
Abstract
Background:
Resilience among adolescents can best be understood by examining the risk and protective factors in the lives of at-risk adolescents. A standardized tool to identify adolescent psychosocial risk and protective factors may help better understand the strengths, vulnerabilities, and the potential for resilience among adolescents. Hence, the present study aims to identify and measure the risk and protective factors in the lives of adolescents.
Methods:
A sequential exploratory mixed-methods design was used to develop a tool that measures risk and protective factors among adolescents. The qualitative study explored psychosocial risk and protective factors among high-risk adolescents using 4 major domains: individual, family, school, and community. To develop the tool, prisoners (N = 12), caregivers of the prisoners’ children (N = 12), teachers of the prisoners’ children (N = 12), and prison authorities (N = 12) were interviewed about their experiences with prisoners’ children. The interview data were analyzed, and items reflecting the risk and protective factors in the lives of the adolescent children of incarcerated parents were generated. The item pool consisting of 239 items was administered to a sample of 312 rural adolescent students. To validate the risk factors scale and protective factors scale, self-report scales measuring behavior problems, adjustment, well-being, and positivity were used.
Results:
The new tool developed to measure the risk and protective factors for adolescent psychosocial development was found to have adequate test-retest reliability, content validity, convergent validity, and divergent validity.
Conclusion:
In this study, a scale to identify psychosocial risk and protective factors was developed and standardized. The tool will be helpful to psychologists and counselors working with adolescents to understand the risks and protective factors present in their lives and design interventions to nurture resilience in them.
Introduction
The resistance to the aftermath of trauma is understood across contexts. The mechanisms to cope with, or resist, the potential precursors to trauma such as exposure to violence, parental substance abuse, migration, sexual abuse and exploitation, institutional abuse, and other specific risks require attention and understanding in a wide range of contexts. 1 The interaction and utilization of available resources in social–ecological systems such as microsystem, mesosystem, exosystem, and macrosystem will account for the individual’s ability to cope during adverse conditions. 2 The capacity to navigate to resources that facilitate positive development under stress or adverse experiences and negotiate with those resources in culturally meaningful ways is termed resilience. 3 Psychological resilience is operated by the multiple interactions of factors within the ecological systems such as individual, family, school, and community systems. 4 Understanding the processes of resilience based on social ecology (eg, temperament, attachment, self-regulation, compassion, care and cohesion from family and extended family, and support from school and various institutions in the community) can help us appreciate how posttraumatic growth and recovery are possible by the individuals’ capacity to navigate toward resources and effectively utilize them for adaptation.1, 5–7 When a child experiences neglect, the experience might not necessarily be vulnerable to abuse; instead, they can express helping behavior and creativity to make others feel secure. 8 The outcomes are shaped by environmental resources for adaptation during the developmental stages.3, 9, 10 The relevance of resilience among high-risk populations is based on population risk exposure, or factors and processes that moderate and mediate the impact of risk exposure or outcomes relevant to the population. 11 It is evident that the more resources individuals access, the better are their chances of adjustment to risk exposure.12, 13
At-Risk Adolescents
Adolescence is when individuals become vulnerable to rapid physiological and social transformation effects. 14 There is consistent interaction between the individual and environment resources during the developmental processes. 15 Adolescents are at a high risk of experiencing psychological problems and psychiatric disorders. 16 Adolescents are likely to be engaged in substance abuse, violence, and other risky behaviors because of difficulties in making positive adaptations to changes during developmental transition. 17 Several sociodemographic factors influence the developmental process from adolescents to adulthood. Significant risky behaviors and physical and mental health conditions are prevalent among rural adolescents.18–20 Further, worsened socioeconomic conditions result in school dropout. 21
Besides this, adverse childhood experiences also influence the developmental process. Adverse childhood experiences include neglect, 22 parental loss,22–24 traumatic events, 25 physical and mental abuse, 26 parental separation, 27 and the like. In the background of such adverse conditions during childhood, the ongoing interaction of risk and protective mechanisms results in either vulnerabilities or resilience among individuals during adulthood.28–31 Active interactions of risk and protective mechanisms influence individuals’ interpretation of the cause, shaping their expectations, attitude formations, and experiences. 32 These experiences are reflected as negative or positive behavioral outcomes at various socioecological levels 1 during the development of an individual.
Risk Factors and Adaptation
Risk factors increase the vulnerability and challenge the healthy psychosocial development of an individual.33, 34 The impact of risk is either determined by the quality and quantity of risk or the perception of risk by the individual. 11 However, risks are influenced at one level or multiple levels. Certain disadvantages in demographic and socioeconomic factors in adolescents’ life predicts socially unacceptable behavioral outcome little later.33, 35, 36 Children experience anxiety disorders, depression, and lower self-regulation skills when they witness parental incarceration. 37 Children witnessing violence and those experiencing child abuse at home develop internalizing and externalizing problems.38, 39 At school, children may face challenges because of disadvantaged demographic conditions like poor school environment, 40 physical appearances, 41 and low grades. 42 Conditions related to intellectual problems at schools lead to experiences of psychological problems. 43 Simultaneously, less support from peers usually leads to anxiety in the children. 44 At the community level, when the children live in impoverished neighborhoods, they may feel the neighborhood unsafe, 45 where access to peers and adults who can aid in their career growth becomes impossible.46, 47
Protective Factors and Adaptation
Protective factors are those factors that enhance healthy psychosocial development. These factors mitigate the adverse effects of risk factors and reduce behavior problems.33, 34, 48 The influence of protective factors at one or multiple levels can benefit healthy development. 49 Adolescent Americans receive instrumental support and peer support during adversities. 50 Similarly, adolescence experiencing good interpersonal relationships reduce depression and enhances resilience. 51 At home, family plays a critical role in promoting psychological well-being. 52 Support from parents is the strongest predictor of healthy psychosocial development where self-esteem and adjustment are developed.44, 53, 54 Support at school and in the neighborhood also predicts psychological well-being.44, 53–56
To understand the agencies and pathways to resilience among adolescents from at-risk backgrounds, developing tools to measure risk and protective factors is particularly important. Many scales have been developed for measuring risk factors18, 57 and protective factors like resilience,58, 59 attachment, 60 strength and difficulties, 61 and well-being.62, 63 The scales focus on self-reports by adolescents 59 and other external factors contributing to protective factors.64, 65 For instance, risk survey focused mainly on demographic variables challenging psychosocial development. 18 The available scales have a specific focus rather than a comprehensive global perspective that includes both internal and external risk and protective factors. Examining risk and protective factors among at-risk adolescent populations from a socioecological perspective needs special focus and stands as the rationale for developing this new scale.
Need for the Study
Multiple empirical types of research on social support, psychological well-being, resilience, emotional regulation, depression, internalizing problems, externalizing problems, etc, elaborate on the processes of the healthy psychosocial development of the adolescent population. These factors could also be measured using standardized scales. Nevertheless, arguments and psychological assessments on the psychosocial health of adolescents and at-risk adolescents in the context of current life experiences and situations are limited. 56 An instrument on protective factors for resilience assesses only a few protective factors from personal resources, family, and peer. 66 Instruments like strength and difficulties questionnaire do not measure factors in a holistic approach or socioecological framework to understand positive adaptation in adolescents. 61 Therefore, a tool that assesses the psychosocial risk and psychosocial protective factors in adolescents can provide a better understanding of the lives of adolescents. The need for the present study stems from the lack of a tool that provides a global assessment of psychosocial risk and protective factors covering different levels of the social-ecological model. Hence, the present study was carried out to identify and develop a scale assessing psychosocial risk and protective factors of adolescents.
Method
The present study adopted an exploratory sequential design—instrument development model variant 67 to evaluate psychosocial risk and protective factors of adolescent psychosocial development and identify the underlying variables. The steps started with qualitative data, then built on the quantitative phase according to the design. The first step consisted of qualitative interview and analysis; the second step was establishing psychometric properties of adolescent psychosocial risk and protective factors scale.
Step 1 Qualitative Interview and Analysis
The qualitative method, the first step of tool development, aims to gain a holistic understanding of an individual in his/her natural environment68, 69 using the data collected. Data were collected through the semi-structured interview with prisoners (N = 12), caregivers of prisoners’ children (N = 12), teachers of prisoners’ children (N = 12), and prison authorities (N = 12). The interviewing prisoners, caregivers of prisoners’ children, teachers of prisoners’ children, and prison authorities will provide insight into the life of prisoners’ children who are at-risk adolescents. The interview data were analyzed using thematic analysis, which involved coding the interview responses and generating subthemes and major themes. Thematic analysis helps the researcher to understand the deeper similarities and differences of the participants’ perspectives. 70
Participants
The participants of the study included incarcerated parents (N = 12), caregivers (N = 12), teachers of children of incarcerated parents (N = 12), and prison authorities (N = 12). All the participants were recruited using the snowball sampling technique based on their availability and consent to participate in the study. The parents who were imprisoned because of accusations of criminal offenses like murder (83.3%) and rape (16.7%) participated in the study. The biological fathers of adolescents whose age ranges from 12 to 16 years were imprisoned for 18 months to 9 years (M = 4.63 years; SD = 2.66). The interview duration with the parents ranged from 15 min to 30 min (M = 22.33 min; SD = 5.12). The caregivers of prisoners’ children in the age group 12 to 16 years include mother (75%), aunt (16.7%), and grandparents (8.3%). The caregivers above the age of 25 were recruited. They took care of the children of incarcerated parents for 3 years to 11 years (M = 7.58 years; SD = 2.35) from the imprisonment of the biological parent. The caregivers reside with the adolescents and interact with them for a minimum of 3 days a week. The interview duration with the caregivers ranged from 20 min to 45 min (M = 31.45 min; SD = 6.20). The teachers taught mathematics (16.6%), social science (25%), science (16.6%), language (33.3%), and physical training (8.3%) to adolescent children of incarcerated parents in the age group of 12 to 16 years. The experience of teaching children of incarcerated parents ranged from 1 year 6 months to 5 years (M = 3 years; SD = 1.34). The duration of interview ranged from 20 min to 40 min (M = 30.67 min; SD = 7.86). The prison authorities were the superintendent (8.3%), probationary officers (33.3%), welfare officers (8.3%), social caseworkers (8.3%), assistant jailor (8.3%), and wardens (33.3%), who work for Tamil Nadu Prison. They have experience interacting, understanding, and dealing with the overall family welfare of adolescent children of incarcerated parents, whose ages range from 12 to 16 years, for about 3 to 35 years (M = 11.08; SD = 7.33). The duration of interview ranged from 15 min to 40 min (M = 25.33 min; SD = 7.60).
Ethical Consideration
Participants were explained clearly the objective, importance, and procedure of the research. They were also informed that no foreseeable factors might cause discomfort when they participate in this research. Before collecting data, the oral consent to participate in the study was obtained from parents, caregivers, teachers, and prison authorities. They were also explained about the right to decline, right to withdraw, privacy, confidentiality, disclosures, maintenance of scientific work, and other ethical principles while receiving oral consent. The permission to research children of incarcerated parents was obtained from the Additional Director General of Police, Prison Department, of Tamil Nadu State. Further, permission to interview prisoners, caregivers, and prison authorities was obtained from Prison Department. Permission for collecting data from schools was obtained from the Chief Educational Officer of schools under the administrative jurisdiction of City Corporation and the Principals of selected schools based on the availability of prisoners’ children.
Procedure
One-to-one, face-to-face, semi-structured interviews were conducted with different samples, including parents, caregivers, and prison authorities at prison premises. Interviews were conducted with teachers at the premises of selected schools. The semi-structured interview questions were majorly open-ended. Close-ended questions were raised by the interviewer only when the interviewer felt minimal clarity of information. The interview focused on various areas of the lives of the children of incarcerated parents, namely, individual factors, family relationships, school activities, and relationships with extended family and neighbors. The interview also focused on participants’ perception of the risk and protective factors in the lives of the children of incarcerated parents. The interview intended to bring out the risk and protective factors in the lives of these children of incarcerated parents through the reflections of the members of environmental resources which influence the overall development of these children. The interviews were also aimed at understanding the pathways to psychological resilience among high-risk adolescents. Interviews were audio-recorded, and notes were taken to analyze and understand the risk and protective factors in the lives of children of incarcerated parents.
Analysis
All the interviews were conducted in the Tamil language. The oral consent to participate in the research and audio-record the interviews were obtained from teachers and caregivers prior to the interviews. Interview notes were taken from the interviews with prisoners and prison authorities. The audio-recorded interviews were transcribed, which were then translated into the English language. The translated transcripts and the interview notes were analyzed using thematic analysis, which provides flexible and potentially rich and detailed data.
70
In order to analyze data, the context of participants’ reported experiences and perceptions related to children’s psychosocial development in the background of the study objectives were used. The data were then explored interpretively to look out for underlying contradictions and meanings that would lead to the reflecting experiences of the participants.
71
The transcribed and translated data were extracted to code and build unifying themes manually. The coded data were built into sub-themes, further congregated under sets of major themes. For further analysis, all the responses were classified into 2 categories under 4 different domains, within a framework, for better interpretation. The framework method
72
was used to compare qualitative data and analyze the contrast across many cases, retaining the connections with other aspects of each individual’s experiences. The 2 broad categories, risk factors and protective factors, were named C1 and C2. The domains were internal domain (D1), family domain (D2), school domain (D3), and community domain (D4). The codes and responses under a category were further grouped under any one of the domains for better interpretation. For example, a participant says,
My son does not get good attention from his father because my son’s father talks with him very rarely. His father hardly wants to know about the child. As far as I remember, son and father have spoken only twice after father’s imprisonment (#CG3, Sangeetha, 44 years).
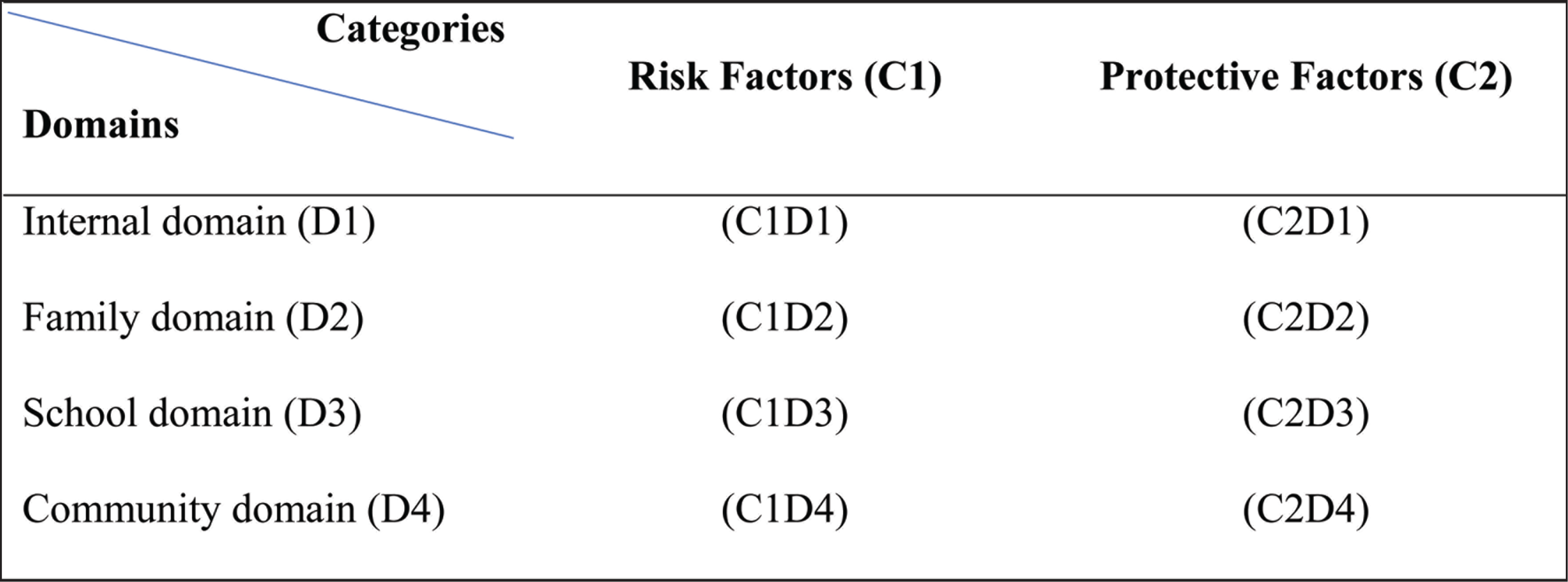
This response could be categorized under risk factors. Further, the same response could be put under the family domain (C1D2). This classification was done because of the child’s prevalent risk condition from a family member. The data were analyzed and categorized in a matrix form to this degree. The following is a matrix representing the classification of the categories and domains based on the data. With reference to the matrix, items for tool development were generated using the interview data.
Item Generation
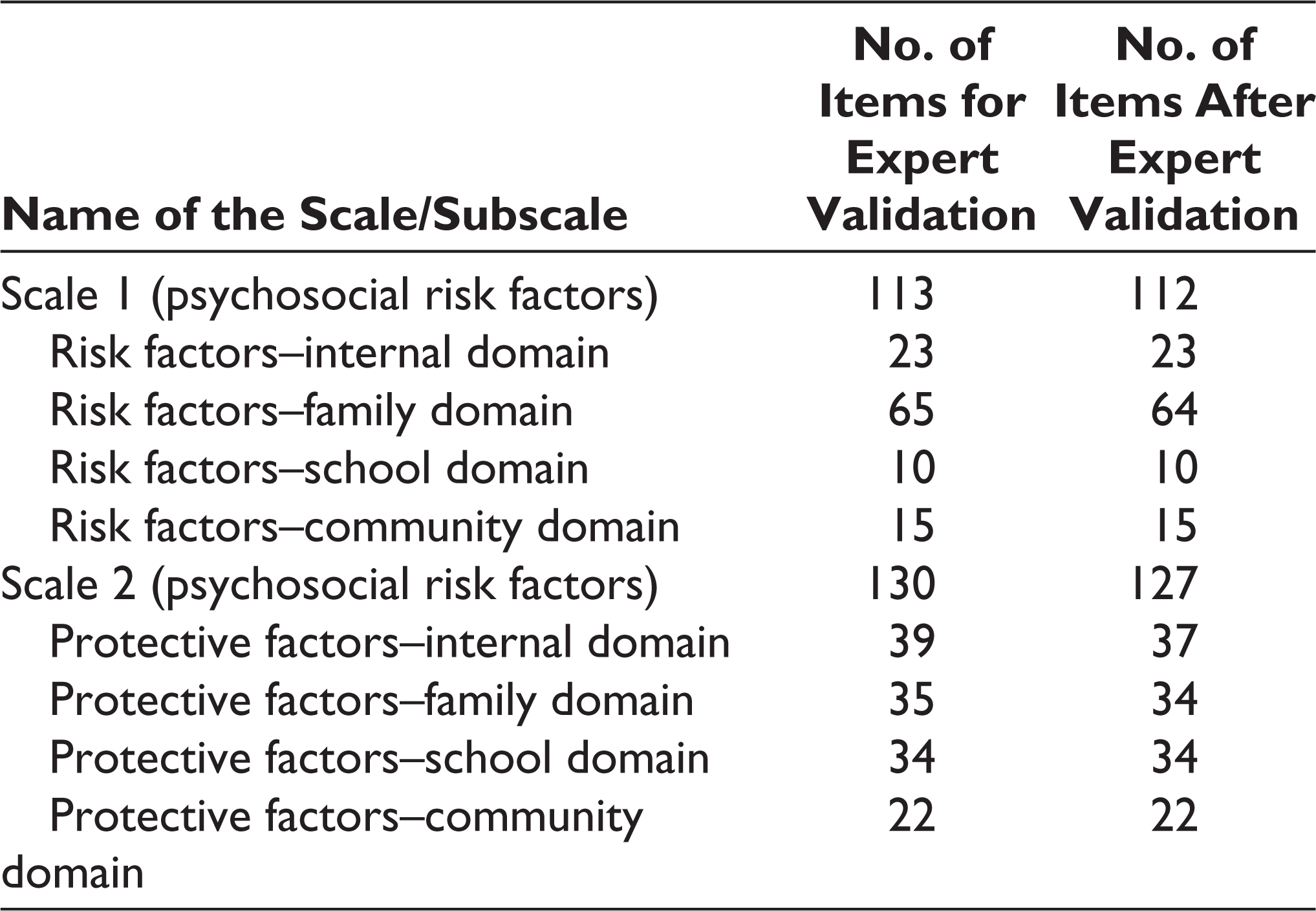
The codes of the thematic analysis from the interview were used to generate items for the tool development. All the items generated are close-ended. The researchers carefully generated items by checking clarity, representation, and relevance for the present study objective. Items were derived from the interview codes consisting of 4 domains: internal, family, school, and community. The segregation of items based on the matrix was essential to understand a broad perspective of the psychosocial development of the adolescent population. Hence, the items were generated based on 2 categories: psychosocial risk factors (n = 113) scale and psychosocial protective factors (n = 130) scale with reference to the matrix. The response for each item was determined to be a 5-point Likert scale ranging from “strongly agree” to “strongly disagree.” The generated items were then given to subject experts for validation.
Validation by Experts
The experts in the panel to validate the items generated for the scale were academics working in adolescent health and well-being. They were requested to validate the appropria-teness of the items generated according to the psychosocial health of the adolescent population. The experts were asked to evaluate the appropriateness and accept items for the psychosocial risk factors scale that measure psychosocial risk factors. The experts were also requested to evaluate the appropriateness and accept items for the psychosocial protective factors scale measuring psychosocial protective factors. Both the scales were to be evaluated for the appropriateness and relevance to one of the 4 domains: internal, family, school, and community domain. The experts, thus, evaluated the psychosocial risk factors scale with 113 items and the psychosocial protective factors scale with 127 items. The results on appropriateness in terms of representativeness of item pool, item clarity, instructions clarity, and linguistics aspects of the items 73 were received from 4 subject experts. On the psychosocial risk factors scale, 1 item and on the psychosocial protective factors scale, 3 items were deleted based on the recommendation by experts, and other items were retained (Table 1).
Showing the Number of Retained Items for Psychometric Analysis
Step 2 Quantitative Data Collection and Analysis
The second step of the study involves a quantitative method to understand various risk and protective factors influencing the psychosocial health of adolescents and also to understand the relationship between variables and the direction of their constructs. 74 The data were collected by administering the newly developed tool to the rural adolescents. These adolescent children reside in the rural parts of the mid-sized city located in the southern part of India.
These adolescent students studying in government schools and hailing from low socioeconomic backgrounds are at-risk for healthy psychosocial development.18, 19 The children living in the rural areas reported mental health problems, lower intellectual attainment, physical problems, and academic problems,18, 19, 75–77 and hence might be considered at-risk for healthy psychosocial development.
Participants
The participants were 312 adolescent students studying in a rural Government school in a mid-sized city in Tamil Nadu state. The age of the participants ranged from 12 years to 16 years (M = 13.63; SD = 0.90). They were students studying sixth, seventh, and eighth grade in a government-run school. The participants did not have a history of psychological illness and consented to participate in the study.
Procedure
Permission was sought from the Principal of a government-run school to collect data from the participants. The school is situated in a mid-sized city located in the southern part of India. Based on the selection criteria, 312 adolescents participated in the study who met the selection criteria for participating in the study. Teachers’/tutors’ judgment was taken to screen-out students who had borderline IQ. All the participants live in rural areas of the mid-sized city who are at-risk to healthy psychosocial development. The data were collected using a set of self-report measures that included the tool newly developed to measure psychosocial risk and protective factors, and other standardized tools measuring well-being, internalizing problems, externalizing problems, adjustment, and positivity from the children who gave written informed consent to participate in the study. Informed consent from the parents of the participants were also obtained. The participants were explained about right to decline, right to withdraw, privacy, confidentiality, disclosures, maintenance of scientific work and other relevant ethical principles before collecting data. The measures were translated into Tamil language for easy understanding of the participants. The collected data were analyzed with the help of appropriate statistical techniques like exploratory factor analysis, linear correlational and average variance extracted analyses, in order to examine the psychometric properties of the tool developed herein. A brief description of the self-report measures used in the study to validate the newly developed tool is given further.
Adolescent Psychosocial Risk and Protective Factors Tool
The tool consists of 2 major subscales, psychosocial risk factors and protective factors. The 112 items risk factors scale measures risk factors that challenge psychosocial development (eg, “I do not like to share my feelings with others”), and the 127 items protective factors scale measures protective factors enhancing psychosocial health (eg, “I care about others most of the time”) among adolescents. The psychosocial risk factor scale consists of 4 domains: disengagement, insecure attachment with parents, maternal distress, and neglect. The psychosocial protective factors scale consists of 7 domains: prosocial behavior, maternal responsiveness, paternal responsiveness, support from teachers, support from peers, support from the community, and emotional support from extended family. The participants responded to statements on a 5-point Likert scale from 5 (strongly agree) to 1 (strongly disagree). A high score on the psychosocial risk factors scale indicates the relevance of adolescents in high-risk conditions. A higher score on each domain indicates a higher level of risk factor assessed by that particular domain. Similarly, the high score on the psychosocial protective factors scale indicates the relevance of adolescents in protective or safe conditions. A higher score on each domain indicates a higher level of protective factor assessed by that particular domain. After factor analysis, 20 items and 28 items in the risk scale and protective factor scales, respectively constituted for further validation of the scale.
Youth Self-Report for Ages 11 to 18 78
The scale measures the emotional and behavioral problems among youth ages 11 to 18. The original scale consists of 124 items, whereas the present study utilized 57 items for the analysis. This scale takes through problem behaviors along with 2 subscales, internalizing and externalizing. Internalizing problems consists of 25 items (eg, “I worry a lot.”). Externalizing problems subscale consists of 32 items (eg, “I argue a lot.”). The participants rated the items on a 3-point Likert scale from 0 (not true) to 2 (true). A high score on each subscale indicates a high level of problem measured by the concerned subscale. The Cronbach’s α on the present sample was 0.87 for internalizing problems and 0.89 for externalizing problems.
Adolescent Well-Being Scale 62
The adolescent well-being scale measured the well-being of adolescents and was devised to pick up possible depression in older children and adolescents. The scale has 18 questions relating to different aspects of adolescents’ lives and how they feel about them (eg, “I feel like crying.”). The participants indicated whether each statement applies to them or not on a 3-point Likert rating scale from 0 (most of the time) to 2 (never). A higher score indicates the likelihood of a depressive disorder. Cronbach’s α on the present sample was 0.63 for well-being.
Bell’s Adjustment Inventory 79
The scale measures the life of the adolescents’ adjustment issues experienced by the individual at various levels. They are home adjustment, health adjustment, social adjustment, and emotionality adjustment. The scale consists of 140 statements that explain various issues experienced. The scale consists of 4 subscales: home adjustment (eg, “Does your mother tend to dominate your home?”), health adjustment (eg, “Are your eyes sensitive to light?”), social adjustment (eg, “Do you find it easy to ask others for help?”), and emotionality adjustment (eg, “Do you daydream frequently?”). The participants marked responses for each statement on a 3-point Likert scale from 0 (yes) to 2 (uncertain). A high score on a subscale indicates a high level of adjustment problem in the area assessed by the concerned subscale. Cronbach’s α on the present sample was 0.88 for home adjustment, 0.93 for health adjustment, 0.33 for social adjustment, and 0.92 emotionality adjustment.
EPOCH Measure of Adolescent Well-Being 63
The scale assesses 5 psychological characteristics, namely engagement, perseverance, optimism, connectedness, and happiness, which foster well-being, healthy, and positive outcomes during adulthood. The scale consists of 20 items that refer to various positive psychological characteristics. The scale has 5 subscales describing 5 highlighted positive psychological variables. Engagement refers to the tendency for psychological involvement and absorption in activities (eg, “I get completely absorbed in what I am doing.”). Perseverance refers to the tenacity in the face of challenge (eg, “I finish whatever I begin.”). Optimism refers to the sense of hope and positive expectations for the future (eg, “I am optimistic about my future”). Connectedness refers to being loved and supported by others (eg, “I have friends that I really care about.”). Happiness refers to a stable positive mood, including being generally cheerful, feeling happy, and loving life (eg, “I am a cheerful person.”). The participants rated each statement on a 5-point Likert scale from 1 (almost never) to 5 (almost always). A high score on each subscale reflects a high level of psychological characteristics measured by the concerned subscale. The Cronbach’s α on the present sample for the subscales engagement, perseverance, optimism, connectedness, and happiness were 0.73, 0.76, 0.77, 0.73, and 0.79, respectively.
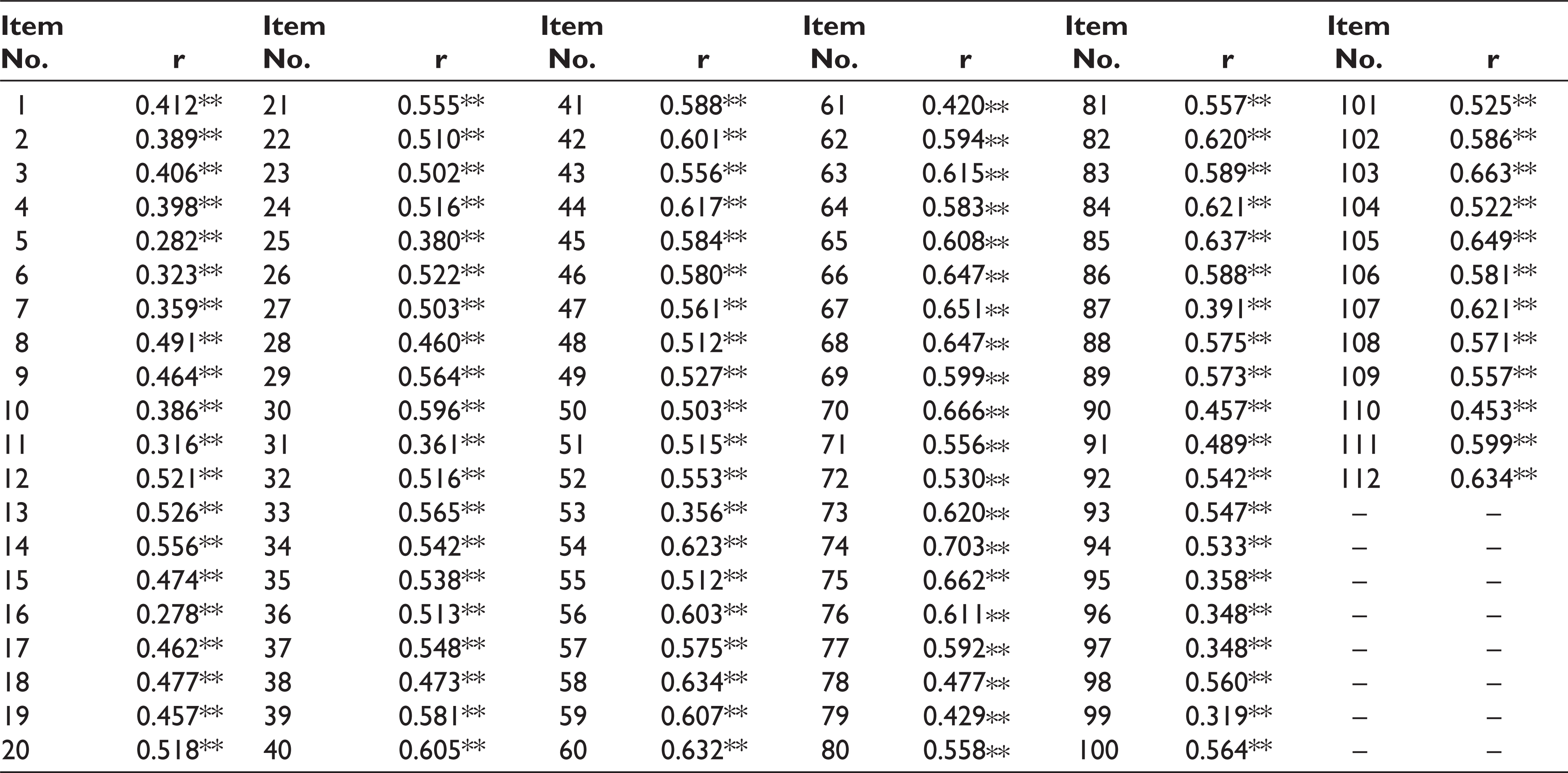
Item-Total Correlation for Psychosocial Risk Factors
Positivity Scale 80
The scale measures the optimistic attitude toward the future of an individual. The scale consists of 15 items that indicate orientation toward the future. The scale consists of 2 subscales. Personal optimism refers to how an individual considers optimism as important (eg, “I have important goals for my life.”). External security refers to a sense of a safety net now and in the future (eg, “I believe that I will be safe from injury.”). The participants responded to each item on the scale using a 5-point Likert scale from 1 (never agree) to 5 (usually agree). A high score on each subscale indicates a high level of psychological characteristics measured by the concerned subscale. The Cronbach’s α on the present sample for subscales personal optimism and external security were 0.92 and 0.83, respectively.
Analysis
Using IBM-SPSS software, version 21 for Windows, the data analysis was carried out. In order to determine whether both the scales measure psychosocial risk and protective factors, respectively in an alternative or parallel form, 81 correlation analysis was carried out between the total score of both scales. The total scores of both scales were negatively correlated (r (312) = –0.17, P < .01). The mean of the psychosocial risk factors scale and psychosocial protective factors scale were 271.44 and 543.12, respectively. The variance of the psychosocial risk scale and protective scale were 8542.90 and 2605.78, respectively. The results indicated that both the scales do not function as parallel forms because the means and variances were not equivalent. 81 Alternatively, the scales measure the psychosocial risk factors and protective factors of the adolescent population independently.
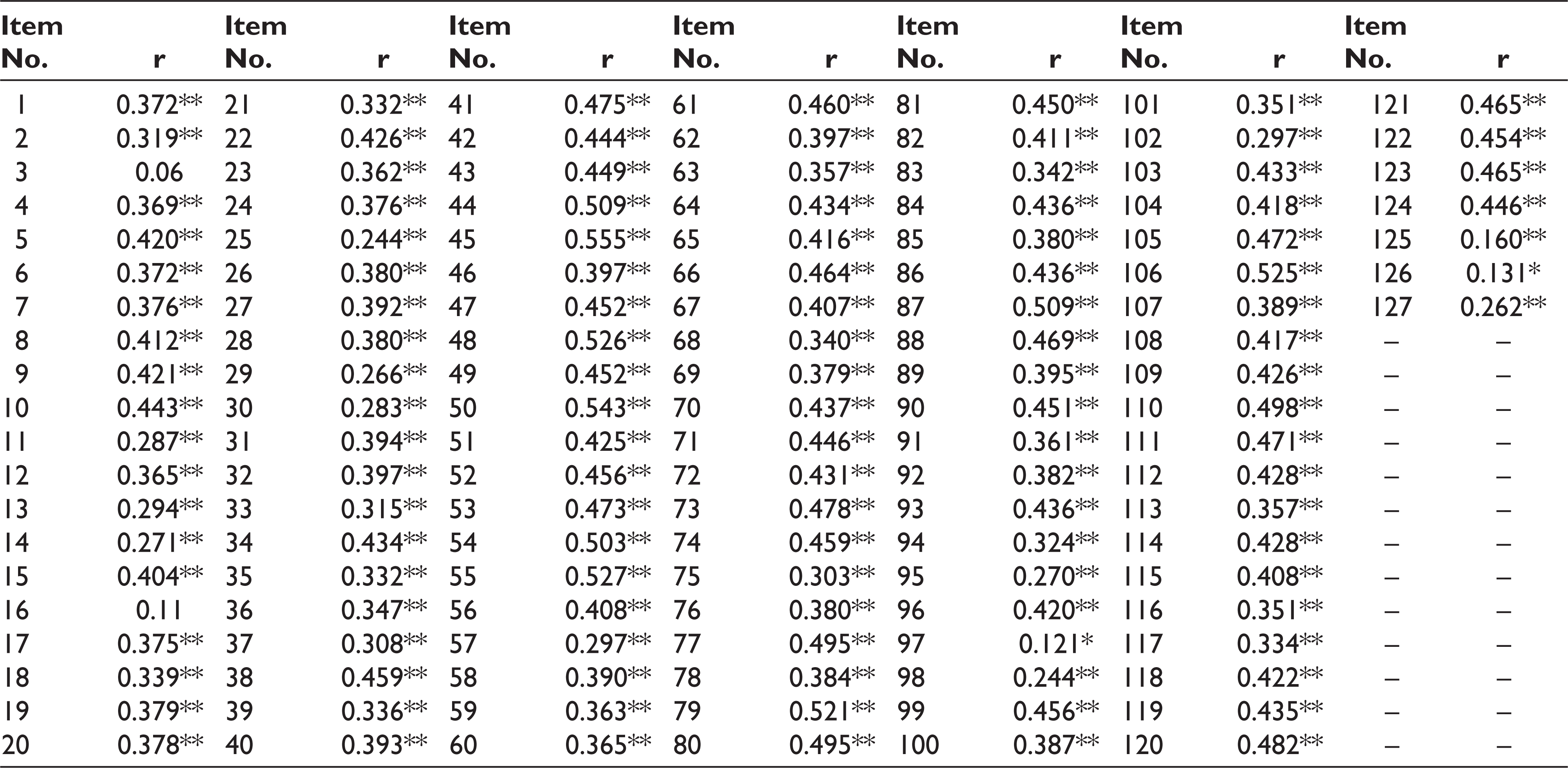
To establish the psychometric properties of the tool, initially, normality was calculated for both scales. Through the Shapiro–Wilk (S–W) test for normality, all items under the psychosocial risk factor scale (n = 112; M = 271.43; SD = 92.43) and protective factor scale (n = 127; M = 543.12; SD = 51.05) were not found to be normally distributed. The item-total correlation was computed to understand the discriminating level of each item with that of the total test score. 82 All the items in the psychosocial risk factors scale significantly correlated with the total score on the scale, where the range of correlation coefficient was from 0.28 to 0.70 (Table 2). Except for 2 items, other items in the psychosocial protective factors scale significantly correlated with the total score on the scale, where the range of correlation coefficient was from 0.13 to 0.53 (Table 3).
Item-Total Correlation for Psychosocial Protective Factors
Principal component analysis was carried out to identify a relatively small number of factors representing the relationship between intercorrelated variables 83 for both scales. Items in both the scales are intercorrelated, at least for the value of r at 0.3 with other items.
The Kaiser–Meyer–Olkin measure of sampling adequacy for the psychosocial risk factor scale was 0.92, and for the protective factor, the scale was 0.83.
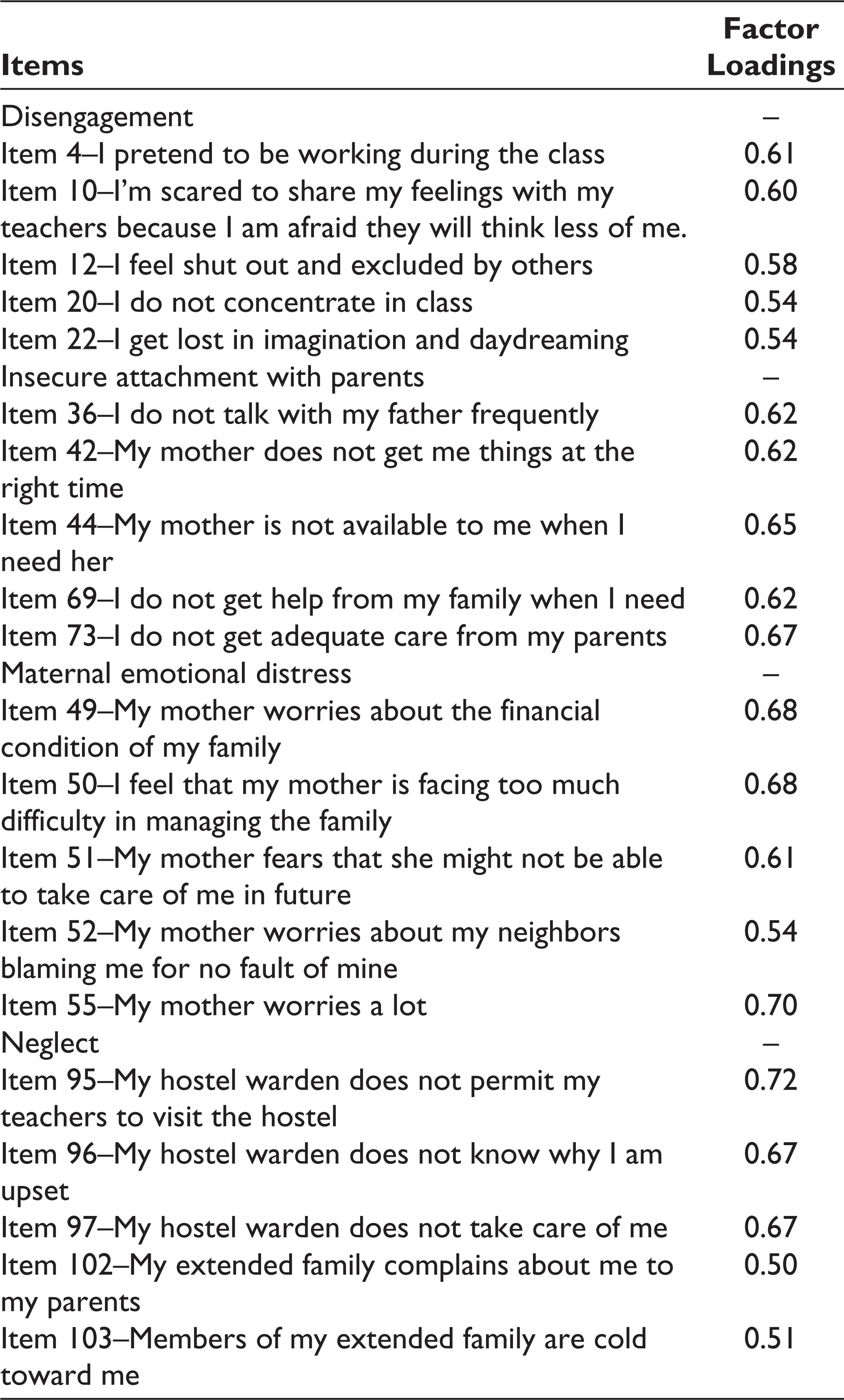
Bartlett’s test of sphericity was significant for Scale 1 (χ 2 (312) = 21426.35; P < .05) and Scale 2 (χ 2 (312) = 22676.42; P < .05). Finally, the communalities were above .6 for both the scales, further confirming that each item shared some common variance with the other. The principal component analysis for the psychosocial risk factors scale, with Kaiser’s criterion of eigenvalues greater than the value generated through parallel analysis,84, 85 constituted 4 factors. They are disengagement (M = 14.02; SD = 5.81), paternal insecure attachment (M = 10.74; SD = 5.77), maternal emotional distress (M = 15.53; SD = 6.50), and neglect (M = 8.51; SD = 4.63). The highest 5-factor loaded items were constituted for final analysis (Table 4).
Showing Factor Loading of Psychosocial Risk Factors Scale by EFA
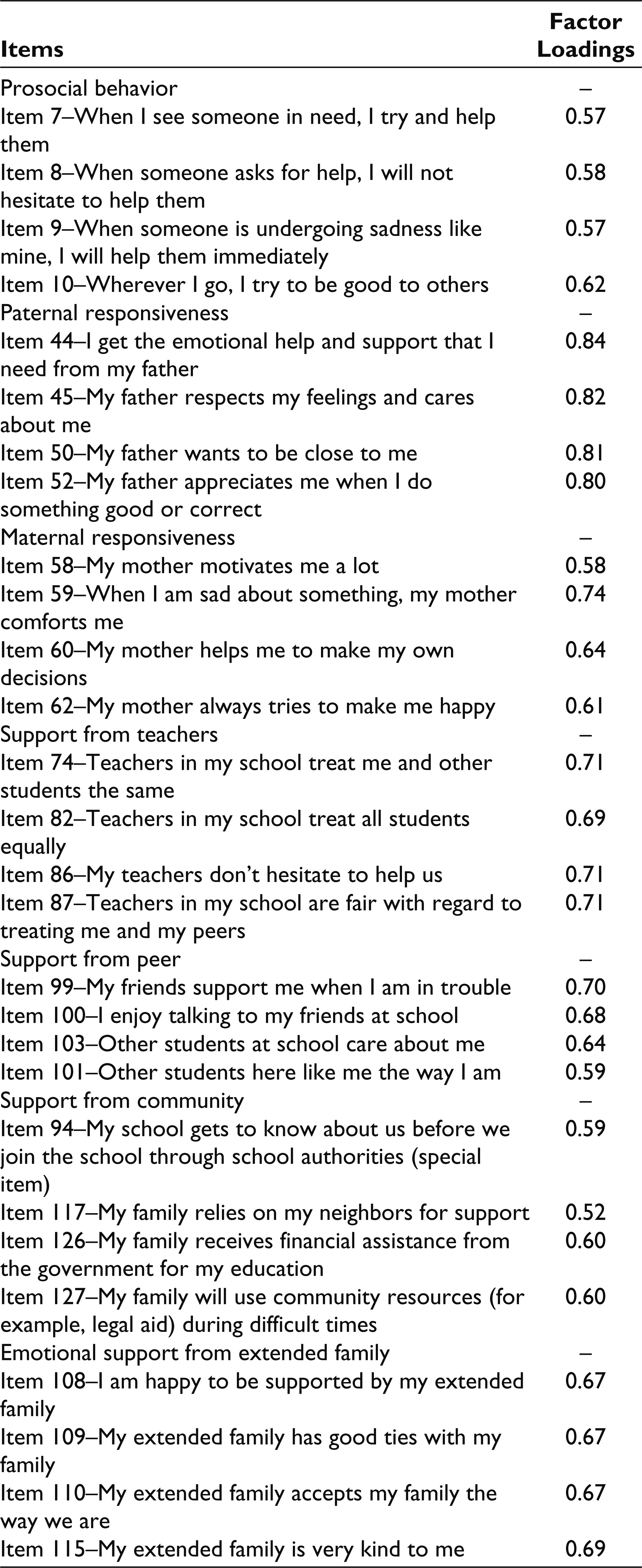
On the other hand, the principal component analysis for the psychosocial protective factors scale, with Kaiser’s criterion of eigenvalues greater than the value generated through parallel analysis, constituted 9 factors. However, the first 7 factors were retained because the eighth and ninth factor had one item each.
The factors which evolved in psychosocial protective factors scale were prosocial behavior (M = 18.29; SD = 2.17), paternal responsiveness (M = 18.01; SD = 3.45), maternal responsiveness (M = 18.41; SD = 2.48), support from teachers (M = 17.46; SD = 3.53), support from peers (M = 17.95; SD = 3.22), support from community (M = 12.0; SD = 4.49), and emotional support from extended family (M = 17.79; SD = 3.16). Highest 4 factor loaded items were constituted for final analysis (Table 5).
Factor Loading of Psychosocial Protective Factors Scale by EFA
Internal Consistency
The Cronbach’s α coefficients were used to evaluate the internal consistency of the psychosocial risk and protective factors scale. The Cronbach’s α coefficients for risk factors and protective factors were 0.87 and 0.83, respectively. The Cronbach’s α coefficients for subscales of the risk factors scale, viz, disengagement, insecure attachment with parents, maternal emotional distress, and neglect were 0.72, 0.78, 0.83, and 0.80, respectively. The Cronbach’s α coefficients for subscales of protective factors such as prosocial behavior, paternal responsiveness, maternal responsiveness, support from teachers, support from peers, support from the community, and emotional support from extended family were 0.73, 0.90, 0.74, 0.82, 0.78, 0.66, and 0.80, respectively. Hence, both scales have adequate internal consistencies.
Convergent Validity
Convergent validity was carried out to understand whether the scale measures risk and protective factors as intended. 86 To test this, linear correlation analysis was carried out to understand the association between the risk factors and protective factors as measured by the new scale developed herein with the risk factors and protective factors measured by other standardized scales. The results for convergent validity are listed further.
Psychosocial Risk Factors Scale.
The overall psychosocial risk factors are positively correlated with home maladjustment, r (312) = 0.30, P < .01, health maladjustment, r (312) = 0.28, P < .01, emotional maladjustment, r (312) = 0.30, P < .01, social maladjustment, r (312) = 0.15, P < .01, overall maladjustment, r (312) = 0.31, P < .01, internalizing problems, r (312) = 0.50, P < .01) and externalizing problems, r (312) = 0.49, P < .01. Meanwhile, overall risk factors negatively correlated with engagement, r (312) = –0.22, P < .01, perseverance, r (312) = –0.29, P < .01, optimism, r (312) = –0.36, P < .01, connectedness, r (312) = –0.37, P < .01, happiness, r (312) = –0.25, P < .01, personal optimism, r (312) = –0.24, P < .01, external security, r (312) = –0.13, P < .05), well-being, r (312) = –0.29, P < .01, r (312) = –0.34, P < .01), and positivity, r (312) = –0.22, P < .01. Risk factors positively correlated with negative outcome 87 and negatively correlated positive outcome.88, 89 This indicates that the risk factor scale and subscales found to have adequate convergent validity.
Disengagement Subscale
Disengagement refers to the lack of involvement in everyday activities. Disengagement is positively correlated with home maladjustment, r (312) = 0.21, P < .01, health maladjustment, r (312) = 0.18, P < .01, emotional maladjustment, r (312) = 0.19, P < .01, overall maladjustment, r (312) = 0.20, P < .01, internalizing problems, r (312) = 0.38, P < .01, and externalizing problems, r (312) = 0.45, P < .01. Meanwhile, disengagement negatively correlated with engagement, r (312) = –0.15, P < .01, perseverance, r (312) = –0.22, P < .01, optimism, r (312) = –0.23, P < .01, connectedness, r (312) = –0.25, P < .01, happiness, r (312) = –0.25, P < .05, personal optimism, r (312) =–0.14, P < .05, well-being, r (312) = –0.25, P < .01, and positivity, r (312) = –0.13, P < .01. This is in line with the findings of the study by Pelton et al, 90 where disengagement indicates the presence of adjustment issues and increases internalizing and externalizing problems among adolescents.91–93 Disengaging oneself from activities increases aggression and violence during late adolescent. 94
Insecure Attachment With Parents Subscale
Insecure attachment with parents refers to the stress and anxiety in child’s attachment with parents. The subscale is positively correlated with home maladjustment, r (312) = 0.21, P < .01, health maladjustment, r (312) = 0.18, P < .01, social maladjustment, r (312) = 0.13, P < .05, emotional maladjustment, r (312) = 0.18, P < .01, overall maladjustment, r (312) = 0.21, P < .01, internalizing problems, r (312) = 0.34, P < .01), and externalizing problems, r (312) = 0.31, P < .01. Insecure attachment toward parents is usually the presence of anxiousness in relationships and avoidance of closeness 95 with parents. Such attachment subsequently led to mental health problems. 95 Meanwhile, insecure attachment with parents negatively correlated with engagement, r (312) = –0.14, P < .05, perseverance, r (312) = –0.17, P < .01, optimism, r (312) = –0.24, P < .01, connectedness, r (312) = –0.30, P < .01, happiness, r (312) = –0.17, P < .01, personal optimism, r (312) = –0.17, P < .01, well-being, r (312) = –0.24, P < .01, and positivity, r (312) = –0.16, P < .01. The findings of the present study are in line with findings, where insecure attachment with parents results in adjustment issues, anxiety, and depressive symptoms.96–99 The problems with paternal relationship predict risk conditions as well as holds negative associations with factors enhancing psychosocial health of adolescents.100, 101
Maternal Emotional Distress Subscale
Maternal emotional distress refers to the psychological distress in the mother that negatively affects the behavior of the adolescent child. Maternal emotional distress subscale is positively correlated with home maladjustment, r (312) = 0.23, P < .01, health maladjustment, r (312) = 0.23, P < .01, social maladjustment, r (312) = 0.14, P < .05, emotional maladjustment, r (312) = 0.26, P < .01, overall maladjustment, r (312) = 0.25, P < .01, internalizing problems, r (312) = 0.47, P < .01, and externalizing problems r (312) = 0.40, P < .01. Meanwhile, maternal emotional distress is negatively correlated with engagement, r (312) = –0.20, P < .01, perseverance, r (312) = –0.26, P < .01, optimism, r (312) = –0.30, P < .01, connectedness, r (312) = –0.27, P < .01, happiness, r (312) = –0.23, P < .01, personal optimism, r (312) = –0.17, P < .01, well-being, r (312) = –0.29, P < .01, and positivity, r (312) = –0.16, P < .01. This result is similar to the result reported by Gondoli and Silverberg, 102 where maternal emotional distress has a positive association with anxiety and negative association with interpersonal relationship. Maternal distress leads to disruption in parental behavior that threatens adolescent health.103, 104
Neglect Subscale
Neglect refers to the absence of care and attention from various resources. Neglect is positively correlated with home maladjustment, r (312) = 0.24, P < .01, health maladjustment, r (312) = 0.25, P < .01, emotional maladjustment, r (312) = 0.24, P < .01, overall maladjustment, r (312) = 0.25, P < .01, internalizing problems, r (312) = 0.28, P < .01, and externalizing problems, r (312) = 0.28, P < .01. Meanwhile, neglect is negatively correlated with engagement, r (312) = –0.13, P < .05, perseverance, r (312) = –0.20, P < .01, optimism, r (312) = –0.28, P < .01, connectedness, r (312) = –0.26, P < .01, happiness, r (312) = –0.18, P < .01, personal optimism, r (312) = –0.25, P < .01, external security, r (312) = –0.13, P < .05, well-being, r (312) = –0.24, P < .01, and positivity, r (312) = –0.23, P < .01. The results of the present study are in line with the study by Lounds et al, 105 where the neglect scores were positively correlated with potential abuse and negatively related with parental relationships. Neglect is an obvious risk condition in the psychosocial health of adolescent population. Neglect results in maladjustment and psychological distress that immensely affects overall development of adolescents.106, 107
Psychosocial Protective Factors Scale
Overall protective factors negatively correlated with home maladjustment, r (312) = –0.17, P < .01, health maladjustment, r (312) = –0.12, P < .05, emotional maladjustment, r (312) = –0.18, P < .01, overall adjustment, r (312) = –0.16, P < .01, internalizing problems, r (312) = –0.25, P < .01, and externalizing problems, r (312) = –0.26, P < .01. Overall protective factors positively correlated with perseverance, r (312) = 0.12, P < .01. Protective factors enhance the psychosocial development of adolescent children despite risk.108, 109 Because the scale and subscales of protective factors are associated with positive outcomes 110 and negative outcomes 111 measured in this study in the hypothesized direction, the scale and subscales are found to have adequate convergent validity.
Prosocial Behavior Subscale
Prosocial behavior refers to the behavior that has the tendency to benefit others. Prosocial negatively correlated with home maladjustment, r (312) = –0.17, P < .01, health maladjustment, r (312) = –0.14, P < .05, emotional maladjustment, r (312) = –0.15, P < .01, internalizing problems, r (312) = –0.20, P < .01, and externalizing problems, r (312) = –0.27, P < .01. Prosocial behavior positively correlated with personal optimism, r (312) = 0.15, P < .05, external security, r (312) = 0.15, P < .01, well-being, r (312) = 0.12, P < .05), and positivity, r (312) = 0.15, P < .01. This finding is in line with the findings of existing researches which argue that prosocial behavior has positive association with optimism 112 and is negatively related with adjustment issues. 113 Prosocial behavior fosters adolescents’ tendency to exhibit perspective taking and empathic concern, 114 and hence may be seen as relevant to positive adaptation.
Paternal Responsiveness Subscale
Paternal responsiveness refers to the father’s attention to the adolescent’s needs and warmth to the requirement. Paternal responsiveness is negatively correlated with home maladjustment, r (312) = –0.13, P < .05) and did not correlate with other variables. The finding reveals that paternal responsiveness plays an active role in children’s adjustment issues at home. Paternal responsiveness guides socialization and the learning process and helps improve assertiveness and reduce substance abuse while facing adverse situations.115–117 Reduced paternal responsiveness predicts aggression within an individual. 118
Maternal Responsiveness
Maternal responsiveness refers to the mother’s attention to the adolescent’s needs and warmth to the requirement. Maternal responsiveness negatively correlated with home maladjustment, r (312) = –0.11, P < .05, internalizing problems, r (312) = –0.06, P < .01, and externalizing problems, r (312) = –0.16, P < 0.01. Maternal responsiveness reduces the emotional problems and adjustment issues that are likely to emerge at home because of at-risk conditions. Maternal responsiveness promotes intellectual growth and a sense of security and trust. 119
Support From Teachers Subscale
Support from teachers refers to the teachers’ sensitive, responsive, and positive interactions that help manage student behavior. Teachers support negatively correlated with internalizing problems, r (312) = –0.15, P < .01, and externalizing problems, r (312) = –0.22, P < .01. Teachers support positively correlated with perseverance, r (312) = 0.15, P < .01. These findings align with the studies that found teachers’ support buffers behavioral difficulties, increases competence, and reduces attachment issues.120–122 Teachers’ support and good quality child-teacher interactions reduce aggression and improve self-regulation. 123
Support From Peer Subscale
Peer support refers to the sensitive, responsive, and positive interactions of peer with adolescent, which manages the adolescent behavior. Peer support is negatively correlated with home maladjustment, r (312) = –0.15, P < .01, health maladjustment, r (312) = –0.18, P < .01, social maladjustment, r (312) = –0.14, P < .05, emotional maladjustment, r (312) = –0.16, P < .01, overall maladjustment, r (312) = –0.18, P < .01, internalizing problems, r (312) = –0.30, P < .01, and externalizing problems, r (312) = –0.30, P < .01. Peer support positively correlated with perseverance, r (312) = 0.15, P < .01, optimism, r (312) = 0.12, P < .05, connectedness, r (312) = 0.16, P < .01, happiness, r (312) = 0.12, P < .05, personal optimism, r (312) = 0.20, P < .01, external security, r (312) = 0.14, P < .05, well-being, r (312) = 0.15, P < .05, and positivity, r (312) = 0.19, P < .01. Peer support reduces adjustment problems and emotional issues. This finding is in line with the finding of existing studies: Lack of peer support indicates adjustment issues in the academic platforms. 124 Peer support promotes academic motivation, classroom engagement, and school belongingness. 125 Similarly, peer support positively influences adolescents’ process of making their life decisions. 126 Consistent support from peers strengthens the factors that enhance the development of adolescents. 127
Support From Community Subscale
Support from the community refers to the positive interactions of individuals with community resources that help manage the adolescents’ behavior. Community support is negatively correlated with optimism, r (312) = –0.20, P < .01, connectedness, r (312) = –0.14, P < .05, happiness, r (312) = –0.12, P < .05, personal optimism, r (312) = –0.23, P < .01, external security, r (312) = –0.14, P < .05, well-being, r (312) = –0.16, P < .01, and positivity, r (312) = –0.21, P < .01. Community resources enhance the satisfaction of life and posttraumatic growth in adolescents. 128 It also safeguards children from growing in the risk condition. 129
Emotional Support by Extended Family Subscale
Emotional support from extended family refers to the sensitive, responsive, and positive interactions of the individuals with the extended family that help manage the adolescents’ behavior. Emotional support by extended family is negatively correlated with home maladjustment, r (312) = –0.15, P < .01, emotional maladjustment, r (312) = –0.12, P < .05, overall adjustment, r (312) = –0.12, P < .01, internalizing problems, r (312) = –0.16, P < .01, and externalizing problems, r (312) = –0.12, P < .05. Emotional support by extended family positively correlated with optimism, r (312) = 0.15, P < .05) and connectedness, r (312) = 0.12, P < .05. Extended family support usually provides strength during economical constrains. 130
Discriminant Validity
Discriminant validity is established when the items within the constructs are highly correlated than with latent constructs. 131 This is calculated by average variance extracted (AVE) analysis, where the square root of AVE should be greater than the correlation value among any pair of latent constructs.
where λi is factor loadings in a construct and εi is error variance.
In the psychosocial risk factors scale, the square root of the average value extracted was 0.57 for disengagement subscale, 0.63 for the paternal insecure attachment subscale, 0.65 for the maternal distress subscale, and 0.62 for the neglect subscale. The square root value of AVE for every subscale is higher than the correlation values of all the other correlated study variables from established scales used in the present study. In the psychosocial protective factors scale, the square root of average value extracted was 0.14 for prosocial behavior subscale, 0.27 for paternal responsiveness subscale, 0.16 for maternal responsiveness subscale, 0.20 for support from teacher subscale, 0.17 for support from peer subscale, 0.13 for support from the community, and 0.18 for emotional support from extended family subscale. The square root of the AVE value for the prosocial behavior subscale is higher than the correlation value of well-being and health maladjustment. The square root of the AVE value for the paternal responsiveness subscale is higher than the correlation value of home maladjustment. The square root of AVE value for the maternal responsiveness subscale is higher than the correlation value of internalizing problems and perseverance. The square root of the AVE value for support from the teacher’s subscale is higher than the correlation value of internalizing problems and perseverance. The square root of AVE value for support from peer subscale is higher than the correlation value of home maladjustment, social maladjustment, emotional maladjustment, engagement, perseverance, optimism, connectedness, personal optimism, external security, and well-being. The square root of the AVE value for support from the community subscale is higher than the correlation value of happiness. The square root of the AVE value for emotional support from the external family subscale is higher than the correlation value of home maladjustment, emotional maladjustment, overall maladjustment, interna-lizing problems, externalizing problems, engagement, optimism, and connectedness. Hence, the psychosocial risk and protective factors scale and subscales have adequate discriminant validity.
The new tool assesses risk and protective factors comprehensively based on the socioecological perspective of adolescent development. Both the scales are intended to identify the risks and protective factors among rural adolescent children between 12 and 16 years of age. Even though the tool does not address risk or protective factors at the school level, the multidimensional nature of the scale attempts to delineate the risk and protective factors at the individual level, family level, and community level among the target population. The findings of the present study should be understood within the context of limitations of the study. The criterion validity was not demonstrated for the tool, which can help understand the performance of the scale in different conditions like adolescents living in institutions, those living with a single parent, etc. When responding to the items, the children might underreport undesirable attributes and over-reporting desirable attributes. 132 In the present study, the students completed the survey in the presence of the teacher/tutor, which could have influenced their responses to the survey items, especially those related to their classroom behavior (eg, I pretend to be working during the class). The new scale did not include negative scoring, which could control acquiescence bias. The new tool could not measure and control variables like self-regulation, life satisfaction, gratitude, and other positive psychological variables among adolescents. Future research can consider including these variables to examine protective factors for at-risk adolescent populations. Inputs from children of incarcerated prisoners were not considered for scale development in this study. Including narratives from children of incarcerated prisoners may provide additional insight into the scale development.
Conclusion
The psychosocial risk factors scale developed herein intends to measure factors that challenge healthy psychosocial development. The factors extracted from the psychosocial risk factors scale through exploratory factor analysis were found to measure 4 psychosocial risk factors: disengagement, insecure attachment with parents, maternal emotional distress, and neglect. The psychosocial protective factors scale developed herein intends to measure factors that buffer against the devastating effects of adverse conditions and promote healthy psychosocial development. The factors extracted from the psychosocial protective factors scale through exploratory factor analysis were found to measure 7 psychosocial protective factors: prosocial behavior, paternal responsiveness, maternal responsiveness, support from teachers, support from peer, support from community, and emotional support from extended family. The psychosocial risk and protective factors scales are found to have adequate internal consistency. The results of linear correlational and average variance extracted analyses of the psychosocial risks scale and psychosocial protective factors scale show that the scales have adequate convergent validity and discriminant validity.
Implications
The development of a tool to measure psychosocial risk and protective factors brings researchers closer to classifying psychosocial risk and protective factors among at-risk adolescent populations. The scales developed herein provide a deeper insight into risk and protective factors among high-risk adolescents. The new scale will open new possibilities for further research focusing on examining the impact of psychosocial health on indicators of mental health, well-being, quality of life, and resilience. This scale can serve as an additional resource in positive psychology and developmental psychology and help investigate the risk and protective factors to offer counseling to high-risk adolescents. As a theory-driven assessment tool, the risk and protective factors scale will effectively evaluate resilience-based programs or mental health-promoting programs at family, school, and community levels. The study provides insight for using mixed methods evaluation to develop assessment tools in the positive psychological field of research. The nature and quality of positive psychological assessment tools will be enhanced if the item generation for the tool includes the experiences of the target population. Most importantly, the factors at various levels of an adolescent’s life can serve as key pointers for policymakers to cultivate talents in multiple ways targeting multiple levels in the socioecological system to help at-risk adolescents fight the adverse conditions in their lives.
Footnotes
Acknowledgements
This research was fully supported by the Centrally Administered Doctoral Fellowship funded by the Indian Council of Social Science Research (ICSSR; Sanction order/Award No. RFD/2017–18/PSY/GEN/253 dated January 9, 2018). We thank the participants who took part in this research. We also thank the authorities who approved to carry out data collection.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.