
Abstract
Background:
Pandemics are known to cause an increase in the prevalence of posttraumatic stress disorder (PTSD). The current COVID-19 pandemic has led to a surge in the same along with other problems such as anxiety and depression.
Aim:
To find out the prevalence of PTSD and other mental health abnormalities among adolescent girls who have contracted COVID-19 infection and the factors associated with it.
Methods:
This was a cross-sectional study carried out for 6 months at RL Jalappa Hospital and Research Center, Kolar. Adolescent girls infected with COVID-19 were included. A total of 100 girls took part in the study after matching inclusion and exclusion criteria. To assess for PTSD, the Mini International Neuropsychiatry Interview-KID (MINI-KID) and CPSS-5 Interviewer Version (CPSS 5-I) questionnaire were used. Data entered in Microsoft office excel were analyzed using SPSS v 22 (IBM Corp., Armonk, NY, USA). To check for the association between factors, chi-square test was applied.
Results:
The majority of girls were aged 18 years, belonged to nuclear families, and had a hospital stay for 7 days to14 days. About 15% of the girls had PTSD diagnosed using two tools. Panic disorder and separation anxiety were commonly seen. Duration of COVID symptoms adolescent girls had before being diagnosed with COVID-19 by RT-PCR and duration of the hospital stay along with symptoms like throat pain, headache, and diarrhea were a few clinical factors that had a statistically significant association with PTSD.
Mental health screening seems to be disregarded in COVID-19 cases. COVID-19 can be a traumatic stressor event among adolescents which can elicit PTSD-like responses and also exacerbate mental health problems.
Conclusions:
Early screening for PTSD or other mental health abnormalities among adolescents post COVID-19 infection should be considered.
Keywords
Introduction
COVID-19 has chaperoned to diverse mental health problems, including anxiety, depression, posttraumatic stress disorder, and other stress-related disorders. The pandemic has triggered an array of emotional, physical, and economic stress and much neglected mental health tribulations. The emerging literature measures the impact of various traumatic stressors related to COVID-19, as well as the effects of less severe types of stress exposures.1, 2 With the COVID-19 pandemic showing incessant trends, living with a fear of infection or post COVID-19 infection stress has become conventional. Posttraumatic stress disorder (PTSD) is a mental health disorder that may develop after exposure to exceptionally life-threatening or horrifying events featuring reexperience, avoiding traumatic memory, and the feeling of continuous threat to be vigilant or over vigilant.3, 4 PTSD has been seen in those who have themselves suffered from serious COVID-19 illness, individuals who, as family members and health care workers, have witnessed other’s suffering and death, individuals who have learned about the death or risk of death of a family member or friend because of the virus, and individuals who have experienced extreme exposure to aversive details.3, 5 COVID-19 infection can act as a potential stressor inducing a major psychological trauma which can emanate sometimes into serious distress and disability in an individual. The neuropsychiatric squeal of COVID-19 delineates a significant clinical challenge that has to be taken into consideration in those who have survived COVID-19 infection. Previous epidemic studies have reported a higher prevalence of PTSD among people exposed to the trauma resulting from an infectious disease epidemic.6, 7 There are very limited research works showing that the COVID-19 pandemic fits into prevailing PTSD and its impact on adolescents. Various studies across the globe have shown that PTSD is more common among the female gender because of inherent biological differences, with women having a higher probability of having PTSD following a stressful event.8–10 With this background, the study was started with the objective to find out the prevalence of PTSD and the clinico-social factors associated with it and other mental health abnormalities like major depressive disorder, social phobia, panic disorder, separation anxiety, specific phobia, and generalized anxiety among adolescent girls who have contracted COVID-19 infection.
Materials and Methods
This was a cross-sectional study carried out for a period of 6 months from January 2021 to June 2021 at RL Jalappa Hospital and Research Center, Kolar, Karnataka, India. As no previously published articles are available regarding PTSD and adolescents infected with COVID-19 infection, 50% of adolescent girls who have contracted the infection having PTSD will be considered as prevalence (p), with error 10% and 95% confidence interval; the sample size was 100. Through RT-PCR, 1594 COVID-19 positive patients were diagnosed at RL Jalappa Hospital and Research Center. Among the 1594 patients, 19 were boys aged from 11 years to 19 years and 116 were adolescent girls found to be positive for COVID-19 (Figure 1).
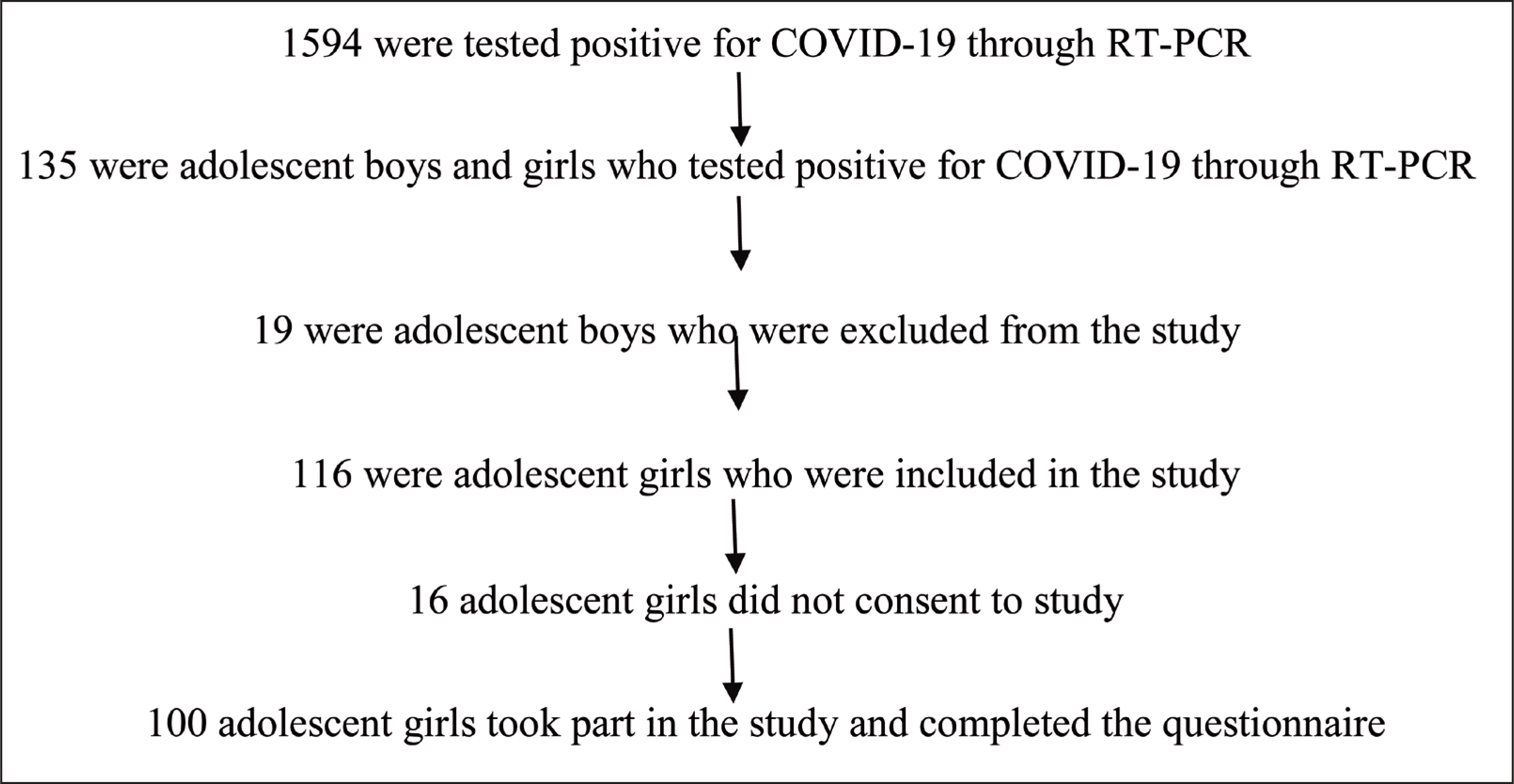
Parents of 16 adolescent girls who tested positive for COVID-19 did not consent to the study, and they belonged to early and mid-adolescence, ie, aged 11 years to 16 years. Adolescent girls with previously diagnosed PTSD for any previous event were excluded. The study was started after obtaining institutional ethical committee clearance. After obtaining consent from parents and assent from adolescent girls, request to participate in the study were mailed through registered E-mail or phone calls; the contact details were obtained from the hospital directory. After obtaining clearance from adolescent girls, the telephonic interview was done at the time they had selected. To assess the sociodemographic details, pretested semistructured questionnaire was used. To assess for PTSD, two tools were used: the Mini International Neuropsychiatry Interview-KID (MINI-KID) and the CPSS-5 Interviewer Version (CPSS-5-I) questionnaire. Data collection was done through telephonic interviews, which lasted for not more than 20 min, by an Assistant Professor in the Department of Community Medicine who had received informal training from a Consultant Psychiatrist and has previous experience using both the tools.
MINI-KID
The MINI-KID is the child and adolescent version of the Mini International Neuropsychiatry Interview (M.I.N.I.). It is a structured diagnostic schedule with Axis-I diagnostic categories. It has been an extremely handy and appropriate psychiatric diagnostic tool and has been used to diagnose PTSD among children and adolescents because of numerous other causes. The MINI-KID generates reliable and valid psychiatric diagnoses for children and adolescents.11, 12 MINI-KID has been widely used in the Indian scenario in diagnosing mental health disorders and in particular PTSD among adolescents.13–16
CPSS-5-I (Child PTSD Symptom Scale)
The CPSS is brief, easy to administer, and available for free. 17 The CPSS-5-I is a 27-item semistructured interview that assesses PTSD and symptom severity in the past month based on interviewer ratings. The CPSS-5-I assesses the history of traumatic experiences to identify an index trauma. Next, the 20 items assessing The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition PTSD symptoms are presented. The interviewer rates each item from 0 (not at all) to 4 (6 or more times a week; almost always) based on the frequency and severity of the reported symptom experienced in the past month related to the index trauma. The total severity score ranges from 0 to 80 and is calculated by summing the ratings of the first 20 items. The CPSS-5-I also yields subscale scores for intrusion (items 1 to5), avoidance (items 6 to7), changes in cognition and mood (items 8 to14), and increased arousal and reactivity (items 15 to 20). Finally, 7 items assess impairment of endorsed. Symptoms on daily functioning pertinent to youth (eg, fun things you want to do, doing your chores, and relationships with your friends).The interviewer rates these items on a scale of 0 (not at all) to 4 (6 or more times a week; almost always), resulting in an impairment score that ranges from 0 to 28. The total impairment score does not contribute to the overall severity score. The total administration time is approximately 30 min.18, 19 Participants positive in both MINI-KID and CPSS-5-I were diagnosed with PTSD. Ethical committee clearance was taken before the start of the study. All data entered in Microsoft office excel sheet were analyzed using SPSS v 22 (IBM Corp., Armonk, NY, USA). Descriptive statistics were applied. To check for the association between factors, chi-square was applied with a level of significance defined as P < .05.
Results
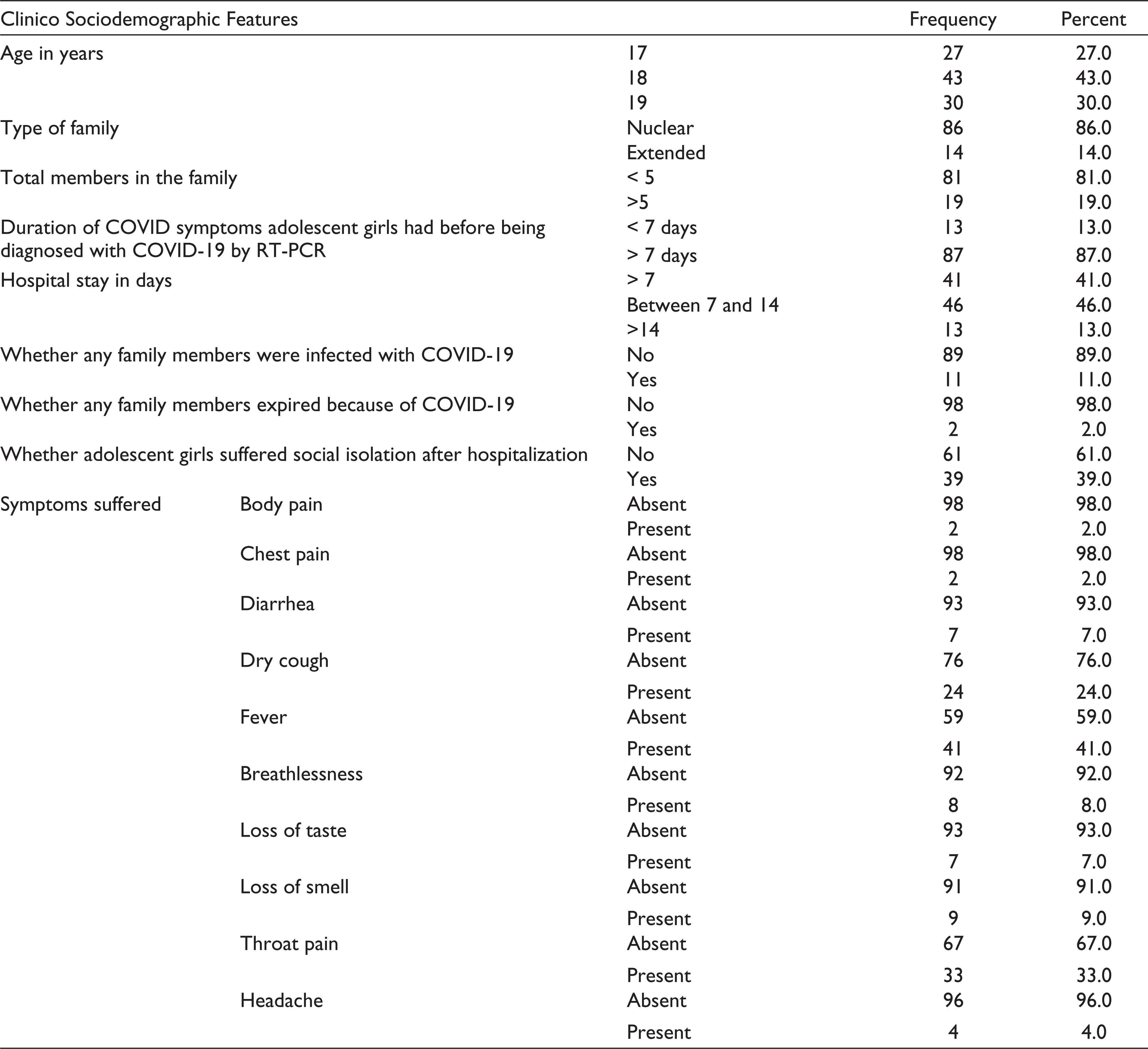
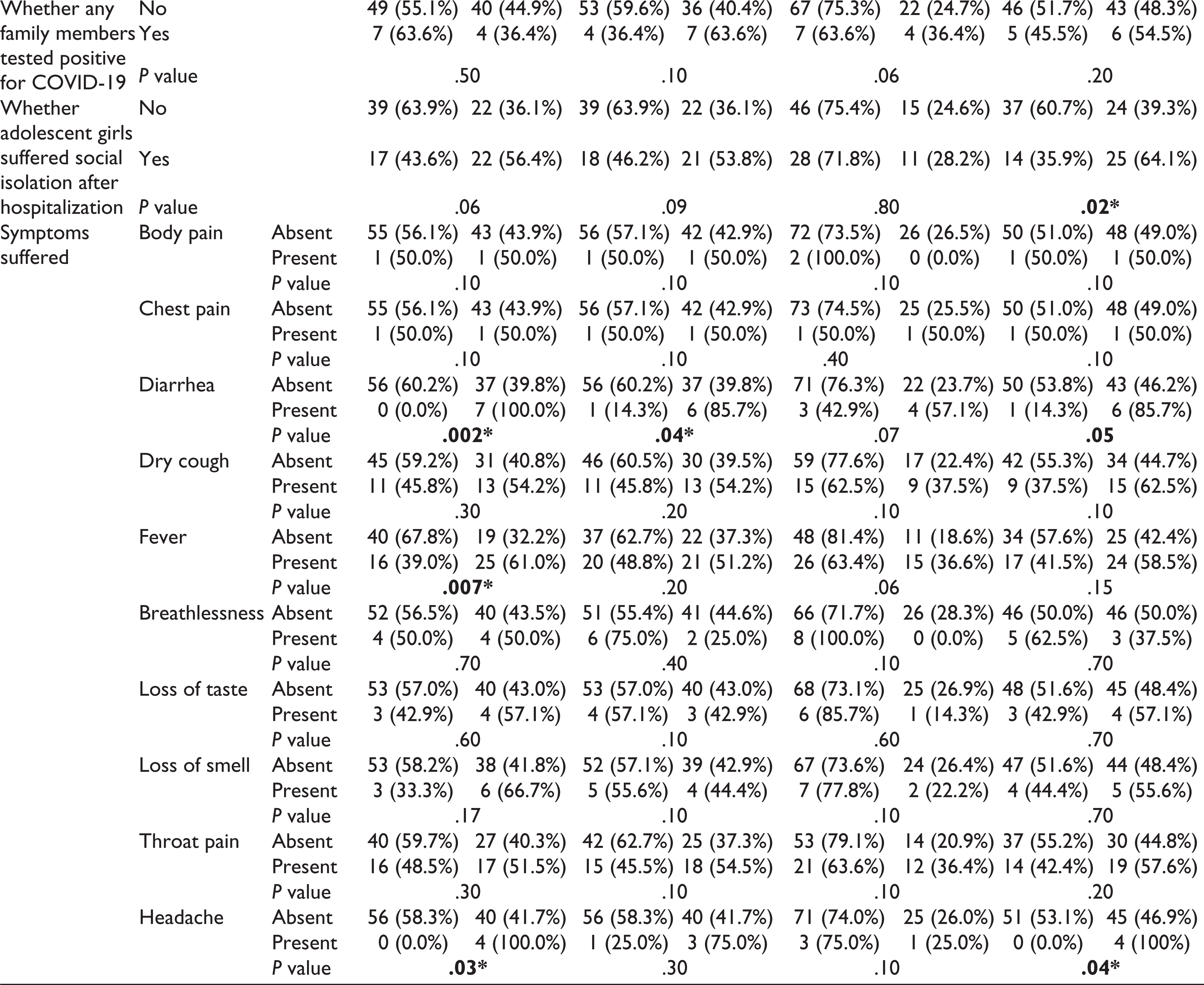
Out of the 100 adolescent girls who took part in the study, 43% were aged 18 years, 86% belonged to nuclear families, 46% had a hospital stay for 7 days to 14 days after diagnosing COVID-19, 39% had suffered social isolation after discharge from hospital, 11% of the participants’ family members were tested positive and were isolated in the hospitals, and 2% participants’ parents died because of COVID-19 infection. Fever and dry cough were the commonest symptoms (Table 1).
Distribution of Adolescent Girls According to Their Sociodemographic and Clinical Features
Out of 100 girls, 18% of girls who had COVID-19 infection were diagnosed with PTSD using MINI-KID and 27% were diagnosed with PTSD using CPSS-5-I.
About 15 (15%) of girls who had contracted COVID-19 infection had been diagnosed positive for COVID-19 using both MINI-KID and CPSS-5-I.
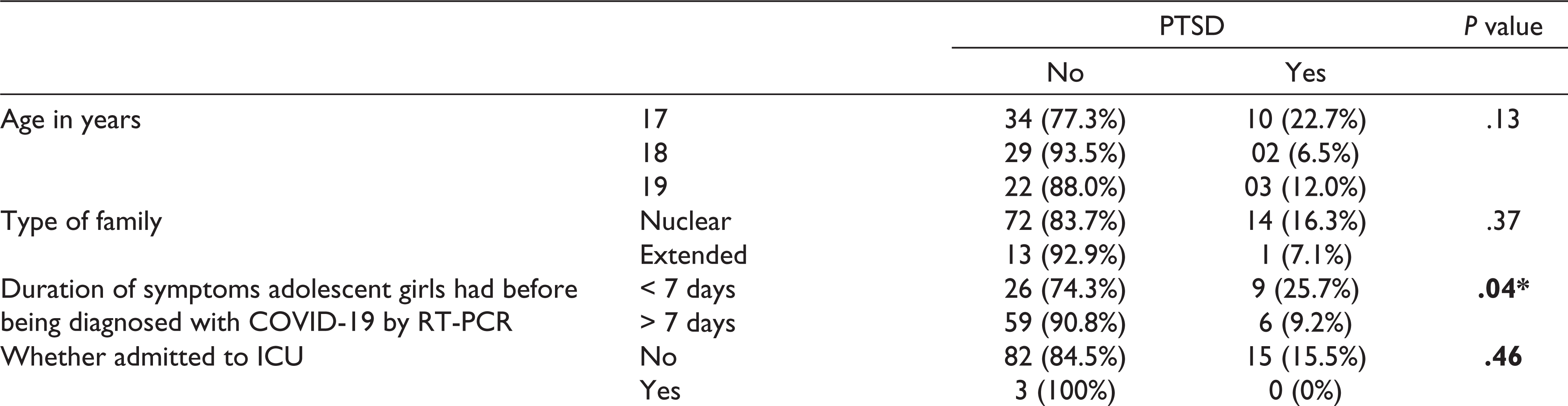
The duration of COVID symptoms the adolescent girls had before diagnosing COVID-19 by RT-PCR, duration of hospital stay, and a few clinical features like throat pain, diarrhea, and headache were found to have a statistically significant association with PTSD (Table 2).
Association of Various Clinico-Social Factors With PTSD
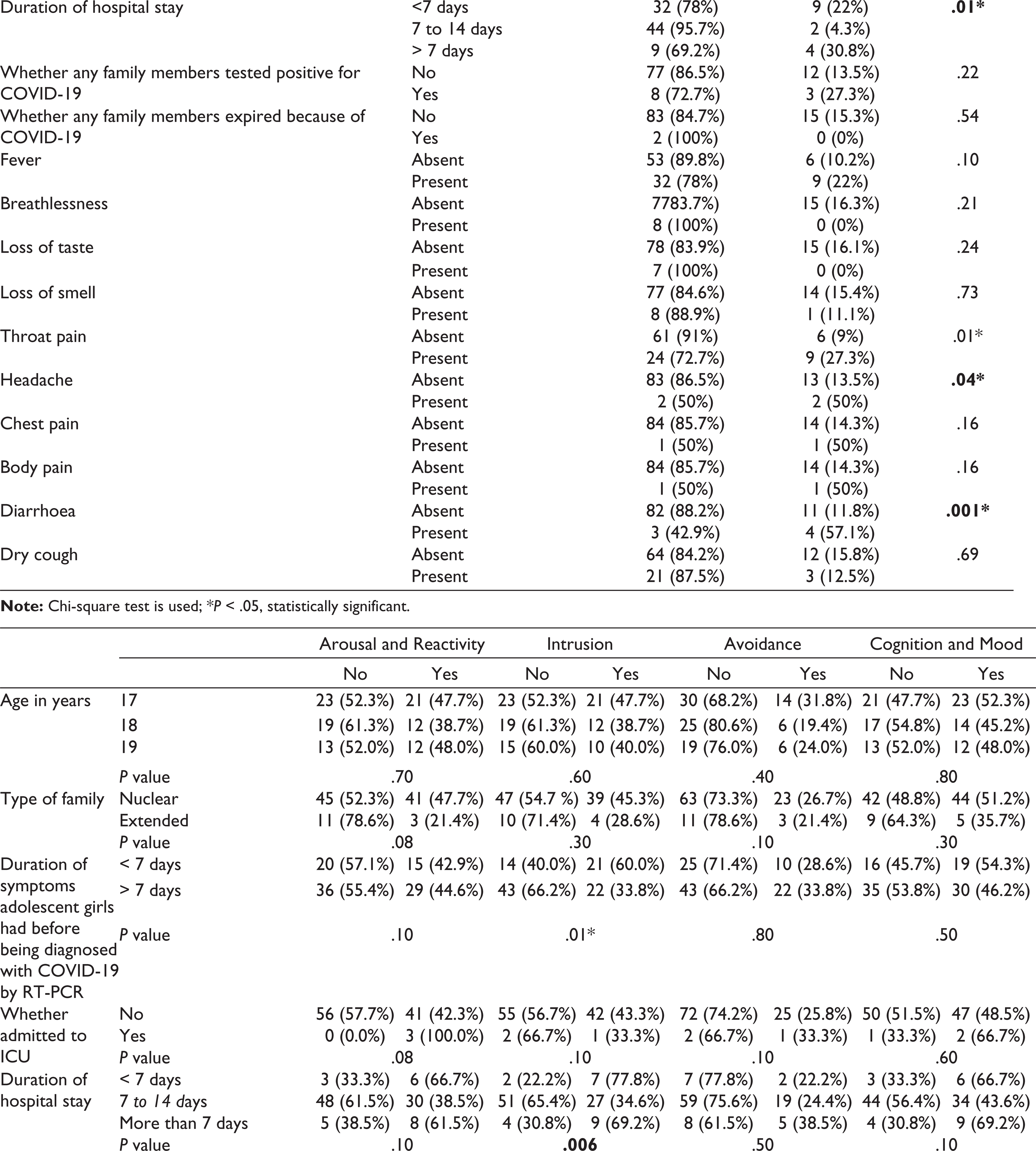
As per the subdomain analysis with CPSS-5I, 44% were found to be positive for arousal and reactivity, 43% for intrusion, 26% for avoidance, and 49% for cognition and mood.
Duration of COVID symptoms the adolescent girls had before being diagnosed with COVID-19 by RT-PCR and hospital stay were the two factors that had a statistically significant association with the intrusion subdomain. Fever and headache were the two symptoms that were associated with the arousal and reactivity subdomain which were found to be statistically significant. Suffering social isolation was a factor found statistically significant with the cognition and mood subdomain.
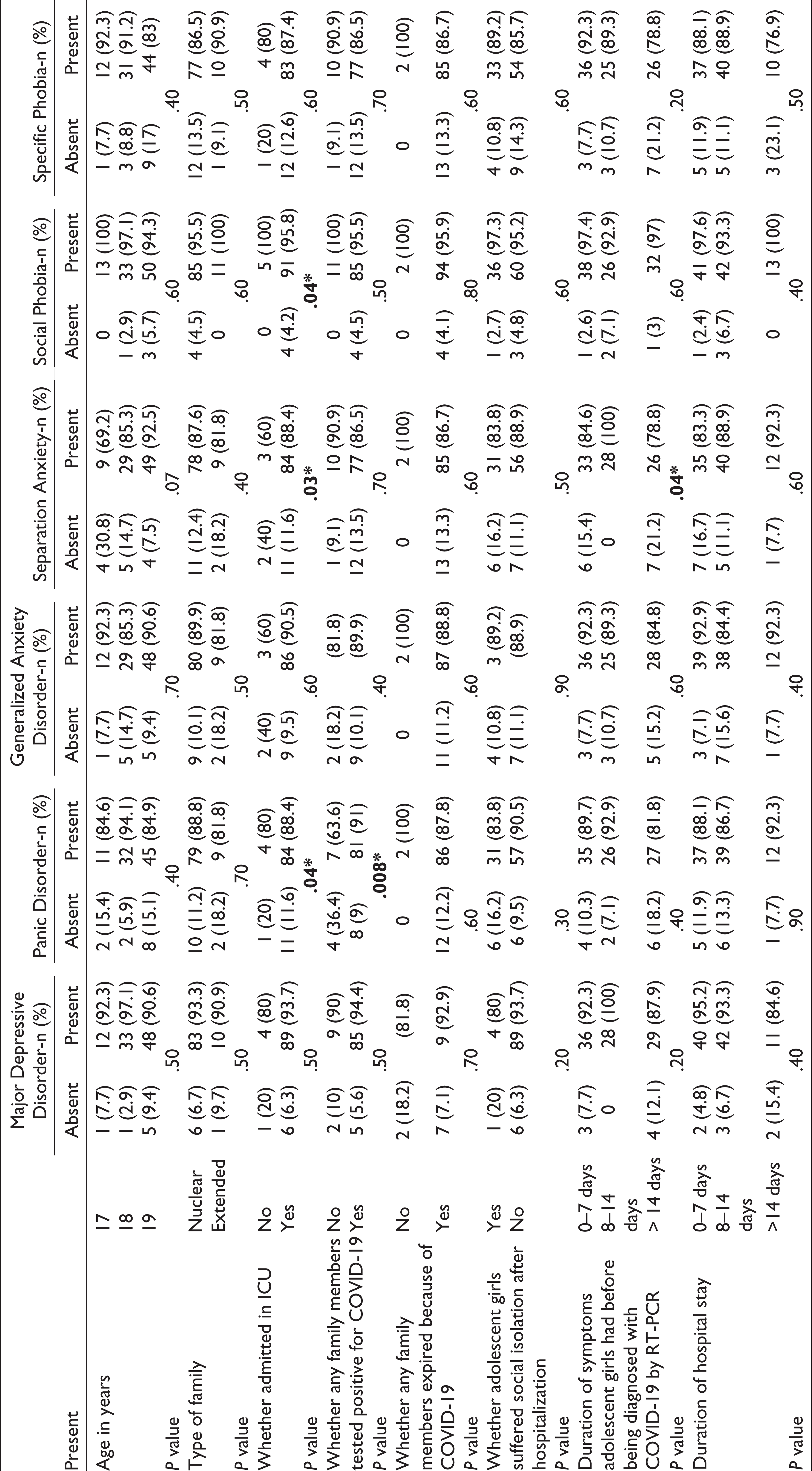
Out of the 100 COVID-19 infected adolescent girls, 7 (7%) had major depressive disorder, 12 (12%) had panic disorder, 13 (13%) had separation anxiety, 4 (4%) had specific phobia, 13 (13%) had social phobia, and 11 (11%) had generalized anxiety.
Factors like admission to ICU and family members being tested positive for COVID-19 were found to be significantly associated with PTSD. Admission to ICU and duration of COVID symptoms were two factors found to be statistically significant with separation anxiety (Table 3).
Association Between Various Psychiatric Manifestations Captured by MINI-KID and Sociodemographic Factors
Discussion
This study being a cross-sectional study carried out for 6 months, showed the prevalence of PTSD among adolescent girls as 15% estimated using 2 different PTSD tools used exclusively in adolescents. Duration of illness and hospital stay were found to have a statistically significant association with PTSD. Girls with throat pain, headache, and diarrhea were symptoms found to have a statistically significant association with PTSD. About 7% had major depressive disorder, 12% had panic disorder, 13% had separation anxiety, 4% had a specific phobia, 13% had social phobia, and 11% had generalized anxiety. Factors like ICU admission and family members being tested positive were found to have a statistically significant association with PTSD. ICU admission was the only factor found to have a statistically significant association with separation anxiety and social phobia among adolescent girls. Duration of illness and ICU admission were factors found to have a statistically significant association with separation anxiety.
As per our literature search, there are no previous studies concerning PTSD among adolescents after contracting COVID-19 infection. The various emerging literature on COVID-19 and PTSD has shown a strong association of PTSD in individuals who had been exposed to COVID-19. According to a study done in China, a significantly higher prevalence of PTSD among participants with suspected or confirmed COVID-19 was found. Those who have had close contact with a person who had COVID-19 had higher odds of having PTSD. 20 A study done in Italy has shown that patients with SARS-CoV-2 had a 31% prevalence of PTSD and females were at higher risk for contracting PTSD post COVID-19 infection. 21 In a study done in China among youth, 14.4% of the sampled youth had PTSD symptoms showing that COVID-19 has an immense effect on youth mental health. 22 A study done by Wang et al in China among nurses who were exposed to COVID-19 has shown a 16.8% prevalence of PTSD. 3 Adolescents who had COVID-19 infection need psychiatry care and 10 % of infected children would experience PTSD as a remote consequence. The prevalence of PTSD in our study is 15% which is similar to these studies. All these studies have established that COVID-19 infection can lead to PTSD. Clearly, there is a dearth of data related to COVID-19 mental health and children affected along with their psychological sequel post COVID-19 infection. This study shows an 11% prevalence of generalized anxiety among participants. A study done in China has clearly established a causal relationship between anxiety in adolescents related to COVID-19 exposure.23, 24A cross-sectional study done in Turkey among health care workers showed the presence of anxiety among those who were exposed to COVID-19. 25 When manifested in children and youth, anxiety disorders are more prevalent but harder to detect of all mental health disorders. 26
This study shows that 7% of COVID-19-infected adolescent girls had depression. Studies done by Guo et al have shown that COVID-19 exposure among adolescents had higher odds of depression. 27 A systematic review showed a higher prevalence of depression among adolescent girls. 28 This study showed that 4% had a specific phobia of COVID-19 infection. COVID-19 infection has instilled fear in children as they are worried not only about getting infected but also having their parents staying at home added with separation from family and friends, seeing or being aware of critically ill members affected with coronavirus, or the passing of loved ones or even thinking of themselves perhaps dying from the virus would have a detrimental effect on the mental health.29–32 It has been shown from various studies that when a child gets exposed to these incidents like pandemics or other natural disasters, it can precipitate the development of various mental health abnormalities like anxiety, panic attacks, depression, mood disorders, and other mental illnesses. Young women getting infected with COVID-19 are at higher risk for developing PTSD.33, 34 Children would have not always gone through a traumatic event just like elders do and any traumatic event can later lead to a stress disorder. 35 Studies have provided evidence for formulating psychological intervention measures to improve young people’s mental health and psychological adaptability during the occurrence of COVID-19, which may be extremely needed for school and college-going adolescents to face any such similar pandemics in the future. 36 Pediatricians must take care of their patients who are adolescents and warn parents of mental health issues like mood swings, irritability, and mild psychosis. 37 Moral injury because of concern of having the loved ones infected or expired because of infection, social isolation post COVID-19 infection, and hospital stay when infected can predispose adolescents to develop PTSD. For children and adolescents, the emotional impact of COVID-19 infection can be the worst experienced or anticipated event. COVID-19 can be a traumatic stressor event that elicits PTSD-like responses and exacerbates other related mental health problems.38, 39 Mental health screening seems to be neglected obviously as controlling the ongoing pandemic and providing the optimal care for COVID-19 patients were still the dominant task in many parts of the world. Targeted mental health services for the prevention of PTSD along with other mental health abnormalities among schoolchildren and adolescents exposed to COVID-19 should be initiated at schools and colleges. Efforts must be made so that children in quarantine can contact their parents guided by daily routine and have access to disease information. Early screening needed intervention, and possible prevention of PTSD among a huge number of COVID-19 survivors needs to be purveyed. As with other mental health conditions, it is important that screening, diagnosis, and treatment for PTSD begins early on before adolescent lose their self-esteem, important relationships, or develop other mental health disorders, including substance misuse.
The strength of the study is that two validated questionnaires were used to diagnose PTSD to avoid overdiagnosis. Various studies on post COVID-19 complications among the elderly have been published but very few on mental health sequels. Up to our best literature search, this could be the first of few studies to see for post COVID-19 mental health sequel among adolescents. The study has a few limitations. The temporal association cannot be established whether mental abnormalities were present before or after infection. A relatively smaller sample size makes the results poor to generalize as it was conducted in only one institution. A multicentric study will be adding more information on the causation of the post COVID-19 mental health sequel. As the pandemic was ongoing with stringent lockdowns, no face-to-face interviews were conducted. Face-to-face interviews would have been more accurate in diagnosing all mental health conditions listed above. CPSS-5-I interview method was used as there was no access to online survey forms for many parents and the majority had no android mobile. Administration of CPSS-SR which is a self-reported questionnaire would have been more appropriate if there was access to android mobiles.
Conclusion
COVID-19 can be a traumatic stressor event among adolescents which can elicit PTSD-like responses and also exacerbate mental health problems. Before people lose their self-esteem, important relationships, or develop other mental health disorders, early screening would prove beneficial and possible prevention of PTSD complications among adolescents. The global incidence of COVID-19 infections has increased as a result of the pandemic, and so will PTSD. The routine use of effective preventive measures and the dissemination of evidence-based psychotherapies should be seen as a priority at schools and colleges. COVID-19 seems to be far from gone until all countries have been vaccinated fully.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.