
Abstract
Background
Myocardial infarction (MI) continues to be a leading contributor to illness and death worldwide, even in the face of substantial therapeutic and preventive interventions. Polygala tenuifolia, a traditional medicinal herb rich in diverse bioactive compounds, exhibits a broad range of therapeutic effects; however, its cardioprotective role has not been fully elucidated.
Purpose
The herein study was proposed to examine the cardioprotective efficacy of the ethanolic extract of P. tenuifolia (PTEE) and was assessed in an isoproterenol (ISO)-induced MI model using male Wistar albino rats.
Materials and Methods
Animals were randomly assigned to four groups: control, ISO-treated, and two groups pre- and co-treated with PTEE for 20 days, followed by ISO administration on days 19 and 20. On day 21, blood and heart tissue samples were collected for biochemical and molecular analyses.
Results
PTEE administration modulated serum biochemical parameters, enhanced antioxidant defense, stabilized myocardial ionic balance, reduced pro-inflammatory cytokine levels, and regulated nuclear factor kappa B/heme oxygenase-1/NAD(P)H quinone oxidoreductase-1 (NF-κB/HO-1/NQO-1) signaling pathways in MI-induced rats. Overall, PTEE exhibited significant cardioprotective activity by mitigating oxidative and inflammatory damage.
Conclusion
The present results imply that PTEE may be pursued as a therapeutic option for managing MI and allied cardiovascular disorders; however, further mechanistic and long-term studies are warranted to substantiate its clinical applicability.
Introduction
Myocardial infarction (MI) remains a primary source of cardiovascular disease burden worldwide despite substantial progress in diagnostic and therapeutic approaches (Mechanic et al., 2025). Cardiovascular diseases collectively account for nearly 19 million deaths each year, with ischemic heart disease responsible for almost half of these fatalities (Roth et al., 2019). Approximately 785,000 people in the United States experience a new MI each year, and an MI-related death occurs every minute (Jneid et al., 2013). Between 2005 and 2014, an estimated 805,000 MI-related deaths were reported, reaffirming heart disease as the nation’s leading cause of death (Lohita et al., 2023). Globally, the prevalence of MI is estimated at 3.8% among individuals aged 60 years or less and 9.5% among those aged 60 years or older (Salari et al., 2023). While improved healthcare infrastructure and preventive strategies have led to a decline in MI incidence in industrialized countries, rates continue to rise in developing regions (Nascimento et al., 2019). Notably, recent evidence suggests an increasing trend of MI occurrence among younger adults (<45 years; Kayikcioglu et al., 2022), which presents a growing clinical and socio-economic concern due to its association with premature morbidity, long-term disability, and reduced productivity.
The pathophysiology of MI is complex, involving a cascade of interconnected mechanisms, including oxidative stress, inflammation, and disruption of cellular signaling pathways. Atherosclerotic plaque rupture or erosion triggers thrombotic occlusion, impairing coronary blood flow and leading to cardiomyocyte injury. Oxidative stress plays a pivotal role in MI progression, generating reactive oxygen species (ROS) that exacerbate inflammation, mitochondrial dysfunction, and cell death. Inflammatory responses further amplify tissue damage, with pro-inflammatory cytokines and chemokines perpetuating a vicious cycle of injury and repair (Młynarska et al., 2024). Approximately 70% of fatal MI cases are attributed to atherosclerosis, with modifiable risk factors, such as smoking, hypertension, obesity, hyperlipidemia, and physical inactivity, accounting for the majority of cases (Deng et al., 2018; Moses et al., 2025). Among individuals under 55 years, smoking remains the most significant risk factor, contributing to nearly 80% of events (Allagbé et al., 2025). Premature atherosclerosis explains nearly 90% of MI in young adults, while non-atherosclerotic causes, like spontaneous coronary artery dissection, coronary vasospasm, hypercoagulability, and drug-induced ischemia, comprise the remainder (Gulati et al., 2020; Krittanawong et al., 2023). An elevated inflammatory profile, particularly high-sensitivity C-reactive protein (hs-CRP), alongside insulin resistance and sedentary lifestyle, further increases susceptibility (Zarich et al., 2006).
Advances in MI therapy have improved outcomes, yet major challenges remain. While primary percutaneous coronary intervention (PCI) is the standard treatment, reperfusion can cause oxidative stress and inflammatory injury (Vasconcelos-Cardoso & Girao, 2022). Despite progress in pharmacological therapy, efficacy remains limited (Saito et al., 2023). Emerging nanoparticle-based systems offer targeted delivery with fewer side effects (Pan et al., 2021). Treatment complexity increases in pregnancy-associated MI, as several standard drugs are contraindicated, necessitating careful, multidisciplinary management (Alameh et al., 2021). Phytochemicals have emerged as promising therapeutic agents for MI due to their diverse cardioprotective mechanisms. Bioactive plant compounds, such as polyphenols, flavonoids, alkaloids, and others, exert an array of pharmacological actions (Arshad et al., 2025; Li et al., 2025; Riaz et al., 2023). These natural agents can be used preventively or as adjuncts to conventional therapies, potentially enhancing efficacy while minimizing drug-related toxicity (Chen et al., 2022). In myocardial ischemia/reperfusion injury, phytochemicals modulate key pathological pathways, including oxidative stress, apoptosis, autophagy, inflammation, and calcium overload (He et al., 2022).
Polygala tenuifolia, a widely used herb in traditional Chinese medicine, demonstrates a broad range of therapeutic effects attributed to its ethanol extracts and bioactive constituents. Recent research highlights its notable neuroprotective potential, particularly in mitigating Alzheimer’s disease by inhibiting beta-amyloid aggregation and preventing neuronal degeneration (Wang & Zhang, 2023). The plant is rich in more than 140 identified compounds, with principal active molecules, such as tenuifolin, polygalaxanthone III, and senegenin. These constituents possess diverse therapeutic properties encompassing antioxidant, anti-inflammatory, anti-depressant, anti-tumor, and anti-arrhythmic effects (Garg et al., 2023). However, the cardioprotective potential of the ethanolic extract of P. tenuifolia (PTEE) against MI remains to be elucidated. This study aimed to investigate the cardioprotective effects of PTEE against isoproterenol (ISO)-induced MI in rats, evaluating biochemical markers of oxidative stress, inflammation, and myocardial ionic levels, alongside assessing modulation of key molecular pathway (nuclear factor kappa B/heme oxygenase-1/NAD(P)H quinone oxidoreductase-1 [NF-κB/HO-1/NQO-1]) changes.
Materials and Methods
Animals
In total, 24 healthy male Wistar albino rats were sourced from a scientifically accredited laboratory facility and used for this study. The study was approved by the institutional ethics committee for animal care and use and conducted in accordance with the institutional ethics committee guidelines.
Following a 2-week acclimatization period, the animals were housed in sterilized rectangular polypropylene rodent housing units with unrestricted access to sufficient nutrition and hydration throughout the experimental period. The animals were housed under standard laboratory conditions (temperature 19°C–25°C, relative humidity 30%–70%), with a 12/12-h light–dark cycle, and provided with a conventional laboratory pellet diet.
Experimental Design
Animals were randomly allocated to treatment and control groups, with six animals per group, using a computer-generated randomization schedule. Investigators were blinded to group assignments during data collection and analysis. Throughout the study, body weight variation within each group did not exceed ±20% of the mean body weight. Group I served as the untreated control and received 0.1% NaCl. Group II was administered ISO (85 mg/kg, intraperitoneally) to induce MI, a non-selective β-agonist, on days 19 and 20 of the protocol. Groups III and IV received oral administration of PTEE at 100 and 200 mg/kg, respectively, for 20 days, with ISO administered on days 19 and 20. On day 21, animals were euthanized by CO2 asphyxiation. Post-mortem samples included heart tissue for organ analysis, and blood was collected for serum isolation.
Estimation of Serum Biochemical Parameters
Serum total protein (TP), C-reactive protein (CRP), and uric acid (UA) levels were estimated using commercially available diagnostic kits in compliance with the manufacturer’s guidelines for use. TP concentration was measured using the Bradford assay, and CRP levels and UA were determined using kits procured from the manufacturer Elabscience, USA. All estimations were performed under standardized laboratory conditions to ensure analytical accuracy and reproducibility.
Assessment of Antioxidant Biomarker
Rat heart tissue was homogenized at a 10% (w/v) concentration in 50 mM phosphate buffer (pH 7.4) containing 1 mM ethylenediaminetetraacetic acid (EDTA), followed by centrifugation at 10,000 × g for 15 min at 4°C. The resulting supernatant served for antioxidant assays, and protein content was quantified using the Bradford (1976) method.
Superoxide Dismutase
Superoxide dismutase (SOD) activity was quantified by the Beauchamp and Fridovich (1971) method based on the inhibition of nitroblue tetrazolium (NBT) reduction. Absorbance was read at 560 nm, and enzyme activity was expressed as U/mg protein.
Reduced Glutathione
Glutathione (GSH) levels were estimated following Ellman (1959) using 5,5′-dithiobis-(2-nitrobenzoic acid) (DTNB) reagent. The yellow chromogen formed was measured at 412 nm, and results were reported as µmol GSH per gram of tissue.
Catalase
Catalase (CAT) activity was measured following the protocol of Aebi (1984) by tracking the decrease in H2O2 absorbance at 240 nm. The rate was calculated using the molar extinction coefficient of H2O2 and expressed as micromoles of H2O2 decomposed per minute per milligram of protein. All absorbance readings were recorded using a UV–visible spectrophotometer, and assays were performed in triplicate to ensure reproducibility.
Assessment of Myocardial Ionic Levels
The electrolytes sodium (Na+), potassium (K+), and calcium (Ca2+) levels were quantified in the heart homogenate of experimental animals using the commercially available kits procured from Elabscience, USA. The assays were carried out per the supplier’s recommended protocol.
Quantification of Pro-inflammatory Cytokines
Serum levels of tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), and interleukin-1β (IL-1β) were quantified using commercial ELISA kits (R&D Systems, USA) in accordance with the supplier’s protocol. Blood was collected by cardiac puncture, allowed to clot, and centrifuged at 3,000 × g for 10 min at 4°C to obtain serum, which was stored at −80°C until analysis. Aliquots of 50 µL serum were added to antibody-coated wells, followed by incubation with biotinylated detection antibodies and streptavidin–horseradish peroxidase (HRP). The assay was developed with a 3,3′,5,5′-tetramethylbenzidine (TMB) substrate, stopped with 1 N H2SO4, and absorbance was read at 450 nm. Cytokine concentrations were derived from standard curves and expressed as pg/mL. Each sample was measured in triplicate.
Quantification of NF-κB/HO-1/NQO-1 Protein Levels
NF-κB, HO-1, and NQO-1 protein levels were measured in the experimental animals using commercial ELISA kits procured from MyBioSource. The assay was performed in triplicate procedures, following the manufacturer’s instructions. Absorbance was measured at 450 nm.
Statistical Analysis
Data are shown as mean ± SD. Statistical analyses were performed with GraphPad Prism. Group comparisons were made using one-way analysis of variance (ANOVA) followed by Tukey’s post hoc test to adjust for multiple comparisons. Significance was set at p < .05.
Results
Ethanolic Extract of Polygala tenuifolia Regulated Serum Biochemical Parameters in Myocardial Infarction Rodent Model
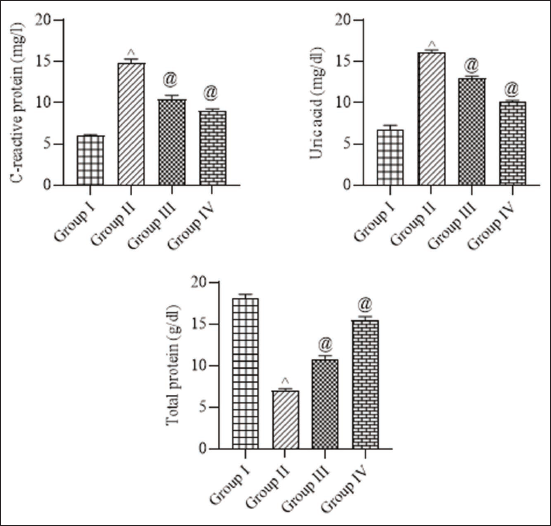
Serum levels of TP, CRP, and UA were evaluated to assess the inflammatory and metabolic alterations associated with MI, as illustrated in Figure 1. Induction of MI resulted in a marked elevation of CRP and UA levels than control rats, which displayed significantly lower values. PTEE administered at doses of 100 and 200 mg/kg in MI-induced rats significantly attenuated CRP and UA levels, respectively. Conversely, TP levels, which were reduced in MI rats, were significantly restored following PTEE treatment at the 100 and 200 mg/kg doses, respectively. Control animals exhibited the highest TP levels relative to all experimental groups. These results indicate that PTEE administration mitigates MI-induced inflammatory and metabolic disturbances in a dose-dependent manner.
Ethanolic Extract of Polygala tenuifolia Enhanced Antioxidant Status in Myocardial Infarction Rodent Model
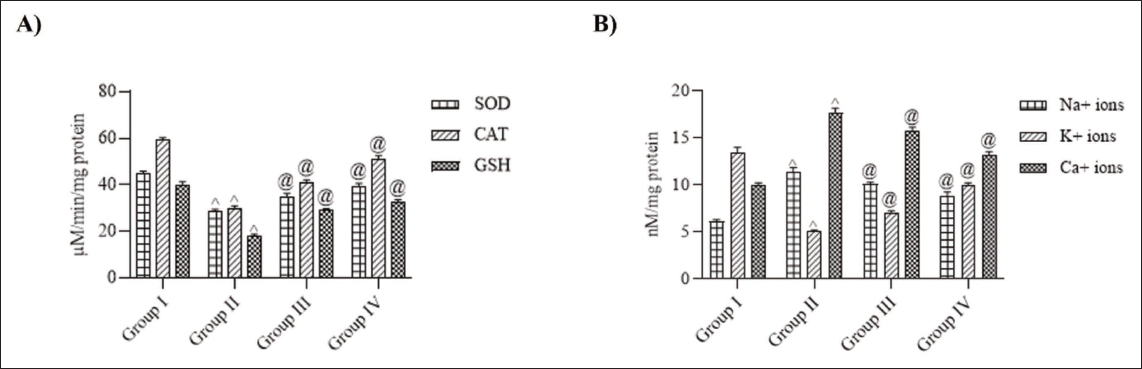
Antioxidant defense enzyme activities showed marked variations among the experimental groups (Figure 2A). The control rats exhibited normal antioxidant enzyme levels, reflecting balanced oxidative status. In contrast, MI-induced rats demonstrated a significant reduction in SOD, CAT, and GSH activities than the control group, indicating pronounced oxidative stress and depletion of endogenous antioxidant reserves. Administration of PTEE at 100 mg/kg resulted in a noticeable restoration of these antioxidant parameters, while treatment with 200 mg/kg PTEE produced a more pronounced improvement. The enzyme activities in Group IV approached values close to those of the control group, suggesting that PTEE supplementation effectively enhanced enzymatic and non-enzymatic antioxidant defenses, thereby mitigating oxidative damage associated with myocardial injury.
Ethanolic Extract of Polygala tenuifolia Altered Myocardial Ionic Levels in Myocardial Infarction Rodent Model
Ionic concentrations in myocardial tissue exhibited significant variations among the experimental groups (Figure 2B). Control rats displayed normal ionic concentrations, reflecting proper membrane integrity and ionic homeostasis. In MI-induced rats, a substantial elevation in Na⁺ and Ca²⁺ levels was observed, accompanied by a marked reduction in K⁺ concentration compared with the control. PTEE treatment at 100 mg/kg significantly restored Na⁺, K⁺, and Ca²⁺ levels toward normal values, suggesting partial protection against myocardial electrolyte disturbances. Rats treated with 200 mg/kg PTEE demonstrated a more pronounced normalization of ionic concentrations, approaching values similar to those in the control. These findings imply that PTEE supplementation stabilizes membrane integrity and preserves ionic balance, thereby protecting cardiac tissue from infarction-induced ionic dysregulation.
Ethanolic Extract of Polygala tenuifolia Attenuated Pro-inflammatory Cytokine Levels in Myocardial Infarction Rodent Model
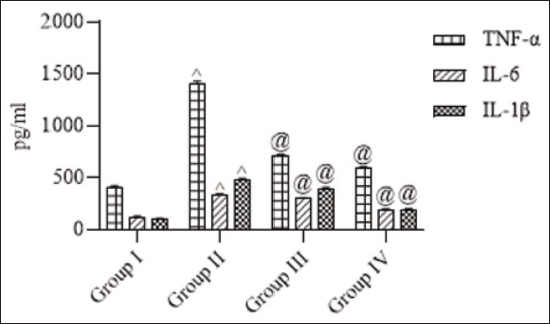
The impact of MI on pro-inflammatory cytokine levels was evaluated, and the results are presented in Figure 3. MI induction rendered enhanced elevation in pro-inflammatory cytokine levels compared to control rats. TNF-α, IL-6, and IL-1β levels were increased in the MI rats when compared with the control. However, the administration of PTEE at 100 and 200 mg/kg significantly attenuated these increases in a dose-dependent manner.
Ethanolic Extract of Polygala tenuifolia Altered NF-κB/HO-1/NQO-1 Levels in Myocardial Infarction Rodent Model
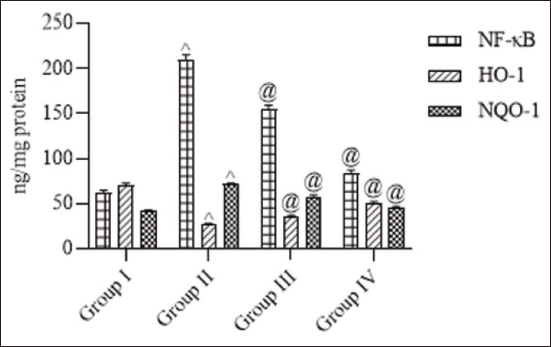
NF-κB, HO-1, and NQO-1 levels were analyzed to assess the inflammatory and antioxidant status in MI-induced rats (Figure 4). MI induction resulted in a significant upregulation of NF-κB compared to the control group, indicating enhanced inflammatory signaling. Treatment with PTEE at 100 and 200 mg/kg markedly reduced NF-κB level, demonstrating its inhibitory effect on inflammation. Conversely, HO-1 and NQO-1 levels, which were significantly decreased in MI rats relative to controls, were restored upon PTEE administration.
Discussion
In recent years, traditional oriental herbal medicines have gained considerable scientific and clinical interest owing to their long history of therapeutic application and perceived safety due to their natural origin (Jiang, 2005; Liu et al., 2008). These botanical formulations are extensively utilized for the prevention and management of various pathological conditions (Tang et al., 2008). P. tenuifolia Willd., a perennial herb officially listed in all editions of the Chinese Pharmacopoeia, is predominantly grown in China (Shanxi Province). Its dried root, known as Polygalae Radix or “Yuan Zhi,” has been employed in traditional Chinese medicine for over two millennia as a tonic, sedative, and expectorant and to enhance memory and cognitive performance (Lacaille-Dubois et al., 2020; Liu et al., 2019).
Extensive pharmacological investigations have revealed that P. tenuifolia exhibits multiple bioactivities, including anti-inflammatory, neuroprotective, anti-depressant, anti-cancer, and sedative-hypnotic effects (Cheng et al., 2006; Cheong et al., 2011; Deng et al., 2020; Xin et al., 2012; Yao et al., 2010). Moreover, extracts and isolated compounds from P. tenuifolia demonstrate significant neuroprotective potential by modulating amyloid-beta (Aβ)-associated toxicity. For example, PSM-04, a crude extract from P. tenuifolia root, has been shown to suppress Aβ aggregation, attenuate oxidative stress, prevent neuronal apoptosis, and upregulate SOD-2 expression in transgenic mouse models (Park et al., 2019). Similarly, BT-11, an extract from the dried root, inhibited acetylcholinesterase activity in a non-competitive and dose-dependent manner in Aβ₁–₄₂-induced rat models (Park et al., 2002). We proposed to examine the efficacy of PTEE in ameliorating ISO-induced MI in adult rats.
MI is characterized by extensive oxidative stress and inflammatory injury, which contribute to cardiomyocyte apoptosis, fibrosis, and ventricular remodeling (Frangogiannis, 2014). Among the key molecular regulators, the NF-κB signaling pathway plays a central role in orchestrating the balance between oxidative damage and cellular defense mechanisms. Activation of NF-κB, a redox-sensitive transcription factor, stimulates several pro-inflammatory cytokines, including TNF-α, IL-1β, and IL-6—mediators known to exacerbate myocardial inflammation and necrosis (Kawano et al., 2006; Lingappan, 2018). Elevated levels of these cytokines have been correlated with infarct size, impaired ventricular function, and poor post-infarction recovery (Mann, 2015). TNF-α promotes cardiomyocyte apoptosis and contractile dysfunction by activating caspase pathways and reducing calcium handling (Haudek et al., 2007). Similarly, IL-1β amplifies inflammatory cell recruitment and matrix degradation, worsening tissue injury (Del Buono et al., 2024), while IL-6 modulates acute-phase responses and induces myocardial hypertrophy through Janus Kinase/Signal Transducer and Activator of Transcription (JAK/STAT) signaling (Fontes et al., 2015). Together, these cytokines perpetuate the inflammatory cascade and contribute to adverse ventricular remodeling after MI.
In the present study, PTEE significantly attenuated the inflammatory response by downregulating NF-κB expression and reducing TNF-α, IL-1β, and IL-6 levels in ISO-triggered MI rats. This reduction suggests that PTEE suppresses cytokine-mediated myocardial inflammation, possibly through inhibition of NF-κB nuclear translocation. Concurrently, PTEE enhanced HO-1 expression and normalized NQO-1 activity, indicating activation of cytoprotective antioxidant pathways that mitigate oxidative stress-induced injury. The observed modulation of these signaling molecules implies that PTEE exerts dual anti-inflammatory and antioxidant actions, promoting myocardial protection.
The HO-1/NQO-1 axis, under the regulation of the nuclear factor erythroid 2-related factor 2 (Nrf2) pathway, is known to suppress NF-κB activity by attenuating ROS and limiting cytokine gene transcription (Durante, 2003; Saha et al., 2020). Thus, the simultaneous upregulation of HO-1 and restoration of NQO-1 expression in PTEE-treated rats may account for the reduction in inflammatory cytokines. Our data are consistent with earlier reports that phytochemicals with antioxidant properties reduce myocardial injury by inhibiting NF-κB signaling and cytokine release (Chen et al., 2022; Mi et al., 2023).
Oxidative stress and ionic imbalance further exacerbate MI-induced injury through the depletion of endogenous antioxidants and mitochondrial dysfunction (Dhalla et al., 2000; Xiang et al., 2021). Additionally, ischemic adenosine triphosphate (ATP) depletion alters Na⁺, K⁺, and Ca²⁺ homeostasis, leading to intracellular calcium overload and subsequent necrosis (Garcia-Dorado et al., 2012). PTEE treatment effectively restored antioxidant enzyme levels and normalized ionic balance, thereby maintaining myocardial membrane integrity and improving functional recovery.
In the present study, administration of PTEE effectively restored serum TP levels while reducing CRP and UA concentrations in ISO-triggered MI rats. CRP and UA elevation in MI reflects heightened systemic inflammation, oxidative stress, and endothelial dysfunction, which exacerbate myocardial injury (Ridker et al., 2002; Saito et al., 2021). PTEE treatment significantly attenuated these alterations, indicating its potent antioxidant and anti-inflammatory activity. Restoration of TP levels further suggests improved myocardial integrity and metabolic stability. These findings support the cardioprotective potential of PTEE through modulation of inflammatory and oxidative biomarkers associated with MI. Collectively, these findings suggest that PTEE confers cardioprotection by modulating both inflammatory and antioxidant pathways while stabilizing ionic homeostasis. This integrated mechanism highlights the therapeutic potential of P. tenuifolia in mitigating oxidative and inflammatory injury during MI.
Apart from these key findings, the present study has several limitations. The lack of histopathological confirmation limits comprehensive assessment of structural changes. Functional cardiac parameters (e.g., echocardiography) were not evaluated, restricting insights into hemodynamic effects. Standardization issues with P. tenuifolia extract may affect reproducibility. The short-term design captures only acute effects, missing potential chronic benefits or adverse effects. Findings are specific to an ISO-induced MI model in rats, limiting generalizability. Long-term safety and efficacy data are lacking. Future studies should address these gaps. These limitations will definitely be addressed in our future studies to further elucidate P. tenuifolia’s cardioprotective potential.
Conclusion
PTEE exerts significant cardioprotective effects against ISO-induced MI through modulation of key oxidative and inflammatory pathways. PTEE effectively suppressed the NF-κB-mediated inflammatory cascade, causing pro-inflammatory cytokines reduction, while concurrently enhancing the antioxidant defense via upregulation of HO-1 and normalization of NQO-1 activity. The restoration of antioxidant enzymes (SOD, CAT, and GSH) and correction of ionic disturbances (Na⁺, K⁺, and Ca²⁺) further emphasize its role in maintaining myocardial structural and functional stability. Moreover, the reduction in serum CRP and UA levels, along with the restoration of TP, underscores the anti-inflammatory and cytoprotective properties of PTEE. Collectively, these results suggest that P. tenuifolia holds strong therapeutic potential as a natural cardioprotective agent by targeting oxidative stress, inflammation, and ionic imbalance. However, further molecular and clinical investigations are warranted to validate its efficacy and establish its translational relevance in cardiovascular therapeutics.
Summary
MI predominantly arises from the rupture or erosion of atherosclerotic plaques, leading to thrombotic occlusion and impaired coronary blood flow. Phytochemicals have emerged as promising therapeutic agents for MI due to their diverse mechanisms. In this work, PTEE exerts significant cardioprotective effects against isoproterenol-induced MI through modulation of key oxidative and inflammatory pathways. Collectively, the present results suggest that PTEE holds strong therapeutic potential as a natural cardioprotective agent, which warrants further studies in the future.
Footnotes
Abbreviations
CAT: Catalase; CRP: C-reactive protein; GSH: Reduced glutathione; ISO: Isoproterenol; MI: Myocardial infarction; PTEE: Ethanolic extract of Polygala tenuifolia; SOD: Superoxide dismutase; TP: Total protein; UA: Uric acid.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This work was approved by the institutional ethical committee of Shangluo Traditional Chinese Medicine Hospital, Shangluo City, Shaanxi Province 726000, China.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
NA.