
Abstract
Type 2 diabetes mellitus is the leading cause of diabetes complications in China, threatening people’s health and quality of life seriously. Over the past few years, with the change in lifestyle and dietary habits, the course of diabetes mellitus is gradually prolonged, and complications in diabetic patients are becoming increasingly common, so scholars have studied the syndrome associated with this disease, which has led to certain research findings. The purpose of this article is to summarise the research progress of diabetes mellitus, diabetic nephropathy, diabetic retinopathy, diabetes mellitus with heart disease, diabetic peripheral neuropathy, and other chronic complications of diabetes mellitus from two aspects of literature and clinical research, present directions and strategies for standardising syndrome types of diabetes mellitus and its common chronic complications.
Introduction
Diabetes mellitus (DM) is a metabolic disease characterised by hyperglycaemia, and Type 2 diabetes mellitus (T2DM) is the most prevalent form of diabetes in China. In recent years, the incidence of DM has continued to rise in China. According to the latest data released by the Chinese Guidelines for the Prevention and Control of T2DM, the prevalence of T2DM among adults over 18 years of age has reached 10.4%. Additionally, the total number of diabetic patients in China is the highest in the world (Chen, 2019). DM can lead to multi-system damage, including functional decline and failure of tissues and organs such as the kidneys, eyes, nerves, heart, and blood vessels (Ge & Xu, 2014; Jia & Lu, 2018). These chronic complications result from macrovascular, microvascular, and peripheral neuropathy caused by factors such as elevated blood glucose. Diabetic complications are not easily diagnosed in the early stages and have a significant impact on the quality of life of patients. The middle and late stages of chronic complications are often accompanied by high treatment costs, which can impose a financial burden on patients and their families (Pang et al., 2020). However, clinical practice has shown that Traditional Chinese Medicine (TCM) can delay the onset and progression of DM and its chronic complications to some extent (Sloan et al., 2021; Tian et al., 2019). This finding is deserving of further investigation. DM belongs to the categories of ‘Pi Dan’ and ‘wasting thirst disorder’ in Traditional Chinese Medicine. The treatment of DM in TCM has a history of more than a thousand years. It is believed that the disease is mainly caused by physical factors, dietary abnormalities, emotional and mental disorders, old age and physical deterioration, fatigue and exhaustion, exposure to external pathogens, and adverse effects of medications. In Huangdi’s Internal Classic, there is a discussion on the ‘wasting thirst disorder’ which describes its aetiology and pathogenesis. It includes factors such as ‘eating greasy food’, ‘when a person is angry the body’s qi will travel up ...... eventually leading to poor blood flow’, and ‘The five zang-organs are fragile’ ‘stagnancy of two Yang-ming meridians’. Effective management of diabetes by TCM is based on accurately diagnosing the TCM syndrome. The TCM syndrome is a proprietary concept in TCM theory that refers to the generalisation of symptoms, signs, and pathology of the organism at a certain stage of disease development. Since the study of the classification of TCM syndromes of DM and its complications in China can help standardise the TCM diagnosis and evaluate the efficacy of the disease, it has received increasing attention from researchers in recent years. However, the diagnostic criteria for this disease have not yet been widely recognised, and there are few reviews on the classification of this disease.
Therefore, we reviewed TCM syndromes studies on Chinese medicine for DM and its common chronic complications, including diabetic nephropathy (DN), diabetic retinopathy (DR), diabetic heart disease, and diabetic peripheral neuropathy (DPN), conducted in China over the past 25 years. We also suggested future research directions for syndrome-based diagnostic criteria for DM and its chronic complications.
Syndrome
Study on the Syndrome Types of DM
Ancient medical practitioners divided diabetes into on the fire, in the fire and under the fire. For the three types of diabetes in TCM, they also performed syndrome differentiation and treatment. Currently, with the change in people’s diet and lifestyle, the duration of diabetes is gradually prolonged, and chronic complications of DM are becoming more prevalent. Nowadays, clinical treatment cannot be based solely on the identification of the three types of diabetes in TCM alone, therefore, scholars have conducted studies on the syndrome types of diabetes.
Zhao et al. (2012) analysed the literature on the treatment of DM from 1994 to 2011 and found that in DM treated with Chinese medicine, the syndrome types of diabetes that appeared more frequently were blood stasis syndrome, syndrome of both qi and yin deficiency, syndrome of yin deficiency and dry heat, kidney yin deficiency syndrome, spleen qi deficiency syndrome, deficiency of both yin and yang syndrome, kidney qi deficiency syndrome, syndrome of yin deficiency and effulgent fire, and phlegm-dampness syndrome; in DM treated with combined Chinese and Western medicine, the pattern of syndrome that more frequent occurrence was blood stasis syndrome, syndrome of both yin and yang deficiency, syndrome of yin deficiency, and dry heat, deficiency of both yin and yang syndrome, qi deficiency, deficiency of both spleen and kidney syndrome, and phlegm-dampness syndrome. Accordingly, blood stasis syndrome, syndrome of both qi and yin deficiency, syndrome of yin deficiency and dry heat are considered to be the main syndrome types of DM. Gong et al. (2015) analysed the four diagnostic information of patients with this disease by clustering and classified the syndrome types of this disease into the spleen-kidney qi deficiency syndrome, liver-kidney yin deficiency syndrome, yin deficiency with heat exuberance syndrome, syndrome of both qi and yin deficiency with Phlegm Dampness, syndrome of yang deficiency with blood stasis, among these syndromes, spleen-kidney qi deficiency syndrome dominated. Based on an analysis of 2826 diabetic patients’ syndrome types, Xing et al. (2021) found that qi deficiency, blood stasis, yin deficiency, and yang deficiency were the most prevalent syndrome types. According to Hu et al. (2019), 18,535 hospital records of diabetic patients were analysed and found that patients aged 20–60 years were predominantly affected by yin deficiency with heat exuberance syndrome, whereas patients aged 60–80 years were predominantly affected by the syndrome of both qi and yin deficiency.
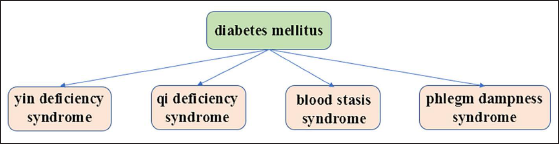
Based on research, DM is mostly associated with yin deficiency, qi deficiency, blood stasis, and phlegm dampness syndrome, which is consistent with its pathogenesis (Figure 1). According to Chinese internal medicine (Chen, 2004), the pathogenesis of diabetes is mainly based on the theory that yin deficiency is the root, dryness and heat as the manifestation. Meanwhile, qi deficiency of both lungs and spleen is still the key factor, and another significant point is that when there is spleen qi deficiency, qi deficiency much more easily leads to phlegm and dampness. Similarly, blood stasis plays an important role in DM pathogenesis. Due to age and prolongation of the disease, the severity of the disease increases, evolving from a single syndrome element (yin deficiency) to two syndrome elements (qi and yin deficiency).
The Main TCM Syndromes of DM.
Study on the Syndrome Types of DN
DN is one of the microvascular comorbidities of DM and a major cause of DN and end-stage renal disease in China (Wang & Wang, 2021). Based on estimates, The risk of diabetes-related kidney disease increases by 25%–40% between 20 and 25 years after diagnosis (Xu et al., 2013), and the prevalence of this disease increases as the years pass (Fan et al., 2013). Zheng et al. (2019) analysed 278 articles pertaining to DN using statistical methods and found that the disease is most commonly associated with qi and yin deficiency syndrome, explaining the pathogenesis of DN. Further research found that blood stasis syndrome was predominant in the marked real syndrome, followed by dampness heat, water dampness, phlegm turbidity and so on, and deficiency of both the spleen and kidney was regarded as critical factors in the development of the disease. Qi et al. (2012) searched and analysed the literature related to DN from 2003 to 2012 and found that syndrome of both qi and yin deficiency, spleen-kidney qi deficiency syndrome, yang deficiency of both spleen and kidney syndrome and deficiency of both yin and yang syndrome were main types of the syndrome of deficiency in origins, and blood stasis was the most important type of excess in superficiality syndrome. It can be seen that DN is mostly characterised by the syndrome of both qi and yin deficiency and blood stasis is the main syndrome of the excess in superficiality syndrome.
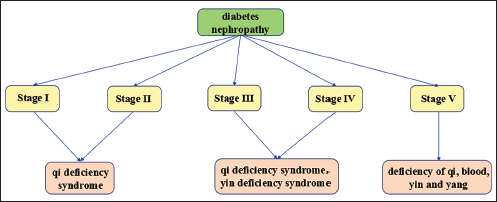
According to the Mogensen staging method, DN was divided into stages I–V (Mogensen et al., 1983). Song et al. (2019) applied a cross-sectional, retrospective survey study to 273 cases and found that stages I–II of DN were dominated by syndrome of yin deficiency and dry heat, stage III was dominated by the syndrome of both qi and yin deficiency, and stages IV and V were dominated by spleen-kidney qi deficiency syndrome, and the study showed that with the progression of the disease, the main syndrome trend of DN was a syndrome of yin deficiency and dry heat ↓ syndrome of both qi and yin deficiency ↓ spleen-kidney qi deficiency syndrome. The study also found that the syndrome of excess in superficiality syndrome was dominated by blood stasis syndrome throughout the disease. Along with blood stasis syndrome, dampness-heat syndrome predominated in the early stages of DN, but as the disease progressed, cold-dampness syndrome and phlegm-turbidity syndrome gradually increased. A review of the literature on DN by Cai et al. (2018) revealed that the early stage of the disease was characterised by qi deficiency syndrome and yin deficiency syndrome, whereas the late stage was characterised by qi deficiency syndrome, yang deficiency syndrome, and dampness-turbidity syndrome. Huang (2017) found that patients with early DN had predominantly syndrome of both qi and yin deficiency and liver-kidney yin deficiency syndrome. In the same study on the syndrome patterns of patients with early DN, Yang et al. (2017) found that patients with early DN were dominated by qi deficiency, yang deficiency, and syndrome of yang deficiency and water diffusion. As shown in the above studies, there are slight differences in opinions regarding the early syndrome patterns of DN, but they all agree that qi deficiency syndrome is one of the main syndrome types of the disease. In 268 DN patients with stage III, Zhang et al. (2019) measured the frequency of syndrome types and found that the syndrome patterns of the disease were mainly yin deficiency with heat exuberance syndrome, spleen-kidney qi deficiency syndrome, syndrome of both qi and yin deficiency, syndrome of dampness-heat accumulation in spleen, and syndrome of blood stasis in channel and collateral. Liu (2016) used principal component analysis and cluster analysis to summarise the syndrome types collected from DN patients and found that the disease was dominated by qi deficiency syndrome and yin deficiency syndrome in the early stage, while the later stage showed qi deficiency syndrome, yang deficiency syndrome, and phlegm-dampness syndrome, and blood stasis syndrome and phlegm-dampness syndrome existed in all stages. A similar conclusion was reached by Li et al. (2019) that stage III patients had mainly syndrome of both qi and yin deficiency, and stage V patients gradually developed into deficiency of qi, blood, yin, and yang with both phlegm-dampness syndrome and blood stasis syndrome.
In the above studies, scholars considered qi-yin deficiency syndrome as the main syndrome type of the disease, but in the study of early syndrome types of DN, there are slightly different perspectives, some scholars considered syndrome of both qi and yin deficiency and liver-kidney yin deficiency syndrome as the main syndrome types of the disease in the early stage, while other scholars considered qi deficiency syndrome, yang deficiency syndrome, and syndrome of yang deficiency and water diffusion as the main syndrome types of the disease in the early stage. The former study is based on the syndrome types of the disease, while the latter is based on the syndrome elements, but both believe that qi deficiency is one of the main syndrome types in the early stage of the disease, we believe that qi can promote fluid, when there is a qi deficiency there is no way to produce fluid, which leads to deficiency of both qi and yin. At the same time, the aggravation of qi deficiency can lead to the occurrence of Yang deficiency. The study involved the middle and late stages of DN, the scholars maintain a unified perspective that the syndrome of yin deficiency and qi deficiency predominate in stage III and IV patients, while the deficiency of qi, blood, yin and yang predominate in stage V patients. As DN progresses, the patient’s syndrome changes from simple qi deficiency to qi deficiency and yin deficiency, and then to qi deficiency, blood deficiency, yin deficiency and yang deficiency, reflecting the complexity of the disease’s developmental change (Figure 2).
The Main TCM Syndromes of DN.
Study on the Syndrome Types of DR
DR is one of the most common and major microvascular complications of DM. Five to nine years after the onset of diabetes, 10% of diabetic patients develop DR, about 50% of patients develop DR within 15 years of onset, whereas 80%–90% develop it within 25 years (Li, 2005).
A literature search by Zhao et al. (2017) revealed that DR patients were predominantly deficient in qi and yin. Wang et al. (2017) found that the frequency of syndrome elements in the DR group was, in descending order, qi deficiency, yin deficiency, blood deficiency, yang deficiency, blood stasis, deep heat, phlegm turbidity, qi stagnation, and dampness heat. Jiao et al. (2017) found that the syndrome of qi deficiency syndrome, dry heat syndrome, blood stasis syndrome, liver deficiency syndrome, and yin deficiency syndrome appeared more frequently in DR patients, with the qi deficiency syndrome accompanying the entire course of DR disease, the liver deficiency syndrome having a greater severe in the middle and late stages, and yin deficiency syndrome is more severe in the late stages. Cao et al. (2017) used factor analysis to extract DR syndrome elements and found that yin deficiency, qi deficiency, blood stasis, and yang deficiency were the main syndrome elements in DR patients.
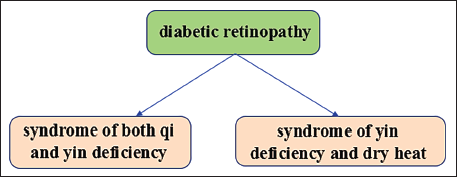
In the study of Chinese medical syndrome elements of DR, scholars mostly considered the syndrome of both qi and yin deficiency and the syndrome of yin deficiency and dry heat as the main syndrome elements of the disease. The syndrome elements are mostly focused on qi deficiency, yin deficiency, yang deficiency, and blood stasis. When people suffer from a deficiency of both qi and yin, their qi and blood cannot reach the orbits and eyes, the eyes are deprived of water and nutrient supply, which leads to the development of retinal lesions. As Dai Yuan Li said in 〈〈Secrets of Syndrome and Treatment〉〉 contains: If the patient has long-term three types of diabetes, the body will lack essential qi and blood, some people will have symptoms of blindness in the eyes, and some will have symptoms similar to stroke such as hemiplegia in the hands and feet, but this symptom is more likely to occur in patients with kidney consumption (Figure 3).
The Main TCM Syndromes of DR.
Study on the Syndrome Types of DM Combined with Coronary Heart Disease
DM and coronary heart disease are two common diseases that seriously endanger human health. Patients with poor glycaemic control can develop lipid metabolism disorders and hyperlipidaemia, which can complicate coronary heart disease (Li et al., 2014). The results of relevant surveys indicate that the incidence of coronary heart disease in diabetic patients is higher than in non-diabetic patients (Lu, 2011). More than 50% of deaths in diabetic patients are related to diabetic cardiovascular complications (Wang et al., 2019), which have a serious impact on people’s survival.
Zhu et al. (2019) analysed the literature related to DM combined with coronary heart disease between 1998 and 2018. It was found that the deficiency of the disease was dominated by qi-yin deficiency, and the syndrome type of the disease was dominated by phlegm, stasis, dampness, and heat. In the distribution of syndrome elements of diabetic coronary heart disease, the frequency of occurrence, in descending order, was qi deficiency, yin deficiency, stasis, phlegm, dampness, yang deficiency, and heat. In addition to these traditional syndrome elements including qi deficiency, yin deficiency, phlegm, and stasis, two other syndrome elements damp and heat are believed to play a significant role in the pathogenesis of the disease.
Based on a current survey method, researchers (Yu, 2016; Zhang, 2016) analysed the syndrome elements in patients with DM and coronary heart disease and then concluded that the disease was characterised by qi deficiency, phlegm, and blood stasis. Yang (2017) analysed patients with DM combined with coronary heart disease using the factor analysis method and found that the main syndrome elements of the disease were yin deficiency, qi deficiency, and blood stasis.
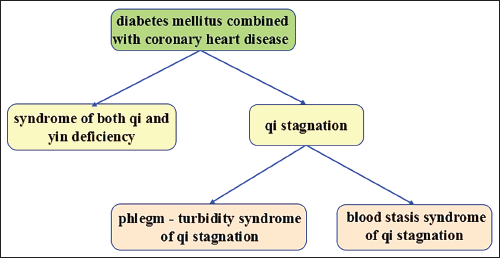
Studies of DM coupled with coronary heart disease most often highlight the syndrome of both qi and yin deficiency as one of the main causes of the disease. Furthermore, other scholars consider the syndrome type of phlegm turbidity syndrome and blood stasis syndrome in light of qi stagnation as the basic types of the disease. Nevertheless, among the studies on the syndrome of DM combined with heart disease, scholars tend to study the syndrome of combined coronary heart disease. However, very few studies have been conducted on DM and other heart diseases, including microvascular cardiomyopathy, cardiac arrhythmias, and cardiac insufficiency due to cardiac autonomic dysfunction. In the future, further study should be centred on diabetes combined with other types of heart disease, so that the study of diabetes combined with heart disease can be more comprehensive (Figure 4).
The Main TCM Syndromes of DM Combined with Coronary Heart Disease.
Study on the Syndrome Types of Other Chronic Complications of DM
DPN accounts for the majority of chronic clinical complications of DM, with a prevalence of 60%–70% (Xiang, 2003), about 10% of diabetic patients already have been involved in peripheral nerve damage at the time of initial diagnosis (Qi & Yu, 2015). The disease is insidious and further development can lead to infection and increase the risk of non-traumatic amputation in patients (Cheng & Yuan, 2021).
A study by Shi and Wang (2019) investigated the distribution pattern of DPN patients using epidemiological survey methods and found that the disease was dominated by qi deficiency and blood stasis syndrome, deficiency of qi and yin with blood stasis syndrome, yin deficiency and blood stasis syndrome, liver-kidney yin deficiency syndrome, yang deficiency and blood stasis syndrome, phlegm and blood stasis syndrome, damp-heat blocking collaterals syndrome, among which patients with disease duration of fewer than five years were dominated by excess syndromes such as phlegm and blood stasis syndrome and damp-heat blocking collateral syndrome. However, patients with a disease duration of more than five years were dominated by deficiency of qi and yin with blood stasis syndrome, yin deficiency and blood stasis syndrome, and yang deficiency and blood stasis syndrome which belong to deficiency complicated with excessiveness syndromes. As can be seen, blood stasis is present throughout the entire course of DPN. In a study of DPN patterns, Shi et al. (2016) found that the pattern of development of this disease pattern is the evolution of qi-yin deficiency ↓phlegm and blood stasis blocking collaterals ↓yang deficiency and cold coagulation. Based on this, scholars mostly believe that phlegm blended with blood stasis and qi-yin deficiency are two reasons of the disease. Because deficiency of both qi and yin leads to poor production and movement of qi and blood, resulting in phlegm and blood stasis. It should be noted, however, that there is no consensus on the pattern of evolution of this disease.
From the above studies, it is clear that the syndrome of both qi and yin deficiency is more common in DR, diabetic heart disease, and DPN.
Though qi-yin deficiency syndrome is an important syndrome type of diabetes and its chronic complications their pathogenesis is different. For example, in DR, the pathogenesis of syndrome of both qi and yin deficiency is that when the patient suffers from thirst for a long time, which causes the body to lose body fluid and blood, and then causes the eyes to lose the nutrition supply of qi and blood, leading to the occurrence of diseases. The pathogenesis of DM with heart disease is that when there is a syndrome of yin deficiency and dry heat, the body will evaporate body fluid and cause poor blood flow, thus forming blood stasis in the body. Also, when the patient suffers from dry heat for a long time, it will deplete the qi and yin. This leads to qi deficiency and the blood flow is weak, and then blood stasis will occur, and the blood stasis will stay in the veins. Both of these conditions can lead to disease. The pathogenesis of DPN is that when a person suffers from dry heat, the yin fluid evaporates in the body, causing the movement of blood in the meridians to be blocked, leading to the disease.
Study on the Syndrome of Other Chronic Comorbidities of DM
In addition to the above studies on common diabetic comorbidities, it is often noted that there are relatively few studies that have been done on other types of chronic comorbidities associated with diabetes, mainly focusing on studies such as the diabetic foot. Fang et al. (2010) analysed the literature on diabetic autonomic neuropathy and found that the disease was mainly characterised by qi and yin deficiency, blood stasis syndrome, deficiency of both spleen and kidney syndrome, and spleen and stomach weakness syndrome.
The results of a study conducted by Sun et al. (2016) on patients with diabetic feet showed that the syndrome elements of the disease were common in blood stasis, dampness heat, yin deficiency, and qi deficiency, with a combination of excess syndrome deficiency syndrome.
Clinical identification of diabetic foot in Chinese medicine is broadly divided into the following four categories. The first category is based entirely on the identification criteria of authoritative literature. For example, Liao (2017), identified diabetic foot as cold and damp obstruction, blood stasis, damp-heat toxicity, heat toxicity injury to yin, and deficiency of qi and blood. Qin (2011), identified diabetic foot as a yin-cold type, blood stasis, damp-heat injection, heat toxicity blazing, and spleen-kidney yang deficiency, which is completely in line with Practical Integrative Surgery of Traditional Chinese and Western Medicines and Integrative Medicine of Peripheral Vascular Diseases. The second category involves making appropriate changes based on the identification of authoritative literature, such as Wei et al. (2011) identified diabetic foot of Yang deficiency and cold coagulation based on the authoritative literature on Yang deficiency and blood coagulation, and yin and cold evidence. The third category involves deviating from authoritative literature and developing their own identification, such as Liu et al. (2019) who identified diabetic foot into three types of evidence: stomach heat blazing, evidence of lung heat and fluid injury evidence, and kidney yin deficiency evidence. The fourth type is to combine two syndromes into one. For example, Y. Zhang et al. (2015) classified diabetic foot into four types of syndromes: yin deficiency, dry heat, venous stasis and obstruction; toxic heat, venous stasis, and obstruction; damp heat, venous stasis, and obstruction; and qi and blood deficiency, and venous stasis and obstruction; and C. Zhang et al. (2015) identified diabetic foot into four types of syndromes: damp heat and toxicity, and tendon rot and meat decay; heat and toxicity, and stasis and obstruction; qi and blood deficiency, and venous stasis, and obstruction; liver and kidney yin deficiency, and venous deficiency, and venous stasis, and obstruction. The five types of diabetic foot are Yin deficiency of the liver and kidney, stasis and obstruction of veins and collaterals, Yang deficiency of the spleen and kidney, phlegm and stasis obstruction of collaterals and collaterals. These four conditions together have collectively caused confusion within the academic community regarding the identification of diabetic feet in Chinese medicine.
In a questionnaire survey, Xu and Wu (2012) collected clinical and evidential features of 200 patients with T2DM combined with hypertension and found that patients with T2DM were predominantly characterised by qi deficiency syndrome and kidney essence deficiency syndrome.
Conclusion
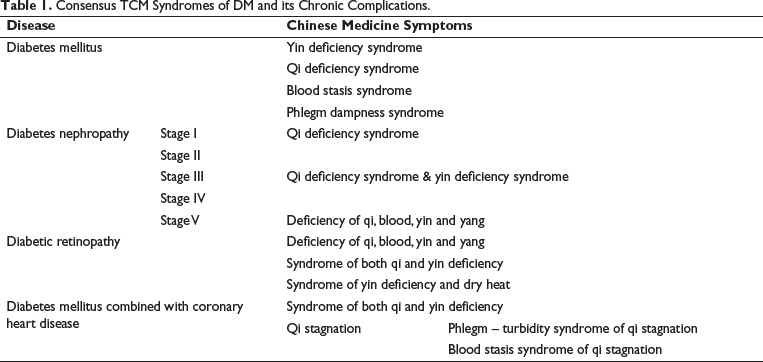
This article summarises the research results of various researchers on the classification of syndrome categories for Chinese medicine in the treatment of DM and its common chronic complications in China over the past 25 years. It reveals that there is a consensus among different studies regarding some of the syndrome categories for Chinese medicine in the four diseases of DM, diabetes nephropathy, DR and DM combined with coronary heart disease (Table 1). However, there are still some issues that researchers need to further explore. First, the naming of TCM patterns for DM and its common chronic complications is not consistent. In addition, researchers hold different views on the distribution characteristics of early DN patterns. The aforementioned issues partially restrict the effectiveness of TCM in treating and preventing diabetes and its long-term complications. In addition, in the evidence-based studies on DM combined with heart disease, there are fewer studies on other DM combined with heart disease, except for those on coronary heart disease. Future studies should focus on strengthening and standardising the nomenclature of DM and its common chronic complications, in order to facilitate the development of criteria for clinical diagnosis and efficacy evaluation of DM and its chronic complications. Not only that, but the sample size should be expanded, and a multicentre clinical study should be conducted to explore the chronic complications of diabetes that have been the subject of differing opinions and insufficient research. On this basis, criteria should be developed for the clinical diagnosis and evaluation of the efficacy of diabetes and its chronic complications.
Consensus TCM Syndromes of DM and its Chronic Complications.
Abbreviations
TCM: Traditional Chinese Medicine; DM: Diabetes mellitus; T2DM: Type 2 diabetes mellitus; DN: Diabetic nephropathy; DR: Diabetic retinopathy; DPN: Diabetic peripheral neuropathy.
Authors’ Contributions
Yiming Hao was responsible for the study and revised the manuscript. Zhiyuan You, Junhong Lu, and Yifeng Xu wrote the manuscript. Yiqin Wang helped in the ideas of study. Zhiyuan You and Junhong Lu share the first authorship.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This study was supported by the Construction Project of Academic Experience Research Studio for Famous Elderly Traditional Chinese Medicine Experts of Shanghai Municipal Health Commission (SHGZS-202201), Scientific Research Project of Shanghai Municipal Commission of Health and Family Planning (No. 20164Y0279), Shanghai Science and Technology Planning Program (No. 21DZ2271000), and Shanghai Education Commission Program (No. 2021 Science and Technology Program (No. 2021 Science and Technology 02-37).