
Abstract
Background:
Media, including mobile phones, computers, and social media, is a dominant force in the lives of adolescents, and has now penetrated the rural areas. Screen addiction (SA) is a pathological compulsive use of screen-based devices.
Objectives:
To estimate SA and its associated factors among school-going adolescents residing in a rural area in South Karnataka.
Methods:
A cross-sectional study was conducted among adolescents (10-19 years) in 4 schools of Solur Hobli, Ramanagara district, using a structured questionnaire including physical activity, family, and academic stressors. SA was assessed using Tao’s Diagnostic Criteria for Internet Addiction. Depression was screened using Physical Health Questionnaire-9. Chi-square test and logistic regression were done for factors associated with SA.
Results:
Of the 335 adolescents, 20% felt preoccupied with screens, 8% felt restless, moody, and irritable when not using them, 26% used screen devices as a way of escaping problems or relieving irritable mood, 12% had depression, and 3.9% had SA. SA was significantly higher among depressed subjects (adjusted odds ratio [AOR] = 5.18 [1.48-18.13], P = .010), males (AOR = 12.54 [1.46-109.9], P = .021), adolescents who felt that their parents fought frequently (AOR = 4.21 (1.17-15.09), P = 0.027), and adolescents who did not participate in sports (AOR = 3.82 (confidence interval: 1.04-14.06], P = 0.044).
Conclusion:
While proportion of rural students with SA is still low, we need to prevent this from developing into a public health issue by recognizing SA and depression among students and develop targeted interventions to manage the same, including increasing awareness among teachers and students about SA and its link with depression.
Keywords
Introduction
Adolescence is a unique phase between the ages of 10 and 19 years 1 with profound and rapid changes in all domains—physical, cognitive, psychosocial, and emotional—that have an impact on the feelings, thoughts, and decision-making of adolescents, making them vulnerable to substance use, lack of physical activity, and unhealthy lifestyle and behaviors. 2 Media which includes television, mobile phones, and computers, as well as social media, are a dominant force in the lives of adolescents. 3 The term “screen addiction” (SA), also known as “screen dependency disorder” describes pathological compulsive use of screen-based devices. 4 Though gaming addiction is the only screen-based addiction included in DSM-V, it has been documented in medical literature that internet addiction or SA is a behavioural addiction and impulse‐control disorder that shares similarities to substance addictions, including aspects of tolerance, withdrawal, repeated unsuccessful attempts to cut back or quit, and impairment in everyday life functioning.4,5 SA among adolescents has been linked to mental health disorders like depression and anxiety, metabolic disorders like obesity, as well as poor academic performance.6–8
India is home to the largest adolescent population in the world, with two-thirds residing in rural areas. 9 With increasing penetration of mobile phone and internet technology into the Indian rural hinterland, adolescents residing in rural areas now have access beyond the traditional television screen, to smartphone and computer screens. This could set rural adolescents on a trajectory of SA and resultant health consequences, more so in rural areas close to large metropolitan cities, where newer screen options like laptops and tablets are easily accessible. The penalty of not preventing or managing SA in this population would also result in the extension of consequent health issues into adulthood, and limiting the opportunities to lead gratifying lives as adults. 2
A study in Gwalior city among private school students found 24% adolescents to have moderate internet addiction and 6.3% had severe addiction 10 ; however, an extensive review of literature has revealed a complete lack of information regarding SA among rural adolescents and its link with adolescent depression in India. This study was therefore conducted with the aim of estimating the prevalence of SA and its associated factors (including depression) among adolescents residing in a rural area in South Karnataka.
Methodology
Study Setting
This was a cross-sectional study among school-going adolescents in 4 government-run high schools located in villages under Solur PHC area, Ramanagara district, South Karnataka, around 60 kms from Bangalore city, during August to September 2019. The medium of instruction in all the schools was Kannada.
Study Population
Adolescent students aged 10 to 19 years enrolled in the 4 schools.
Sampling
Sample size was calculated based on a previous study in Mangalore city schools, where 30% of adolescents had an internet addiction. 11 With 5% absolute precision and 95% confidence limits, sample size was estimated to be 323. As the total number of students in the sampling frame was nearly the same, universal sampling was employed.
Inclusion Criteria
Students who have completed 10 to 19 years of age.
Exclusion Criteria
Students who were absent on the days of visit by the researchers.
Ethical Considerations
Ethical approval was obtained from the Institutional Ethics Committee along with permissions of the Block Educational Officer and school principals. Written informed consent from the parents and participants aged 18 years and above and written and verbal assent from the students below 18 were obtained prior to enrolment in the study.
Study Tools
The students filled out a pretested, structured, self-administered questionnaire translated into Kannada and back translated by a different translator to identify any ambiguities or errors that could have occurred due to the nuances of the language. Face-validation for content was done by 2 experts in the field of adolescent psychiatry and public health. It included socio-demographic details and risk factors like family and academic stressors, 12 types of screens used, duration of use of each device per day, and number of days used per week, and whether the device was used for academic, social media, recreational, or gaming purpose. SA was assessed using Tao’s Diagnostic Criteria for Internet Addiction, a 7-item questionnaire which has a sensitivity of 99.2%, specificity of 100%, and positive predictive value of 100%. 13 As per Tao’s criteria, the subject was said to have SA if he/she had at least 6 h of daily internet use for the last 3 months along with preoccupation with screens (thinks about previous screen activity or anticipates next session) and withdrawal (manifested by dysphoric mood, anxiety, irritability, and boredom without screen activity), plus any 1 of the following: tolerance (increase in screen use to achieve satisfaction, desire, and/or unsuccessful attempts to reduce or discontinue screen use), continued excessive use of screen devices despite having a persistent problem likely to have been caused or exacerbated by screen use (like pain in the wrists or at the back of the neck while using screen devices), loss of interests, previous hobbies, and entertainment with the exception of internet use or the use of screen devices to escape or relieve feelings of helplessness, guilt, and anxiety. The Kannada version of the Patient Health Questionnaire-9 (PHQ-9) was used to screen for depression. The questions are scored on a Likert scale ranging from Not at all-0, to nearly every day-3, with a maximum total score of 27. A score of <5 indicates no depression, 5–9: mild depression, 10–14: moderate depression, 15–19 moderately severe depression, and ≥20 indicates severe depression. PHQ-9 screens for depression among adolescents with a sensitivity of 90% and a specificity of 86%. 14 Students who screened for depression and /or SA were referred to the secondary-level hospital nearby for further evaluation and management. At the end of the study, all the students in each of the 4 schools attended an interactive health education program on depression and SA.
Operational Definitions
SA: based on Tao’s Diagnostic Criteria for Internet Addiction. 13 Screen-based devices: smartphone, tablet, television, gaming consoles, computers, and laptop. 15 Early adolescence: 10–14 years, late adolescence: 15–19 years. 16
Statistical Analysis
The data was analyzed using IBM Statistical Package for Social Sciences version 20. The data was described using frequencies, proportions, mean, standard deviation, median, and inter-quartile range. Bivariate analysis was performed with chi-square test to associate SA with various independent covariates. Multiple logistic regression analysis was performed and adjusted odds ratios with 95% confidence intervals (CIs) were obtained. P value of <.05 was considered statistically significant for all analyses.
Results
A total of 335 adolescents participated in the study. The mean age of the study population was 13.99 ± 1.15 years. There were more of young adolescents in our study (66.5%) and slightly higher proportion of males (54.9%). Majority (51.6%) belonged to lower or lower middle class. Majority of the study participants belonged to the nuclear families (71.3%). On screening with PHQ-9, it was found that 40 (11.9%) of the adolescents had probable depression.
The study found that 306 (91.3%) of the rural adolescents were using some form of screen, most commonly used form of screens were smartphones (63.0%), television (48.4%), and laptop (12.5%). None of the adolescents were using tablets/iPads.
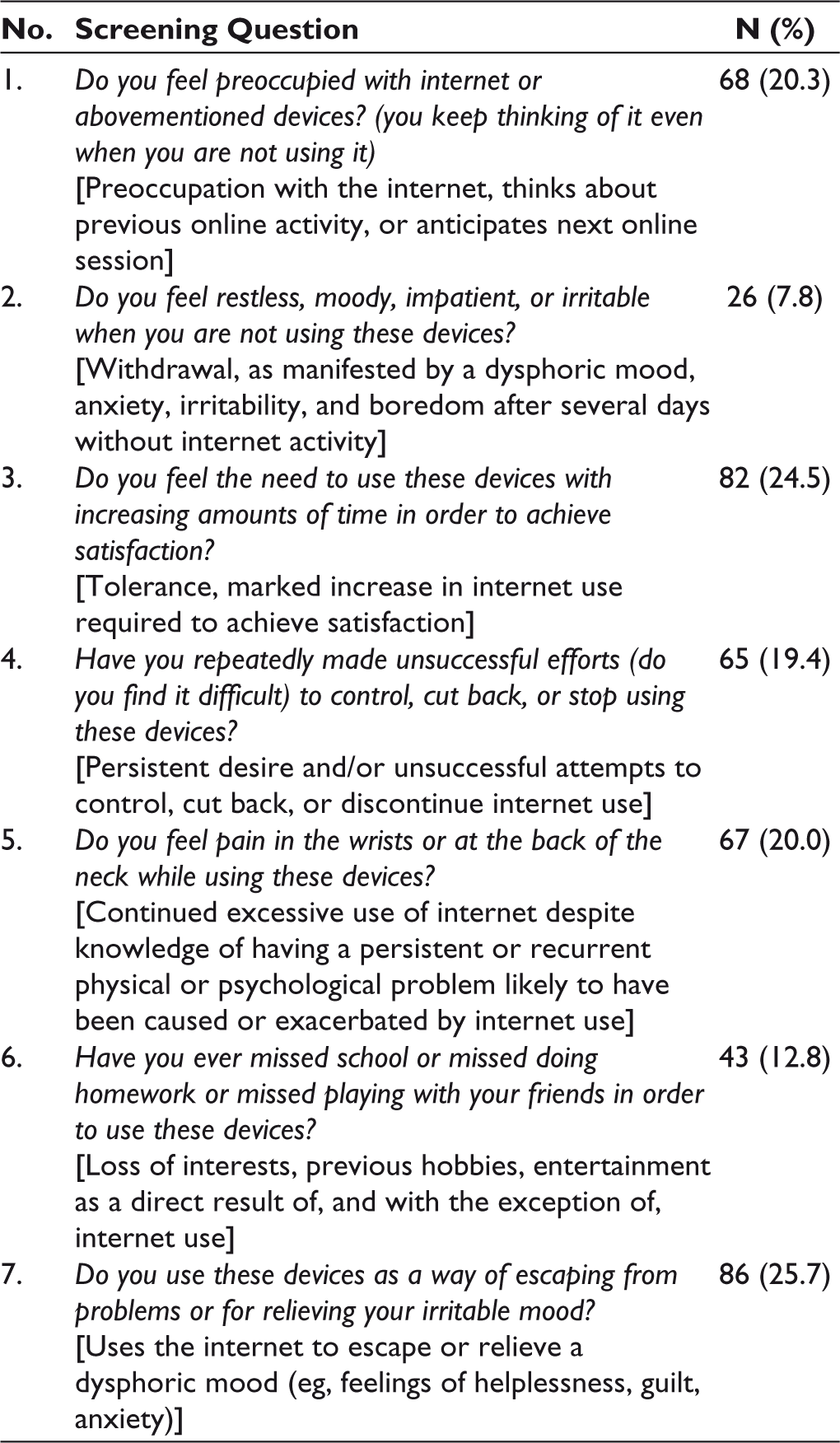
We found that 13 (3.9%) of the study participants had SA. The following SA behaviors were elicited in the study: 20% of the participants reported that they felt preoccupied with screened devices and 8% reported that they felt restless, moody, impatient, or irritable when they were not using the devices. It was found that 26% of the participants reported that they used the devices as a way of escaping from problems or for relieving their irritable mood, 25% reported that they felt the need to use these devices with increasing amounts of time in order to achieve satisfaction, and 19% felt that they had repeatedly made unsuccessful efforts to control, cut back, or stop using the devices. It was found that 20% of the participants reported pain in the wrists or at the back of the neck while using the devices and 13% had missed school or missed doing homework or missed playing with their friends in order to use the devices (Table 1).
Screening of Subjects Using Tao’s Criteria for Screen Addiction
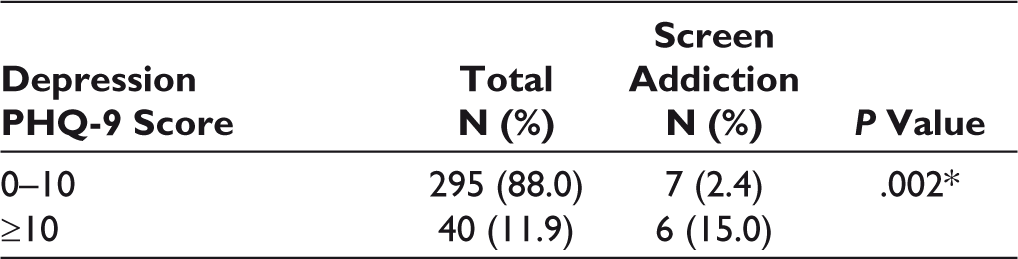
SA was found to be significantly associated with male adolescents (P = .006), those who felt that their parents fought frequently (P = .048), nonparticipation in sports (P = .024), and those who used screens for the purpose of gaming (P = .035). SA was also significantly associated with depression (P = .002) (Tables 2–6).
Association of Screen Addiction With Various Sociodemographic Factors (n = 335)
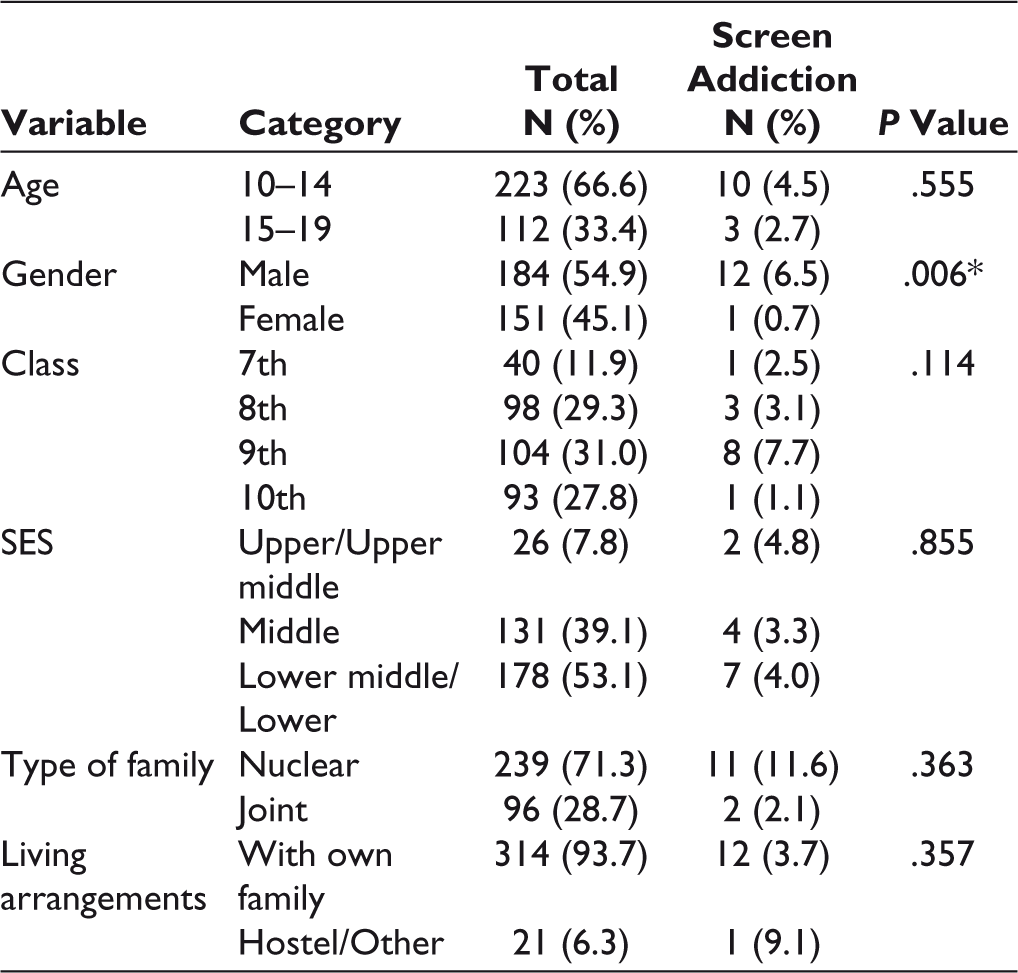
*Statistically significant at P < .05.
Association of Screen Addiction With Family Factors (n = 335)
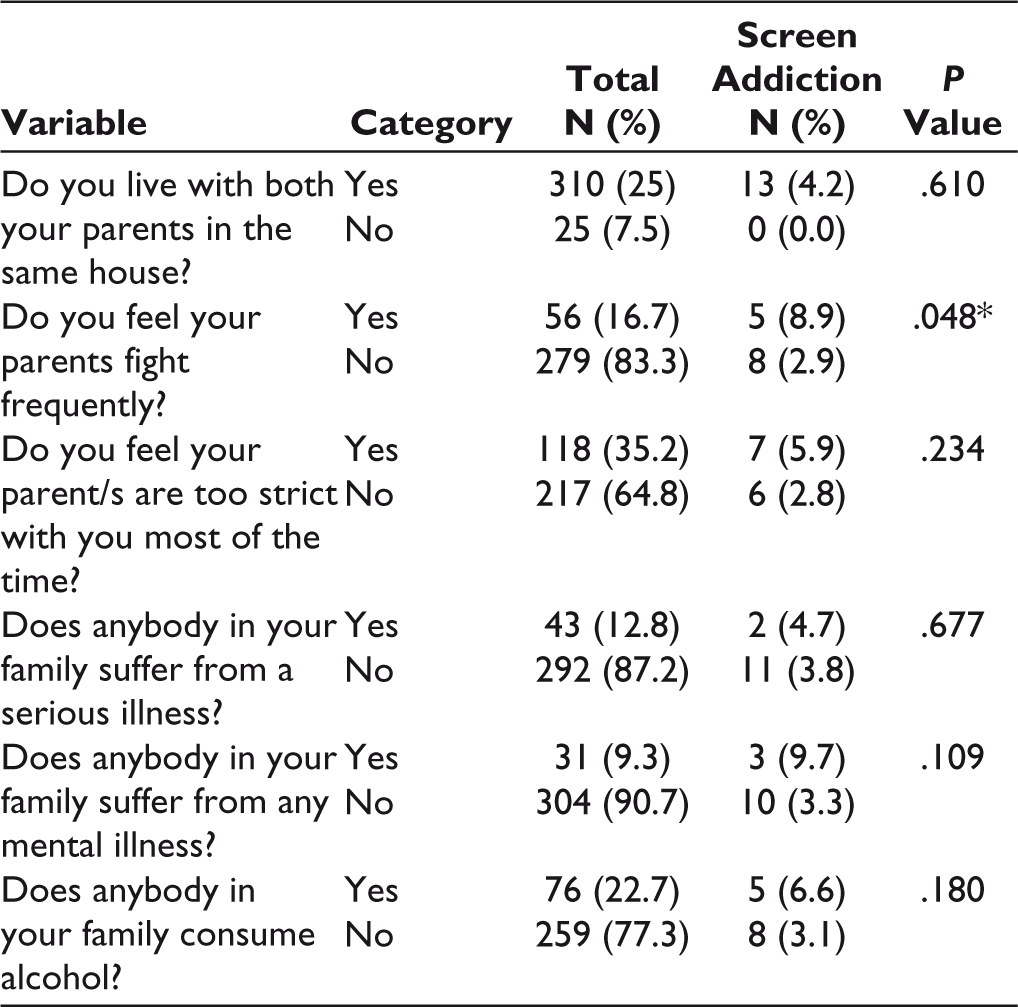
*Statistically significant at P < .05.
Association of Screen Addiction With Academic Factors (n = 335)
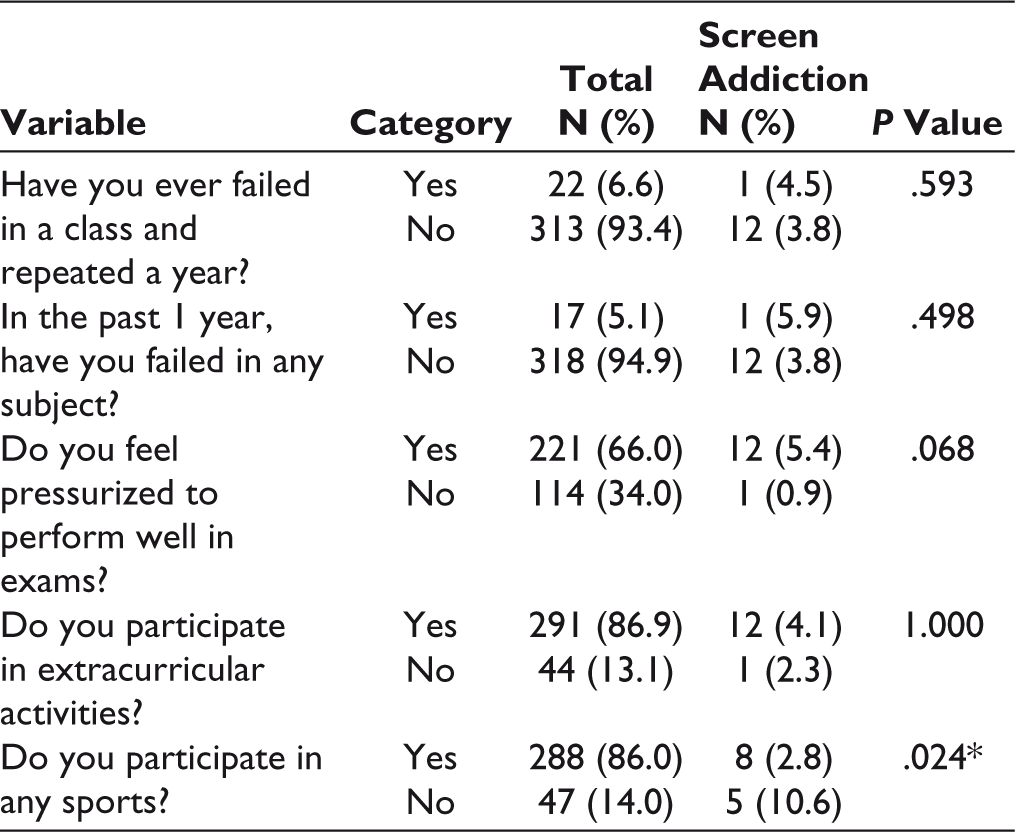
*Statistically significant at P < .05.
Association of Screen Addiction With Type of Screen and Screen Time (n = 335)
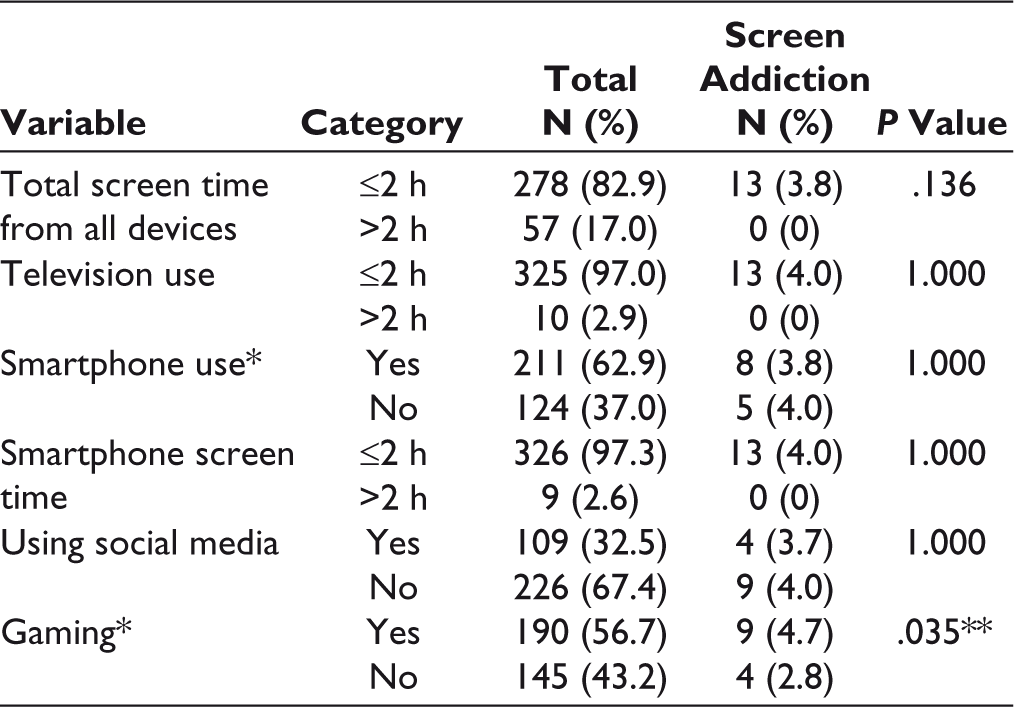
*These are not mutually exclusive categories. Subjects reported using smartphones for browsing internet, using social media, and gaming. Gaming was performed on smartphone, smart TV, and gaming console.
** Statistically significant at P < .05.
Association of Screen Addiction With Depression (n = 335)
Multiple Logistic Regression With Significantly Associated Factors
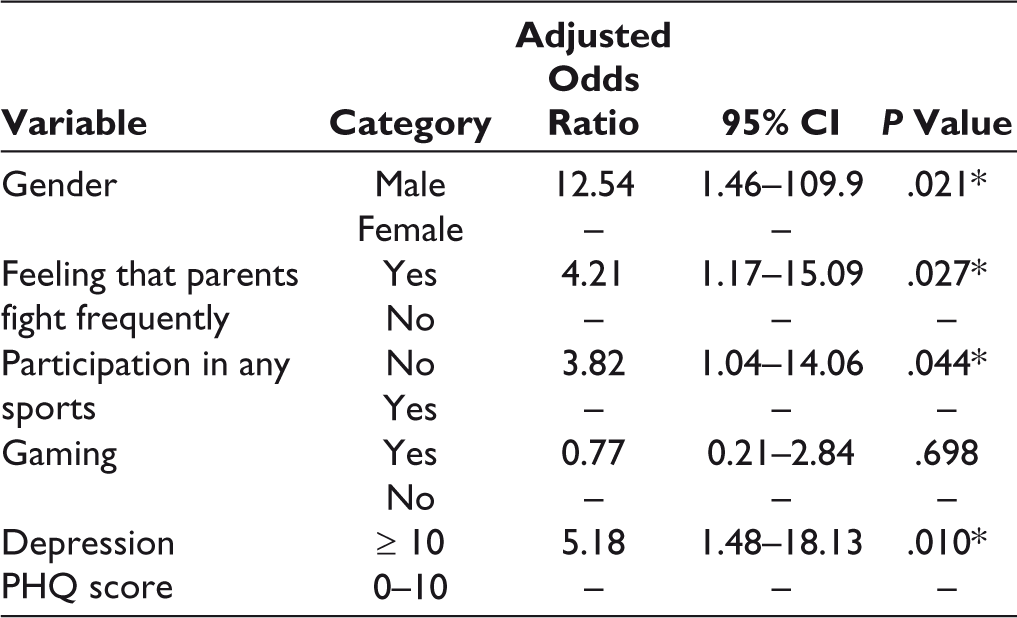
After regression analysis, the variables that retained a significant association with SA were male gender (adjusted odds ratio [AOR] = 12.54, CI [1.46–109.9], P = .021), parents fighting frequently (AOR = 4.2, CI [1.17–15.00], P = .027), not participating in sports (AOR = 3.82, CI [1.04–14.06], P = .044), and having probable depression (AOR = 5.18, CI [1.48–18.13], P = .010) (Table 7).
Discussion
For the first time, India has more internet users in rural areas (227 million) than urban areas (205 million). 17 This study was therefore done to estimate the prevalence of SA and its associated factors including depression among rural school-going adolescents.
It was found that 3.9% of the study participants were found to have SA. A striking contrast was seen in a study among rural school students in Haryana where 30.3% had SA. 18 However, the screening tool used in the Haryana study was a self-designed nonvalidated tool which included questions on keeping the phone switched on while resting and returning missed calls. This could have results in overestimation of SA as these behaviors are not considered as addictive behaviors in all the currently validated SA screening tools. Our study results are similar to an Italian cross-sectional study that found a prevalence of 6.3% mobile phone addiction among adolescents. 19
While exploring screen addictive behaviors, we found some similarities with the Haryana study, where it was found that the proportion of adolescents who felt preoccupied with screen-based devices was 20%, while it was 17% in our study. We found that 26% felt they needed to use the device for an increased amount of time to achieve the same satisfaction and 13% admitted to skipping classes to use screens, these proportions were the same as in the Haryana study. 18
Males in this study were 12 times more likely to have SA as compared to females in this study. This finding was similar to the Haryana study. 18 The probable reason could be that adolescent boys usually play more computer and mobile phone games as compared to adolescent girls and in traditional settings, girls are often more occupied with household chores as compared to boys. Also in rural areas, the number of screen-based gadgets are fewer in the home, and in a patriarchal society, boys are given preference over the girls when it comes to sharing limited resources.
We found that adolescents who reported that their parents fight frequently were 4 times more likely to be addicted to screens than those who did not report so. Family conflict has been identified as a risk factor for SA in a systematic review by Sahu et al. 20 This could be explained by the fact that adolescents who experience parental discord may use screens to distract themselves from the conflicts at home and this becomes a mode of escape from unpleasant reality.
Adolescents who did not participate in sports were 3 times more likely to have SA than the ones who did participate in sports activities. A study in Korea found that participation in sports reduced internet addiction among 13- to 15-year-old students. The mediator variable identified was self-control. Participation in sports was found to improve self-control which in turn reduces screen time and SA. 21 This finding has public health importance as physical activity and sports can easily be incorporated into the daily schedule of students at school, not only to improve physical health but also the mental health of adolescents.
Our study found that adolescents with probable depression were 5 times more likely to be addicted to screens than those without depression. This finding resonates with that found in studies in USA, 22 Sweden, 23 Lebanon, 24 Turkey, 25 and Korea. 26 Possible explanations for this link are sleep deprivation and social isolation, leading to cognitive and behavioural problems which can further lead to poor academic performance, lack of self-esteem, and depression.
Our study points to the need for reaching out to teachers, parents, and students to educate them regarding the dangers of SA. One in every 10 students in our study had probable depression and this indicates a need for school-going adolescents to be screened for depression along with appropriate referral pathways. Students need to be encouraged to participate in sports and for schools to take concrete measures to ensure that daily sports is included in the school routine. Counselling services for students may be made available at schools by partnering with NGOs. Rashtriya Bal Swasthya Karyakram (RBSK) strengthens school health in rural areas through identification and intervention for children up to 18 years, for disease, deficiencies, defects, and delays. 27 Screening for depression and SA with appropriate referrals may be included under the purview of RBSK.
Our study was conducted a few months before the COVID-19 pandemic struck. Since then, screen time has increased for adolescents due to online learning and increased use of screens for entertainment during the lockdown periods. The problem of SA can only get worse given this situation. There is scope for further research into how the COVID-19 pandemic has affected SA among rural-dwelling adolescents.
Limitations
The study was based on a self-reported questionnaire. This may have led to recall and social desirability bias, which may have led to under-estimation of SA. We have used the term screens and internet interchangeably, as many of the televisions nowadays have “smart screens” and it is difficult to verify whether the subject was watching a television program or online videos (eg, YouTube), and whether the subject was playing online games or using a gaming console with the television. The exact duration of internet- and non-internet-based screen use was therefore difficult to assess.
Conclusion
Our study found that most rural adolescents use screen devices and 3.9% of them had SA which was significantly associated with male gender, parental conflict, nonparticipation in sports, and depression. Screen devices have well penetrated the rural community and SA has to be addressed before it becomes a public health problem. School-going adolescents need to be screened for depression, should be offered counselling services, and need to be encouraged to participate in daily sports at school.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.