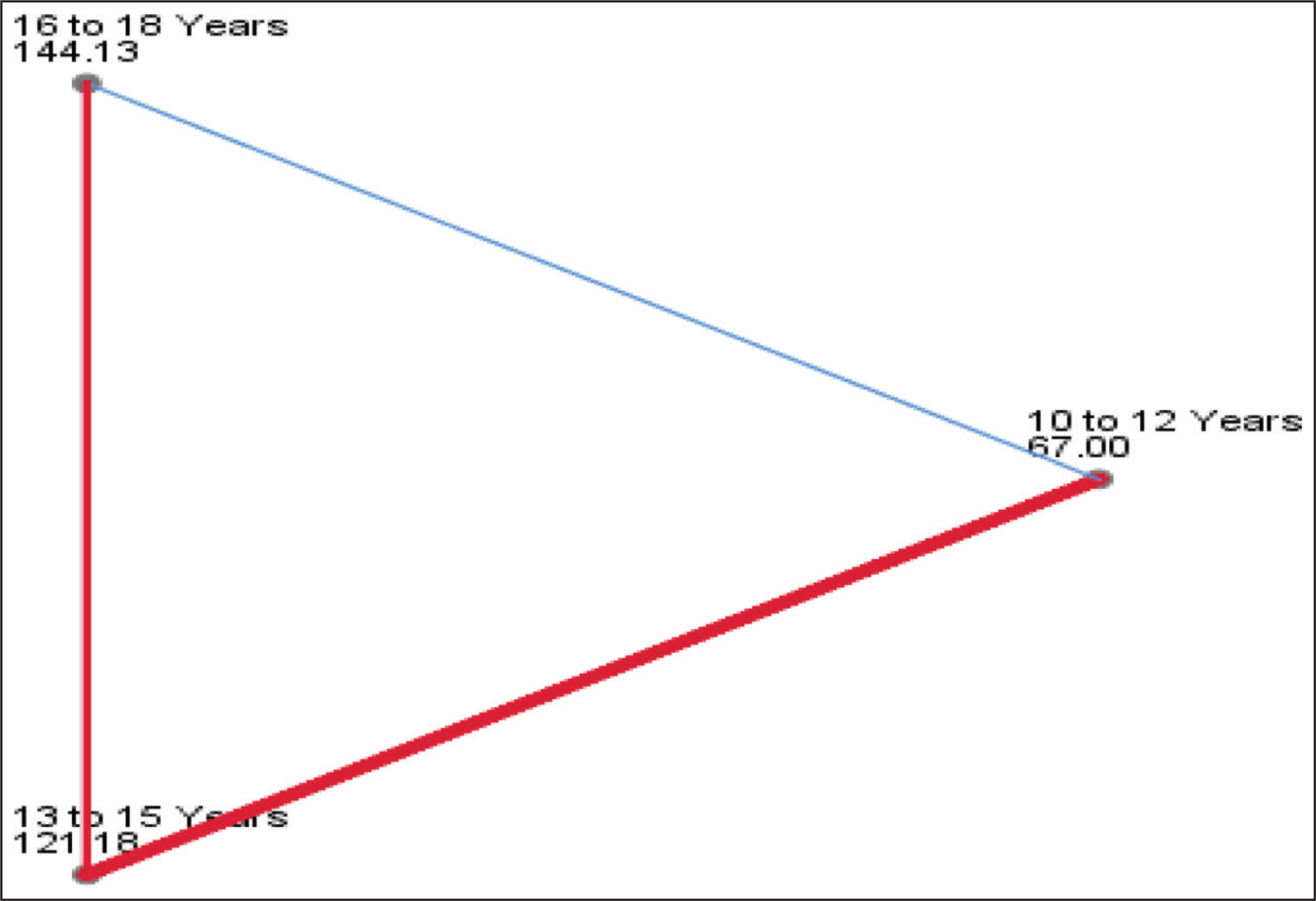
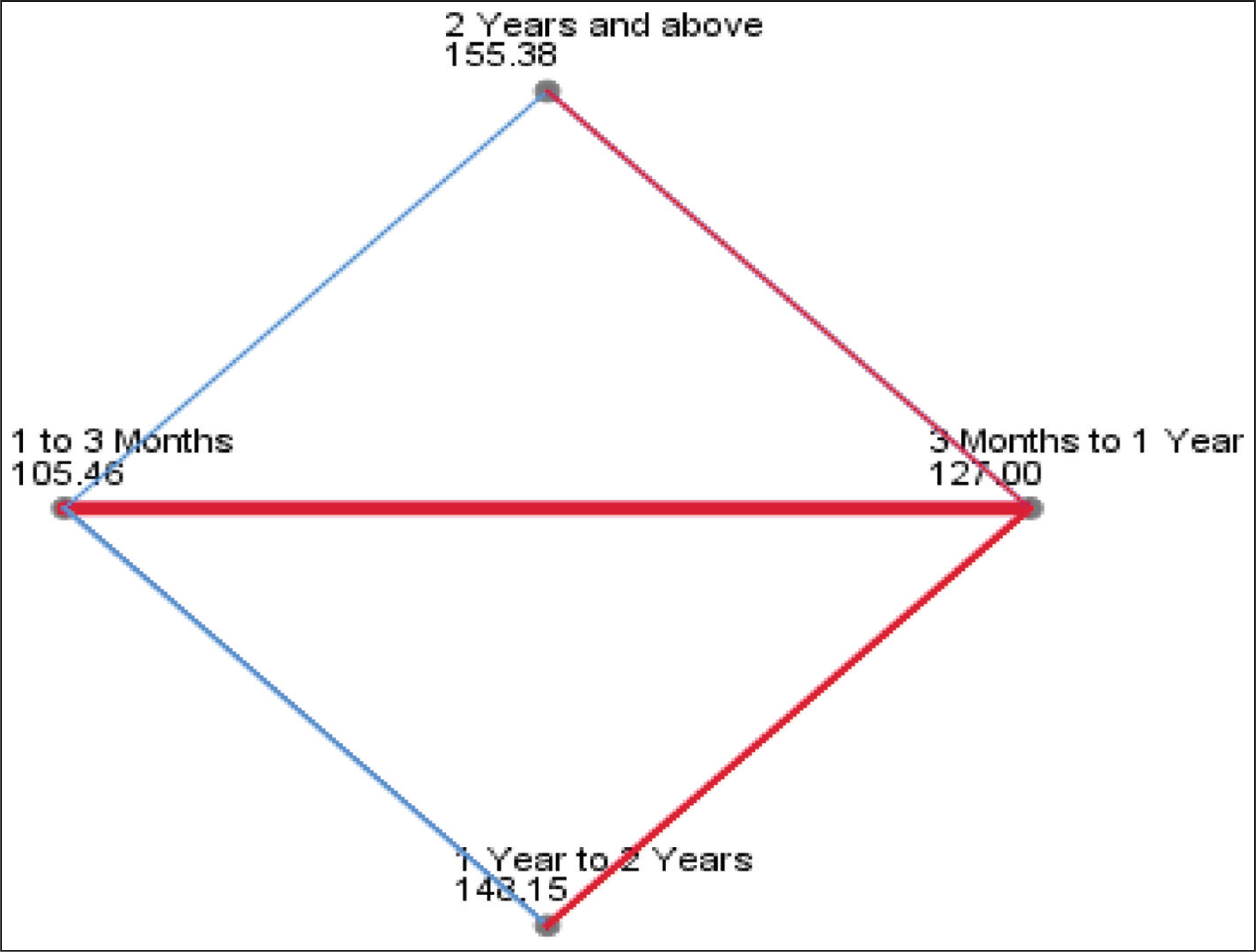
Post hoc analysis was carried out to identify the age groups that differed significantly in their resilience scores. Figure 2 shows the results of post hoc analysis which indicates that a significant difference in resilience existed between the age group of 10 to 12 years and 16 to 18 years (χ 2 = −2.295, P = .022). Thus, resilience is found to be higher for the older age group. As illustrated in Figure 3, post hoc analysis reveals that a significant difference in resilience existed between participants staying for 1 to 3 months and those staying for 1 year to 2 years. Similarly, participants residing for 1 to 3 months and those residing for more than 2 years differed significantly in their resilience scores (χ 2 = −2.431, P = .045). That is, compared to participants who have been staying for less than 3 months, those who have been staying for 1 year to 2 years and more than 2 years had higher resilience.
Post Hoc Analysis of Resilience Based on Age
Post Hoc Analysis of Resilience Based on the Duration of Stay
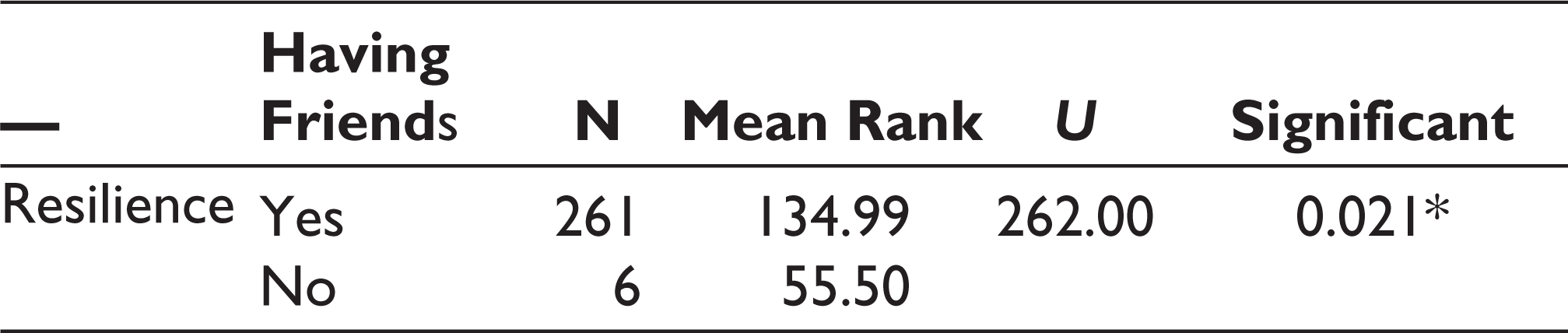
To compare differences in resilience between participants who had friendships and those who reported not having friendships, the Mann–Whitney U test was carried out. Results, as shown in Table 4, indicated that resilience differed significantly based on whether the participants developed friendships or not (U = 262.00, P = .021). Participants who had friendships showed higher resilience.
Comparing Mean Differences in Resilience Based on Having Friends
Discussion
CSA is rampant 13 and the culture-imposed taboo and discrimination, and inadequate and unsafe family environments of CSA survivors necessitate institutional support during their rehabilitation. Kerala government’s initiative at protecting CSA survivors in shelter homes was one of its kind. The medical, psychological, and social rehabilitation provided at these shelter homes aimed at rebuilding their confidence and reintegrating them into mainstream society. Thus, this study targeting CSA survivors in these shelter homes has to be placed in the context of this support system, and its findings have to be scrutinized with respect to the rehabilitation services provided at the shelter homes.
The primary result of this study suggests that CSA survivors in shelter homes undergo considerable emotional distress, as they were not emotionally stable. The majority of the participants reported some extent of anxiety and aggression, even though depression was relatively less reported. Generally, CSA is a quiet crime without a proper witness, leaving no physical signs and effectively covered up by perpetrators. Many children do not reveal their abusive experiences, for reasons of shame, a feeling of normalization encompassing the abuse, and dread of reverberation if they reveal the abuse. 23 This lack of visibility of CSA imposes a great deal of emotional trauma upon CSA survivors. The trauma causes severe wounds in the psyche of the survivor and its deep-rooted effects are commonly reflected in internal issues like self-blame, internalization of sexual experiences, feelings of regret, powerlessness, helplessness, and insecurity, and most importantly, not perceiving the experience as abuse at all.16–18 Thus, the present result signals the fact that the current rehabilitation services are not adequate to deal with the emotional issues of the participants. This calls for the need for more extensive and consistent mental health support for the children to cope with emotional distress. However, the finding that more than 90% of the children reported average to very high resilience signals the benefits of social support and motivation provided in the shelter homes. Individualized care, positive peer interactions, motivational training, and career orientation programs provided in these homes can potentially boost the resilience of children, even though factors other than those pertaining to institutionalized care may be at work.
An in-depth analysis of the scores from the emotional health scale suggests that the levels of aggression, anxiety, and depression experienced by the participants are positively related to each other. This indicates the pervasiveness, intricacy, and multifaceted nature of the emotional issues faced by CSA survivors. Several pieces of research have already established anxiety, depression, and other internalizing problems as the psychological consequences of CSA7, 19 and the result of this study conforms to them. Aggression, because of its externalizing nature, is a matter of special concern. Research shows that externalizing problems in CSA survivors can potentially lead to risky behaviors in adolescence like alcohol use and sexual intercourse, which may be attributed to the experiences of betrayal and stigma and the resultant tendency to detach from conventions. 24 Thus, if not appropriately managed, aggression can have devastating long-term consequences in the lives of CSA survivors. Hence, integrated psychological support, uniquely addressing the internalizing and externalizing problems of each child, is the need of the hour.
The negative relationship of the emotional health scales of aggression, anxiety, and depression with resilience is a finding that was subjected to further analysis for their predictive role. All the 3 variables–aggression, anxiety, and depression–caused significant negative effects on the resilience of CSA survivors. This finding constantly reminds us of the central role taken by mental health in driving the positive adaptation of trauma survivors. A recent study by Fuller-Thomson et al (2019) 10 suggests that the strongest predictor of complete mental health and resilience in adult CSA survivors was lifetime depression, followed by other factors including anxiety. Aggression has always been negatively related to resilience and its detrimental effects on the psychosocial adaptation and well-being of CSA survivors are beyond question.24, 25
In this study, the participants reported high resilience, at the same time, expressed significant levels of emotional distress, which was found to affect their positive adaptation as well. Initially, these findings may seem to be contradictory, but it is not surprising as the multidimensional nature of the construct of resilience provides a justification for this seemingly controversial finding. As Luthar et al 8 have reviewed, there are studies in which adolescents, who have been through adversities, overtly demonstrated successful adaptation but struggled covertly with psychological problems like depression. The construct of resilience encompasses multiple conceptually related and unrelated domains, and adjustment in one domain does not necessitate an adjustment in another unrelated domain. The participants of this study have been receiving rehabilitation programs and activities in the shelter homes that promote their growth and development and orient them toward their future. As a result, they are likely to report to be highly ambitious, optimistic, achievement-oriented, self-sufficient, and socially competent. However, their underlying trauma-induced conflicts and emotional issues may remain largely unattended and unsettled and reflect in high scores on emotional issues like anxiety, depression, and aggression, despite high resilience. This can be taken as a methodological limitation of this study, as the assessment of resilience was not comprehensive enough to account for its multiple dimensions. Moreover, understanding resilience as a continuous growth process puts forth the idea that “being resilient doesn’t mean that a person won’t experience difficulty or distress.” 26 Resilience involves staying flexible while going through difficult times in life and bouncing back to normal functioning. A resilient person lets herself experience strong emotions during stressful and traumatic events, at the same time knows how to get back to a balanced state of functioning.
In addition to the emotional health variables, sociodemo-graphic variables were also analyzed. First and foremost, emotional health was significantly different based on the age of the participants. Participants who were aged 16 to 18 years were more resilient than 10 to 12-year-old ones. Studies have yielded mixed results on the effects of age on resilience and coping strategies of children and adolescents.27, 28 Although Sun and Stewart 29 have reviewed a few studies that depicted age-dependent increases in resilience factors like self-esteem, their cross-sectional study found that younger children scored high in terms of several resilience factors like communication, empathy, autonomy, prosocial peer relations, etc than adolescents. The researchers suggest the role of adolescents’ increasing expectancies and beliefs about peer-oriented and familial patterns of support, which they learn to be vital for success, problem-solving, and emotional development. In this study, the ascending trend of resilience with respect to age may be attributed to the facilitative environment, enriched by peer support, provided in the shelter homes.
Another finding of the study is that religion and place of residence do not produce any significant difference in the resilience of the participants. In 2006, Edmond et al 11 investigated 99 sexually abused adolescents living in the foster care system and found that resilient girls were more certain of their educational plans, were more optimistic about their future, and had more positive peer influences. However, family support and religion had no significant influence on their resilience. These results suggest that foster care systems orient children toward their future, support them in overcoming their familial and social predispositions, and treat them uniformly, irrespective of their religious and family backgrounds. Similarly, in the shelter homes of this study, children were not experiencing any discrimination based on their religion or place of residence, all of them get equally motivated toward their future goals and hence display no differences in resilience based on their religion or locality.
The effectiveness of the rehabilitation services offered at these shelter homes is further established by the duration of stay of the participants. Children who have been at the shelter homes for less than 3 months were relatively less resilient than children who were there for more than 1 year. And as the duration increased to 2 years, resilience improved considerably. Studies that evaluated the effectiveness of foster care homes and out-of-home placements have found that natural mentoring relationships existed in these institutions and played a promotive role in resilience. In such contexts, children developed a sense of belongingness, and the outcomes are reflected in their hope and current life skills. 12 The present finding is thus consistent with the existing literature and thereby acknowledges the promising role played by the shelter homes of Kerala.
The last variable investigated for the role in resilience, adds a golden feather to the results of this study. The presence of friendships in the lives of the participants was found to have a strong difference in their resilience. This is an expected finding, but highly important as the presence of a confidant in life was found to be the second strongest element of complete mental health in CSA survivors. 10 Moreover, positive peer influences in foster care systems promoted resilience among CSA survivors. 11 . Most importantly, several studies and peer interventions have discovered that having a friend can buffer CSA child survivors from the effects of stress, reduce their risky behaviors, and prevent victimization in later life. 30 Thus, the present finding enlightens that peer relations within the shelter homes become instrumental in promoting their psychological well-being.
Limitations
The nongeneralizability of the findings of the study, as it was limited to a group of CSA survivors living in shelter homes, is an obvious limitation of this study. In addition, the lack of a multidimensional assessment of resilience and not accounting for resilience-building factors other than those within the institutional care system also pose a serious limitation of the study.
Conclusion and Recommendations
This study throws some important insights into the current rehabilitation efforts being implemented in Kerala. The efforts have been successful in building the resilience of CSA survivors and driving them toward an optimistic future. However, adequate attention to the multiple emotional issues faced by them is lacking and its consequences can potentially create long-standing maladjustments across their personal, social, and professional lives. Integrated mental health support should be offered, regularly and systematically. The institutional support provided at the shelter homes has been found to be highly facilitative, as evident in the effects of several sociodemographic variables, particularly the duration of stay. The most promising result comes from the role of age as it implies that however devastating the trauma is, adequate support can bring survivors back to a positive, confident, and independent life. Moreover, the significant role of peer relationships sheds light on the future directions of support mechanisms offered at these shelter homes. The introduction of peer-based interventions and peer mentors can be a source of support and inspiration for CSA survivors to wither away from the emotional trauma and rebuild their futures.
Authors’ Contributions
All 5 authors contributed to the development of this manuscript. TMT and JAM conceived the initial review and developed the manuscript. TMT, SG, and UAS conducted a methodological analysis of the studies and involved drafting the manuscript. JAM and BPP provided expert support concerning future intervention research and critically commented on the paper.
Footnotes
Acknowledgements
This paper and the research behind it would not have been possible without the exceptional support of research assistants, participants of the study, administrative staff of the shelter homes, and Dr Baiju Gopal and Dr Justin K James in data analysis.
Declaration of Conflicting Interests
This paper is a part of a larger research project funded by the Department of Women and Child Development, Government of Kerala. The authors declared no competing interests concerning study design, collection, analysis, and interpretation of data, report writing, and publication.
Funding
The research study is part of a research consultation initiative funded by the Department of Women and Child Development, Government of Kerala. The findings were given to representatives of the funding agency once the project was completed, and permission to publish them was granted..
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.