
Abstract
Keywords
Finkelhor and Berliner [1] have reviewed published research into the treatment of sexual abuse. Casting their net very broadly, they were able to locate 29 studies that used pre- and post-standardised measures to assess change in the sexually abused child or parent following treatment. Sample sizes varied widely (from five to 156), as did age range (from 3 to 18 years) and sex of subjects (13 involved female subjects only; two included only male subjects; and 14, both sexes). Seventeen studies were uncontrolled and five were quasi-experimental. Only seven of the studies reviewed by Finkelhor and Berliner involved random assignment to an experimental treatment program and a comparison or control group.
The methods of treatment employed in these studies varied considerably: music therapy, drama therapy, structured or psychodynamic group therapy, family therapy, individual or group cognitive–behaviour therapy, stress-inoculation and graded exposure therapy, psychodynamic individual psychotherapy, multifaceted therapy, crisis intervention, non-directive supportive therapy, and ‘mixed, unspecified’ treatments. The standardised measures used in these studies to estimate the effect of treatment varied widely; for example, the following variables were assessed: self-confidence, depression, anger, emotional pain, hostility, anxiety, posttraumatic stress disorder, avoidance, dissociation, sexual concerns, self-esteem, self-concept, social competence, locus of control, maternal depression, parental psychopathology, family conflict and parental practices.
Of the 17 uncontrolled studies, 13 found significant improvement from pretest to post-test. Of the five quasi-experimental studies, three found that the experimental program had produced a more favourable outcome on post-test than a comparison or no-treatment group. Of the seven fully controlled studies, four demonstrated the superiority of one treatment over its comparison or no-treatment control group. The controlled studies (together with two more recently published) will be described in more detail in this paper.
Controlled studies
Three [2–4] of the nine controlled studies we could find have not been published other than in
Baker [2] compared the effect of a 10-week individual psychotherapy program (n = 15) with that of a 6-week group therapy intervention (n = 24) on female outpatient abuse victims, 13–17 years of age. Standardised measures of self-concept, anxiety and depression were employed. The results of group therapy exceeded those of individual therapy with regard to self-concept but not anxiety or depression.
Burke [3] compared the effect of a 6-week structured group therapy program (n = 12) with that of a waiting list no-treatment control group (n = 13). Subjects were female outpatients, 8–13 years of age. At the end of treatment and at follow up, the treatment group exhibited less psychopathology than the control group on standardised measures of emotional distress, anxiety and depression.
Perez [4] compared the effects of a 12-week individual play therapy program (n = 18), a 12-week group play therapy program (n = 21), and no-treatment (n = 16) on outpatient subjects of both sexes, 4–9 years of age. Both treatment groups exceeded no-treatment in regard to standardised measures of self-concept and internalised locus of control, but there were no significant differences between the effects of the two treatment groups.
Verleur
Monck
Berliner and Saunders [7] compared a 10-week sexual-abuse-specific structured educational group therapy program (n = 48) with a similar program to which were added stress inoculation and graded exposure (n = 55). The subjects referred were outpatients, of both sexes, aged 4–13 years. The programs were modified appropriately for 4–6, 7–10, and 11–13 year olds. In both groups, each week's session was devoted to a different topic (e.g. expressing feelings about the abuse, the offender, family and friends; the impact of disclosure; self-esteem; body awareness and sexuality; and prevention and termination of unwanted contact). In the second program, stress inoculation, progressive relaxation exercises, the ‘quieting reflex’, thought-stopping skills, and graduated exposure were added to the structured educational program. Both treatment programs were manualised, and all treatment sessions were audio-taped and checked in order to ensure treatment fidelity. The outcome was assessed at pretest, post-test, 12 months, and 2 years with six standardised instruments related to general fears, fears related to sexual abuse, anxiety, social competence, general symptomatology, depression and sexual behaviour. Participants in both groups improved significantly in anxiety, depression, general symptomatology and sexual behaviour, but not in general or abuse-related fearsor social competence. However, there were no significant differences between the two groups in the magnitude or rate of improvement on any of the measures. A subset of children (5–15%) deteriorated over the 2 years, while another subset did not improve. Berliner and Saunders raised the question of whether children who are asymptomatic at pretest should be treated.
Deblinger
Cohen and Mannarino [9] compared the effect of a 12-week, abuse-specific, structured, cognitive–behaviour therapy program (n = 33) with that of a 12-week, non-specific, non-directive supportive program (n = 28). Subjects were referred outpatient children of both sexes aged 3–6 years, who had been sexually abused. The cognitive–behaviour therapy program involved both parent and child. Parental objectives involved resolving the following issues: ambivalence concerning belief of the child; parental feelings toward the perpetrator; attributions concerning the abuse; feelings that the child is damaged; management of inappropriate child behaviour, fear and anxiety; and the parent's experience of abuse (if appropriate). The child's objectives concerned: safety; assertiveness; learning the distinction between appropriate and inappropriate touching; abuse attributions; resolution of feelings toward the perpetrator; reducing regressive behaviour; and coping with fear and anxiety. The cognitive–behaviour interventions employed included cognitive reframing, thought stopping, the use of positive images, contingency reinforcement, parental training and problem-solving. The contrasted non-specific treatment program was designed to provide support, build rapport, and encourage the expression of feeling through empathy, reflective listening, supportive statements and clarification. Clinicians were trained specifically in one or other program. Both treatment programs were manualised and the fidelity of treatment implementation checked by audio-tape. Subjects were assessed at baseline, at completion of treatment, and at 12-month follow up, using standardised measures of social competence and general symptomatology, sexualised behaviour, and a parental count of the frequency of episodes of problematic behaviour during the previous week. There were significant differences in outcome between the effects of the two treatment programs: cognitive–behaviour therapy was superior in regard to its effect on total symptomatology, internalising symptoms, sexualised behaviour and weekly-recorded problematic behaviour.
Cohen and Mannarino [10] have recently compared the effectiveness, for adolescents, of a 12-week cognitive–behaviour program (n = 30) with that of a 12-week non-specific therapy program (n = 19). Subjects were outpatients of both sexes aged 7–14 years, referred within 6 months of having experienced independently validated sexual abuse. Treatment outcome was assessed before and after treatment with standardised measures of symptomatology and social competence, anxiety, depression, and sexual behaviour. The cognitive–behaviour therapy program targeted depression; anxiety; the connections between thoughts, feelings and behaviour; and inappropriate behaviour associated with the abuse. The cognitive–behaviour therapy program also addressed parental emotional distress and guilt, the capacity of the parent to provide adequate support to the child and parental behaviour management. Both treatment programs were manualised, and the fidelity of implementation monitored by audio-tape. Therapists switched programs at the midpoint of the study. The cognitive–behaviour program exceeded the non-specific program in regard to depression and social competence but not sexual behaviour, symptomatology, or anxiety. The drop-out rate from this study was high (40%), particularly from the nonspecific therapy group, and may have been responsible for the somewhat disappointing results.
Recommendations
After their review of treatment research in child sexual abuse, Finkelhor and Berliner [1] came to the following conclusions. Some abused children, despite treatment, either do not improve or get worse. The optimal duration of treatment is unclear, and the drop-out rate a serious problem. Given the diversity of psychopathology following child sexual abuse, it is unlikely that one kind of treatment will suit all. It is unclear whether (or which) asymptomatic children should be treated. Boys are harder to treat than girls. Finally, intrafamilial sexual abuse usually occurs in a setting of personal, familial and community problems all of which may need therapeutic intervention.
Finkelhor and Berliner [1] recommended the following directions for future research. There is a need for properly controlled studies, with sufficiently large sample size, followed for a sufficiently long time. The index treatment or treatments should be specified, abuse-specific and implemented with high fidelity to the design of the treatment. Pre- and post-follow up measures are required, from a variety of sources, tapping the full range of abuse-related phenomena. The non-offending parent needs treatment as well as the child. Sexualised behaviour, aggression, impulsivity and depression probably require targeted intervention because, although these behaviours may arise from the abuse experience, they are self-perpetuating. Finally, treatment should be based on an explicit conceptual model of the psychopathology of child sexual abuse. The treatment program to be described next addresses all these recommendations.
The University of Queensland program for the treatment of child sexual abuse
The University of Queensland (UQ), in collaboration with Protect All Children Today (PACT) (Queensland), has been funded by the National Health and Medical Research Council (NHMRC) to develop treatment programs and evaluate the impact of treatment for child sexual abuse. As our therapists are trained community clinicians, this is not a laboratory-based
Conceptual model
The UQ/PACT Project is based on a modification of Spaccarelli's [11] transactional model described in the previous paper. In this model (see figure 1),
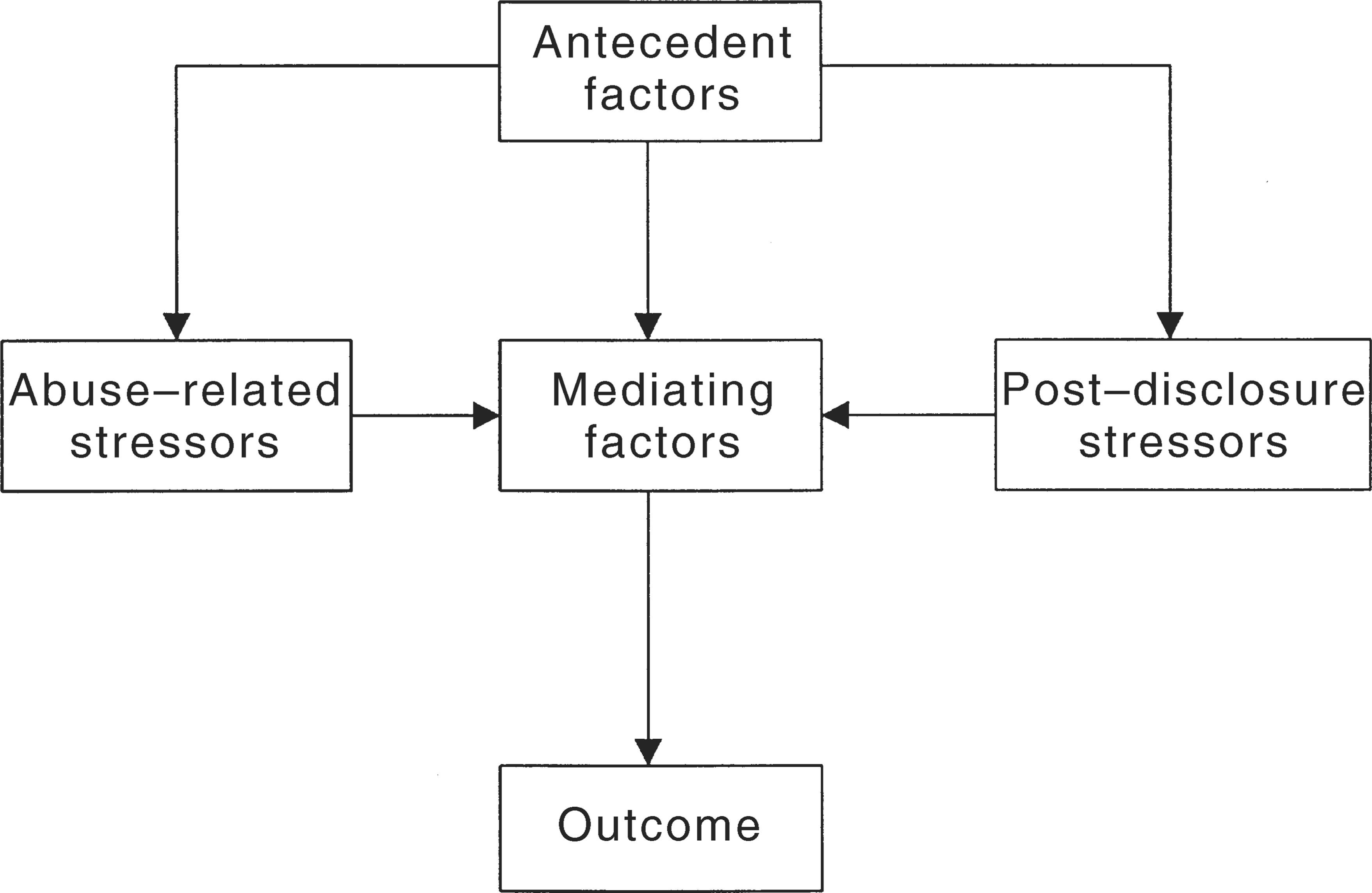
A conceptual model of the pyschopathology of child sexual abuse.
As treatment intervention cannot affect antecedent or abuse-related factors, it must target post-disclosure stressors and mediating factors, for example: (i) the quality of parental support; (ii) parental attributions about the abuse; (iii) parental psychopathology (especially reactivated conflict concerning past sexual abuse) as reflected in parental coping style; (iv) the stress of the child of testifying in court; (v) maladaptive attitudes toward the self (e.g. of being to blame for the abuse, of being bad or damaged or of being powerless); (vi) maladaptive attitudes to others (e.g. that others cannot be trusted or that they must be placated sexually); (vii) traumatic state (as manifest in posttraumatic stress disorder); (viii) dysregulation of affect, impulse and self; and (ix) maladaptive coping style (particularly denial, suppression, avoidance, dissociation, externalisation and inappropriate tension-reduction).
Successful treatment, therefore, should be reflected in an improvement in, or alleviation of, the above problems, together with the adoption by the child of a more adaptive coping style (i.e. disclosure, support-seeking and cognitive restructuring).
Sample
Subjects are victims of substantiated cases of sexual abuse, of either sex, 6–16 years of age, referred from the police or child protection (SCAN) teams in south-east Queensland. Exclusion criteria are as follows: children with verbal IQ less than 70; those who are not living with a caregiver; those who are expected to testify in court; those who continue to live at home with the offender; and those whose experience of sexual abuse occurred over 2 years before referral. We plan to recruit 200–300 families over an 18-month period.
Treatment programs
This study compares two contrasting, 18-week, manualised treatment programs: a cognitive–behaviour therapy program and a family therapy program.
The cognitive–behaviour therapy program progresses in three 6-week phases. In Phase I,
The family therapy program is derived from cybernetics-based and structural family therapy. It, too, has three 6-week phases. Phase I,
The two programs differ in that the family therapy program keeps child and parent together throughout the 18 weeks, whereas the cognitive–behaviour program separates them in Phase II. The cognitive–behaviour therapy program uses graded imaginal exposure in Phase II and a combination of cognitive–behaviour therapy techniques and behaviour modification in Phases II and III. In contrast to the cognitive–behaviour therapy program, the family therapy program does not ask the child to examine traumatic memories and their associated affects and does not use cognitive–behaviour techniques to deal with such issues; instead, if the child's traumatic memories emerge in the course of treatment, they are dealt with by externalisation, reframing and stress management.
Theoretically, the cognitive–behaviour therapy program should have an impact on outcome superior to that of the family therapy program because it directly addresses sexual trauma by the use of specific therapeutic techniques.
Clinicians
The clinicians who implemented the two programs have been recruited from 14 different child and youth mental health clinics and from three non-government agencies in south-east Queensland. Each clinician is trained in a 3-day workshop to implement one of the two programs. Treatment fidelity will be assessed by random audio-tape audit of different therapeutic sessions.
Evaluation
At baseline, 18 weeks, and 12 months the following domains are assessed: parental psychopathology; the parent's reaction to the child's disclosure of abuse; the child's social competence and general symptomatology; dissociation; posttraumatic symptomatology; anxiety; depression; sleep disturbance; hyperactivity; aggressiveness; sexualised behaviour; attitudes to self, others and the abuse; attachment; self-esteem; and defensive style. Between Phases II and III, in order to select the foci of Phase III, we check whether or not the child is still exhibiting sexualised, aggressive, or impulsive behaviour.
Conclusion
An analysis of research into the treatment of child sexual abuse suggests that there is, as yet, no convincing evidence that any treatment is effective. Contemporary opinion that cognitive–behaviour therapy represents the treatment modality of choice is based on two controlled studies [9,10], conducted in a labaoratory setting, with children aged 4–6 and 7–14 years, respectively, whose progress was assessed by a relatively limited evaluation system, and on a third controlled study [7] that focused primarily on whether child or parent should be treated alone or together. In a fourth controlled study [6] with a wider age range (4–13 years), it could not be demonstrated that cognitive–behaviour therapy provided benefits beyond those accrued by educational group therapy.
As Finkelhor and Berliner [1] point out, aside from the preferred modality of intervention, the desired duration and frequency of therapy are unclear. Other uncertainties concern the context of treatment. Should therapy be conducted in an individual, family or group context? Is it essential (or even desirable) in all cases for the child to explore his or her memories concerning the abuse experience? When (if ever) should treatment be offered to an asymptomatic child? How should parental psychopathology (particularly emotional disturbance arising from unresolved conflict concerning past sexual abuse) be dealt with? Should parental problems be part of the child's therapy or should the parent be referred elsewhere for treatment? How should the therapist deal with the child's past or present exposure to emotional neglect, lack of intellectual stimulation, physical abuse, or domestic violence: problems that often precede or accompany sexual abuse? Can children with impaired verbal intelligence benefit from psychodynamic psychotherapy or cognitive–behaviour therapy? If not, how can the children be prepared in order to benefit from verbally oriented therapy? Finally, how should the index treatment be controlled? If a no-treatment or ‘usual services’ control group is ethically or politically unacceptable, is it possible or desirable to compare the index treatment with another treatment that is more than a ‘dummy’?
Questions abound. As has already been said, sexual abuse is an experience, not a disorder. Its manifestations and contexts are quite diverse. For these reasons, it is not likely that a ‘one size fits all’ treatment will work. We seek the criteria that will determine how the central model of treatment should be modified to suit the individual case. In the long term, the clinician's task will be to select treatment goals for the particular case and to design an individualised, multifaceted, evidence-based treatment program. This is a technically different task from that associated with designing an experimental treatment program and pitting it against a control or comparison treatment. However, it will not be possible to design individualised treatment plans until it is known what generic treatments work best for which children with which problems.
Finally, it is not clear whether laboratory research can be translated into effective community treatment. Can community clinicians co-operate in multi-centre trials of treatment programs? If they do, it is essential that they adopt the constructive skepticism that characterises the best researchers, and constrain their natural individualism in order to preserve the fidelity of the treatment being tested. No easy matter.
Acknowledgement
The preparation of this paper has been funded in part by the National Health and Medical Research Council project number 990201, ‘Child Sexual Abuse: Evaluation of a Multimodel Treatment Program’.