
Abstract
Background
Infection Prevention and Control (IPC) processes are associated with inherent changes in the general operations of hospitals as they directly modify the clinical outcomes, effective functioning and the internal image of any healthcare setting. Positive IPC is essential to the safety of patients and reliability of the institution. Insight into the perceptions of IPC practice by the hospital staff is a vital element to enhance practising procedures and optimise practice-related measures.
Purpose
The purpose of the study was to evaluate the perception and practicability of the IPC between the members of staff working in the hospital in different clinical and non-clinical departments. In particular, the study aimed at defining the impact of such practices on the efficiency and internal reputability of the hospital.
Methods
A questionnaire was designed to be given to the members of staff at the hospital, a research of Linking Infection Prevention Control to Hospital Efficiency and Reputation in several departments, both clinical and non-clinical. The collected data involved staff perceptions about IPC practices, factors that impede proper implementation and infection high-risk areas. The answers were compared in a logical manner to discover a shared theme and possible missing links in the modern IPC strategies.
Results
Current IPC measures negatively influenced hospital efficiency and the internal reputation, as established by the analysis. Employees have pointed out the great variance in the practice levels of IPC compliance between the departments, and that intervention in this may be required to complement training with targeted solutions, especially where there is the greatest risk. The research reported that persistency in training and education enhanced compliance as well as awareness among the health workers.
Conclusion
Findings support the need to make hospitals focus on high-risk processes and ensure implementation of IPC practices by reinforcing it with specific training sessions. Educational programs have the prospect to significantly increase efficiency and internal image of the hospital because they may influence staff members and their perspective on it. The need to study the most appropriate sample size and the contribution of cutting-edge technologies in enhancing IPC further should also be answered in subsequent research.
Keywords
Introduction
This article outlines the Salient issue of Healthcare-Associated Infections (HAIs) and the need to have effective Infection Prevention and Control (IPC) efforts in Indian hospitals. HAIs have significant impacts over patient outcomes, the efficiency of the hospital and the internal reputation of the healthcare organisations. The article defines the concept of IPC as outlined by the World Health Organisation (WHO) with a special focus on how it can help to reduce unnecessary and potentially hazardous infections among patients as well as the medical staff. The hierarchy of controls developed by the National Institute for Occupational Safety and Health (NIOSH) can be used as the basic system of the assessment, and its implementation is the IPC that comprises elimination, substitution, engineering controls, administrative controls, environmental controls and the Personal Protective Equipment (PPE). The reason why inadequate IPC translates to operational inefficiencies, increased workload, employee burnout and ultimately results in the degradation of the internal reputation of the hospital has also been discussed by the article. The study will explore how IPC practices can affect hospital efficiency and internal reputation to fill gaps in the literature, since the mediating effect of hospital efficiency has rarely been studied. The need to carry out the research is reasoned with intellectual, social and practical reasons. The article ends with a set of study questions, aims and a conceptual framework that links the IPC measurements, efficiency and an internal reputation of a hospital to each other in a way that it builds a ground to conduct the empirical research and offer strategic implications to enhance the quality of healthcare delivery in India.
Conceptual Model
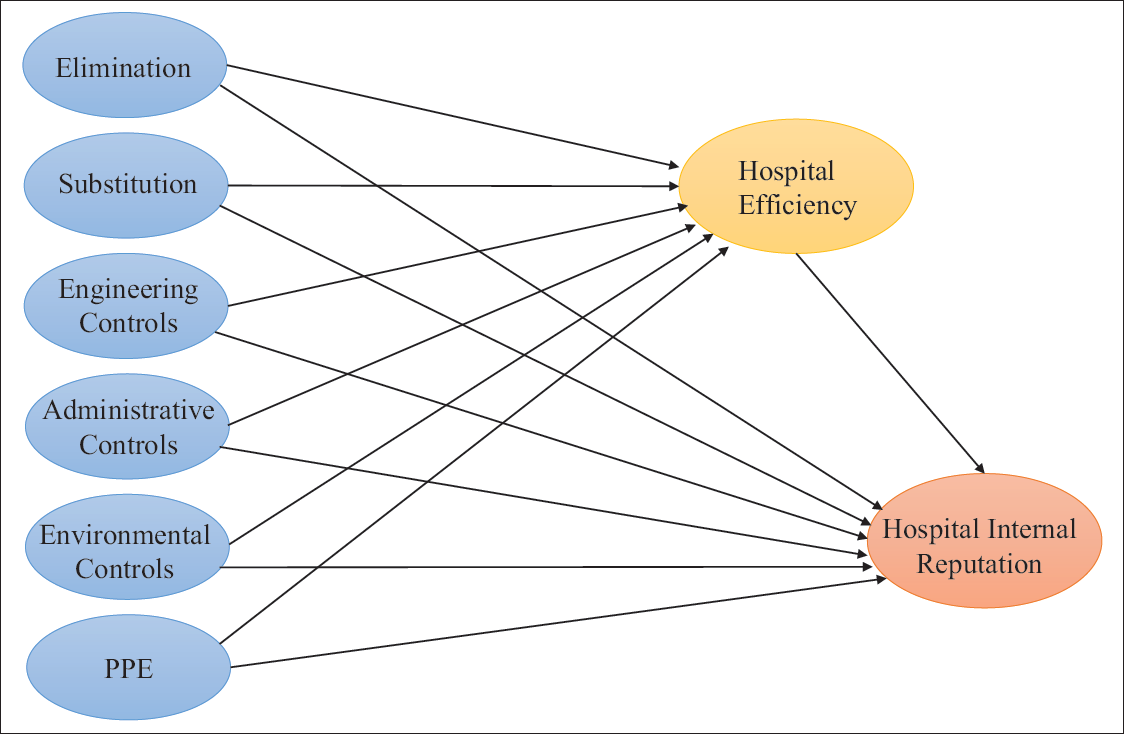
IPC requires the implementation of various policies and procedures with the main purpose of reducing infection rates, with the focus on bringing down the risk of HAIs. As discussed by Dempsey et al. (2025), 1 Frameworks for Infection Prevention and Control (IPAC) are not foreign to the IPAC community or practitioners, and these guides were extrapolated to align consistently with the hierarchy of controls. This study builds on that foundation to assess their impact on hospital efficiency and internal reputation. As noted by Masuku et al. (2025), 2 IPAC frameworks are well-established among practitioners and have been consistently aligned with the hierarchy of controls—a foundation this study adopts to examine their role in hospital efficiency and reputation. As mentioned by Wang et al. (2025), 3 the competency-based framework for preventing blood-borne exposures in medical students is aligned with the NIOSH hierarchy of controls. This alignment reinforces the relevance of structured IPC frameworks in guiding effective prevention strategies. Numerous programs such as surveillance, isolation, outbreak management, environmental hygiene, employee health, infection prevention policies and education have been identified in this context. According to Jia et al. (2019), 4 HAIs add to the medical cost for the patients by increasing their length of stay at the hospital. Thus, HAIs are not only threatening to the patient’s health and life but also are associated with increased economic burden and economic loss. HAIs result from the incident rate or can be the cause of a lack of proper hygiene and sanitation. Since good sanitisation and high-quality care can lower the incidence of HAIs, Vokes et al. (2018) 5 have emphasised the use of pay-for-performance systems for HAI control. But it is imperative to put in place sufficient actions that can support IPC. Therefore, the application of the hierarchy of controls as guided by Dunn et al. (2015) 6 is the relevant theoretical framework to be integrated for the study of the measures associated with IPC (Figure 1).
Proposed Conceptual Framework.
Methods
Research Design and Approach
In order to investigate the connections between hospital performance outcomes, such as efficiency and internal reputation and IPC measures, this study adopts the correlational research design. For studying naturally occurring phenomena in organisational settings, a correlational design is suitable since it enables the methodical examination of relationships between variables without changing the discussion (Creswell and Creswell, 2017). 7 This design recognises that causality cannot be conclusively established without experimental controls, but it allows for the identification of significant patterns and predictive relationships. As this research primarily aims to evaluate how various IPC strategies affect hospital operations and reputation, a correlational research design remains most appropriate. On the other hand, the deductive theoretical approach is used in this study as being a part of applied research. The methodology begins with the use of already laid theoretical models and tests their relevance using empirical research data, as evidenced by Saunders et al. (2003). 8 The deductive approach is quite effective in hypothesis-driven investigations whose research is guided by previously known theories. This is in opposition to an inductive method of building theory based on observations articulated by Alrajeh et al. (2020). 9 In the present case, the investigation conducts specific hypotheses elaborated through the previous studies of hospital management and IPC effectiveness and uses quantitative data collected through surveys to favour the arguments. Further supporting the selection of a correlational design is the fact that it is frequently employed in healthcare management research, especially when examining the effects of policies and organisational performance, as noted in the findings of Polit and Beck (2008). 10 The study contributes to theoretical discussions regarding the role of IPC in healthcare systems while offering practical insights for hospital administrators by examining the correlations between efficiency and reputation metrics and variables such as engineering controls, administrative controls and staff compliance. However, the results are interpreted with the proper caution regarding causal inferences, acknowledging the limitations of correlational research, such as the inability to control for all confounding variables.
Sampling Design
Sample Size
In a prominent study by Faul et al. (2009), 11 the population is unknown; therefore, the sample size is calculated using G Power software. In G*Power 3, five types of power are available; the study uses a priori analysis explained by Bredenkamp (1969) 12 and Cohen (1988), 13 and the necessary sample size is computed as a function of user-specified values for the required significance level. Drawing on the work by Faul et al. (2009), 11 the sample size determination using G*Power software was also used in the study for greater robustness. With a 5% significance level, assuming normal data distribution and achieving a t-statistic above 1.96, the software indicates a minimum sample size of 218. Nonetheless, a larger sample size is utilised in the study for greater robustness. It indicates that the sample taken in the study is adequate. A total of 658 individuals working at the middle level from different hospitals located near Bhatinda district were contacted through both e-mails and in-person. We received 383 valid responses out of 658, where the response rate was 59.82% from hospitals.
Instrument Design
To pursue the proposed study, conducting a questionnaire-based survey would be most feasible. However, unable to find a standard scale existed to pursue the study, as the research done previously did not test the hierarchy of controls. Therefore, specific themes were identified from the existing literature and studied for the measures. This framed the pathway to develop and define the scale applicable for measuring the operational variables, as explained.
Data Collection Procedure
The data collection process for this study is carefully designed to align with the quantitative, cross-sectional research design and judgmental and snowball sampling approach, ensuring methodological rigour while maintaining ethical standards. Following approval from hospital review boards and related committees, the researcher initiated contact with potential participants through HR-facilitated email distributions that included a detailed participant information sheet. This document outlines the study’s purpose, confidentiality protections, voluntary nature of participation and data handling procedures, serving as implied consent when respondents proceed with the survey. The questionnaire was administered physically using the paper-and-pencil method. To maximise response rates while maintaining data quality, a multi-phase contact strategy was implemented, beginning with an introductory email from HR, followed by two reminder emails/telephonic calls/physical visits to their hospitals at 2-week intervals and concluding with targeted follow-ups if needed to ensure adequate representation across job roles. The survey instrument included attention checks and consistency validators to identify and exclude careless responding. Trained research assistants helped to monitor the data collection process in real-time, addressing queries while carefully documenting all participant interactions and response patterns. Following data collection, a comprehensive quality control protocol was implemented that included checks for duplicate responses, implausible answer patterns and completion times, with problematic cases flagged for review by the principal investigator. The cleaned dataset was then prepared for analysis through a standardised process of variable coding, missing data evaluation and transformation where necessary to meet statistical assumptions. Throughout this process, strict confidentiality was maintained through de-identification procedures, secure data storage on password-protected servers with institutional access controls and a documented audit trail of all data handling decisions.
Statistical and Software Tool Used
The study employs a comprehensive suite of statistical and software tools to ensure rigorous data analysis and robust hypothesis testing. Microsoft Excel served as the primary tool for initial data entry, cleaning and organisation, facilitating the systematic recording of survey responses while identifying and rectifying discrepancies such as missing values, duplicate entries and formatting inconsistencies. This preliminary step is critical for maintaining data integrity before transitioning to advanced statistical analysis. IBM SPSS Statistics was then used for principal component data analysis, enabling the examination of frequency distributions, detection of outliers and assessment of data normality through skewness and kurtosis metrics. Descriptive statistics, including means, standard deviations and ranges, are computed to evaluate central tendencies and dispersion patterns, ensuring the dataset meets the assumptions required for subsequent inferential analyses. To assess the reliability and validity of measurement scales, for confirmatory analysis and hypothesis testing, SmartPLS 3.0 is employed to conduct Partial Least Squares Structural Equation Modelling (PLS-SEM), chosen for its robustness in handling complex models with latent variables, mediating pathways and moderating effects. PLS-SEM is particularly suited for this study due to its flexibility with non-normal data distributions and smaller sample sizes, making it ideal for exploratory research in organisational settings. The software facilitates confirmatory factor analysis to validate the measurement model by examining composite reliability (CR), average variance extracted (AVE), discriminant validity using the Fornell–Larcker criterion and Heterotrait-Monotrait (HTMT) ratio and finally the path analysis and mediation test.
Results
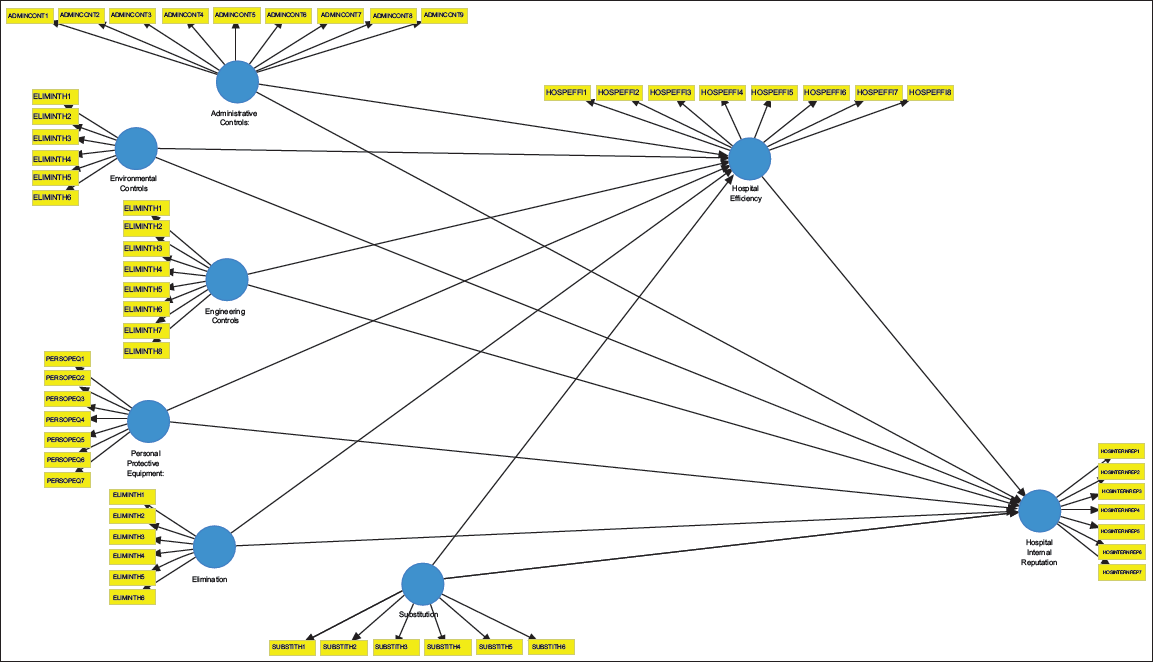
In Figure 2, the Analysis section ensures that the findings are both theoretically significant and methodologically sound by closely examining the research questions using a variety of advanced statistical techniques. By integrating advanced modelling techniques and ensuring the validity and reliability assessments with descriptive and inferential statistics, the study provides a comprehensive and nuanced understanding of the relationships between the primary constructs under investigation.
Proposed Conceptual Path Model: PLS-SEM Visualisation of Constructs.
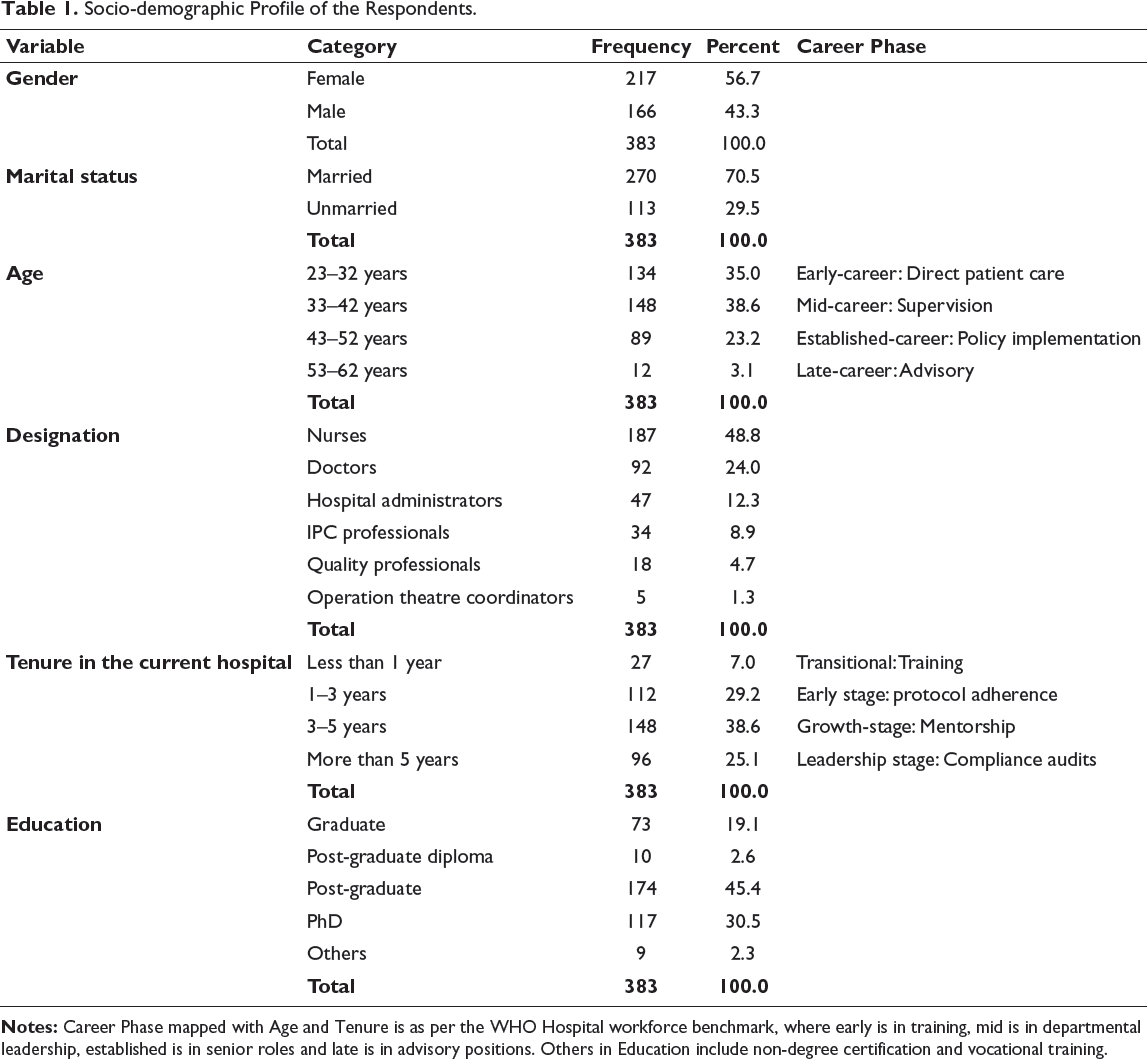
Socio-demographic Profile of the Respondents.
Reliability and Validity Tests
Critical psychometric properties that evaluate the survey items’ ability to measure the intended theoretical constructs in the structural equation model are shown in Table 1. The correlation between each indicator item and its assigned latent construct is represented by the outer loadings. Hair et al. (2019) 14 noted that items effectively representing a construct typically exhibit factor loadings between 0.7 and 0.9. To assess the reliability of a scale—commonly referred to as internal consistency, both Cronbach’s alpha and CR are employed. According to Raykov (1997), 15 Peterson and Kim (2013), 16 and Dunn et al. (2015), 6 Cronbach’s alpha measures the interrelatedness of items within a group, while CR accounts for different item loadings, providing a more precise estimate of reliability. Fornell and Larcker (1981) 17 and Henseler et al. (2015) 18 stated that convergent validity is considered adequate when the AVE exceeds 0.5, indicating that the construct explains more variance in its items than is attributed to measurement error.
Reliability and Validity Test Results.
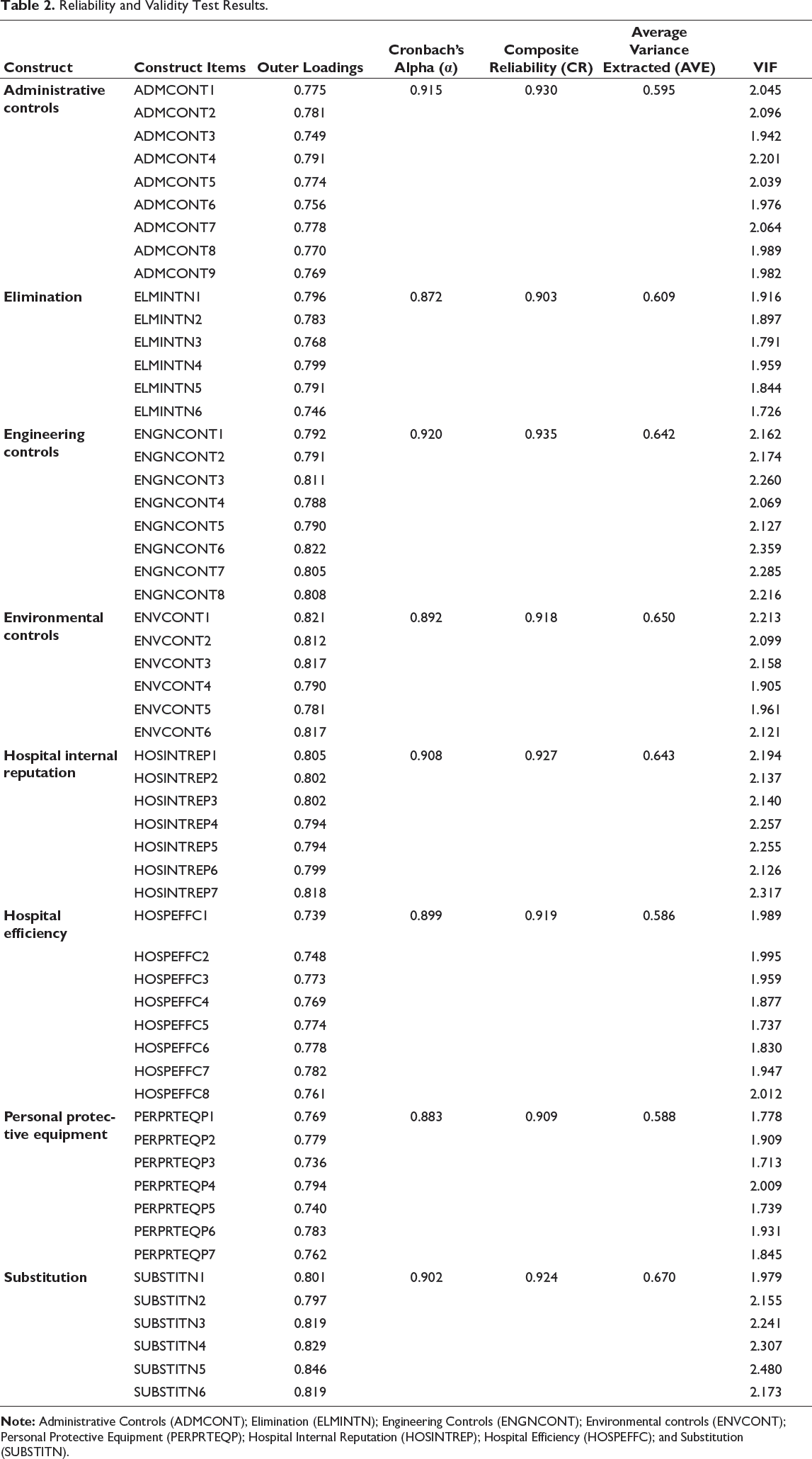
It is interesting to note that all VIF values range between 1.713 and 2.480 and remain significantly below 3.0, suggesting the absence of problematic multicollinearity. Alternative hazard reduction strategies are especially well-measured, as evidenced by the high loadings and reliability metrics for Substitution (SUBSTITN) with loadings 0.795–0.843, and α = 0.902.
In response to these concerns, Henseler et al. (2015) 18 recommended using the HTMT ratio as a more robust approach for assessing discriminant validity.
Heterotrait-Monotrait (HTMT) Ratio.
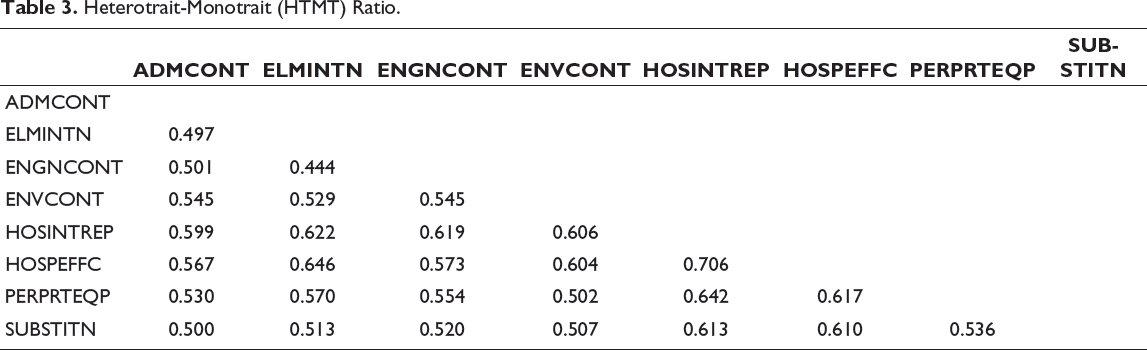
According to Benitez et al. (2019) 19 and Ogbeibu et al. (2018), 20 an HTMT ratio is expected to be below 0.85 in accordance with the accepted instruction on satisfactory discriminant validity. In the study undertaken, the HTMT ratios of the construct ranged between 0.444 and 0.706, and all were lower than the 0.85 mark; thus, the discriminant validity was existent.
Before assessing the structural model, the fit of the model was evaluated, which was carried out through three important parameters, namely the Standardised Root Mean Square Residual (SRMR), the Normed Fit Index (NFI) and the exact fit of a model using statistical inference derived through bootstrapping. As an adaptation of the SRMR, the discrepancy between the actual observed correlation matrix and the correlation (implied) model is a strong metric of an excellent model fit when the values are less than 0.08, as articulated by Hu and Bentler (1999). 21 Henseler et al. (2015) 18 proposed SRMR, as a goodness-of-fit index in partial least squares structural equation modelling (PLS-SEM) to reduce the danger of model misspecification. An incremental fit index is the NFI that compares the chi value of the given model to an alternate meaningful baseline model to measure the fitness, and normally scores above 0.90.
Also, the goodness of fit of the particular model was determined by looking at the statistical inference of the variance between the observed and model-predicted covariance matrices. To this effect, Dijkstra and Henseler (2015a, 2015b) advocated the usage of dULS (squared Euclidean distance) and dG (geodesic distance), wherein a non-significant distinction (p > .05) between model-implied and empirical correlation matrices indicates a good-fitting model.
Model Fit Indices.

For the saturated model, which contains no free paths, fit indices were computed for the measurement model. As presented in Table 4, the SRMR value for the saturated model was 0.043, which is below the recommended threshold of 0.08, indicating a good fit. The NFI value of 0.850, though slightly below the ideal threshold of 0.90, falls within an acceptable range. Furthermore, both d_ULS and d_G values were found to be below the 95% bootstrapped quantile (HI 95% of d_ULS and HI 95% of d_G), providing additional evidence that the data fit the model well. These results collectively support the adequacy of the measurement model.
Estimation of the Path Model
A cutting-edge program for partial least squares structural equation modelling (PLS-SEM), SmartPLS 4, was used to estimate the path model in this study. It is especially well-suited for complex models with non-normal data distributions and smaller sample sizes. PLS-SEM is perfect for exploratory and predictive research because it maximises the explained variance of dependent constructs. Before evaluating the structural model to test proposed relationships between constructs, the measurement model was evaluated to ensure validity and reliability. To ascertain statistical significance, important parameters such as effect sizes (f2), p values, and path coefficients (β) were estimated through a bootstrapping process with 5,000 resamples.
Moreover, the proportion of variance in a dependent (endogenous) construct explicable by its independent (exogenous) constructs in the structural model is expressed as the R-squared (R 2 ) indicator of PLS-SEM. It is in the range 0 to 1, where larger values indicate a higher predictive ability of the model. For example, an R 2 of 0.50 indicates that the predictor constructs (such as infection prevention controls) account for 50% of the variance in the dependent construct (such as hospital efficiency). R 2 values of 0.75, 0.50 and 0.25 are frequently regarded as substantial, moderate and weak, respectively, in behavioural research, though there are no hard and fast rules explained by Hair and Alamer (2022). 22 R 2 aids in evaluating the explanatory power of the model and is supplemented by predictive relevance (Q2) to verify robustness and adjusted R 2 (for complex models).
The findings offer practical implications for healthcare management by shedding light on the direction and strength of the relationships among hospital efficiency, internal reputation and IPC measures. The analysis was further enhanced by the detection of possible mediating or moderating effects made possible by SmartPLS 4’s sophisticated algorithms. The results are guaranteed to be both statistically sound and practically applicable for enhancing healthcare outcomes thanks to this strong methodological approach.
The R 2 and adjusted R 2 values for the endogenous constructs show the significant explanatory power of the structural model. Hospital Efficiency’s R 2 of 0.538 (53.8%) and adjusted R 2 of 0.530 show that the predictor constructs, such as administrative controls, engineering controls, substitutions, eliminations, environmental controls and PPE, can account for a sizable portion of the variance in hospital efficiency outcomes. Even after accounting for complexity, the model is still robust, as evidenced by the tiny difference between R 2 and adjusted R 2 . According to the final outcome variable, hospital internal reputation, which exhibits even stronger predictive relationships with an R 2 of 0.583 (58.3%) and adjusted R 2 , the model’s predictors can account for nearly 58% of the variance in reputation. These findings show that hospital efficiency and internal reputation can both be strongly explained by the theoretical framework, with reputation being marginally more affected by the predictors that were included. The model’s efficacy in capturing important relationships in the healthcare context is empirically supported by the high R 2 values, both of which are above 0.50.
Discussion
In the process of conducting the study, it became important to identify the variables that can have an impact on the implementation of IPC measures. Previous research, like that by Brooks et al. (2021) 23 has demonstrated that demographic factors, including but not limited to gender, marital status, age, education level, income and years of work experience, have a substantial impact on the adoption and efficacy of IPC approaches. These characteristics influence individual compliance, flexibility and attitudes towards IPC procedures, which in turn influence views of the efficiency of the institution. For this reason, they were under statistical control in the current study to isolate the actual influence that IPC interventions had on the efficiency of hospitals. Gender and adherence to the IPC have always been associated. The number of studies has documented that female health workers are more compliant with cleanliness-protective situations.
Based on the 103 results of Ungar et al. (2023) 24 and Hu et al. (2012), 25 this increase in compliance among women is associated with the decrease in the number of procedural errors and the regular application of the protocol on IPC, both factors that indirectly increase the speed of hospitals. It is also indicated that age is a factor contributing to the behaviour of IPC, and younger employees will tend to have a more responsive level in terms of training and adaptation of procedures. Abdella et al. (2014) 26 and Gammon et al. (2007) 27 argue that younger professionals are more active in mobile communication and information technologies strategies and digital healthcare solutions, and, accordingly, this leads to the improvement of efficiency in the procedures and institutional agility. The other factor of importance is education, which significantly determines the effectiveness of prevention and control of infections.
The results of Aftab et al. (2015) 28 provide grounds to suggest that more educated individuals conduct and execute IPC practices better and accordingly report the improvement in the outcomes of infection control and more streamlined workflows. This adds more grounds in the choice of including education as a control variable. There is a non-linear correlation between the experience in the work and the compliance with the requirements of IPC. Alhumaid et al. (2021) 29 observed that professionals in the middle of their careers, with 6–10 years of experience, strike a balance between procedural familiarity and openness to change, which ultimately leads to increased IPC compliance and enhanced efficiency. Other factors that impact IPC habits include marital status and income, although in a roundabout way. Staff members who are married may have a greater aversion to risk and a better dedication to safety standards, stated Sax et al. (2017). 30
On the other hand, as brought forth in work by Schutte et al. (2024), 31 professionals with higher incomes, who are frequently in senior jobs, may have a bigger effect on the implementation of IPC and more control over their working environment. This research took into account these aspects because, even though they are not the 104 major emphasis, they do contribute to the variation in IPC-related attitudes and practices. The choice to account for these demographic parameters is based on the existing research that demonstrates the influence that these characteristics have on adherence to the IPC and, consequently, on the efficiency of the hospital. By keeping these factors as control variables, the study could assign observed effects to IPC measurements rather than underlying demographic disparities, which allows for a more accurate result.
Now focusing on the effect of IPC factors on hospital efficiency, the results obtained through SEM show that all six categories of IPC measures—administrative control, elimination, engineering control, environmental control, substitution and PPE—significantly contribute to hospital efficiency. These results reveal some clear trends in the contextual efficacy of these controls and support much of the body of knowledge already in publication. With their greatest standardised factor loading, administrative controls play a significant part in enhancing hospital efficiency. This is consistent with current research, such that by Jason et al. (2020), 32 which underlines that efficient IPC deployment depends fundamentally on established policies, frequent training and good workflow management; especially in resource-limited environments. The literature also highlights the scalability and cost-effectiveness of administrative controls, which are hence a pillar of sustainable IPC systems mentioned in WHO (2016). 33
The significant mediating impact here demonstrates that these behaviours not only enhance results but also serve as essential conduits for improving internal perceptions of efficiency. ENGNCONT had a notable yet somewhat reduced indirect impact (β = 0.029, p = .003). Engineering controls, including adequate ventilation systems, 111 negative pressure isolation rooms and automatic disinfection devices, facilitate the establishment of a controlled environment, thereby diminishing the danger of airborne transmission and cross-contamination. ENVCONT has a significant indirect influence of β = 0.034 (p = .002). Environmental controls, including regular surface sanitation, waste management and water quality assessment, are essential components of IPC systems. The study highlights them as the most prominent techniques of infection control, crucial for influencing frontline workers’ views of hospital cleanliness and safety. The mediating function of hospital efficiency suggests that the efficient integration of environmental controls into hospital procedures not only decreases infection rates but also enhances a disciplined and tidy operational image. This engenders a ripple effect regarding personnel perceptions of the institution’s reliability and dedication to safety. Such effects are robustly corroborated by research highlighting the symbolic significance of cleanliness and environmental hygiene in shaping organisational image, particularly in contexts where public expectations are escalating. The function of PERPRTEQP, exhibiting a mediated impact of β = 0.033 (p = .001), further substantiates this story. PPE serves as the primary and individual interaction between infection control policies and healthcare professionals. The literature emphasises that the accessibility, quality and proper utilisation of PPE are perceived by personnel as indicators of institutional care and readiness. Hospitals that provide consistent access to PPE and offer continuous training in its utilisation are 112 not only more effective in managing infections but also more inclined to gain the trust and loyalty of their staff. The mediating role of efficiency in this route substantiates the assertions that prompt procurement, inventory management and training systems—characteristics of effective management—are essential for PPE-related initiatives to enhance internal reputation favourably. The SUBSTITN variable (β = 0.039, p = .000) denotes the replacement of high-risk activities or materials with safer alternatives. Ultimately, ADMCONT has the lowest, although still considerable, indirect effect (β = 0.024, p = .013), indicating the presence of administrative controls such as infection reporting systems, compliance checks, signs and training. Although they are essential to IPC, their influence on hospital efficiency—and consequently internal reputation—may be seen as more procedural than operational.
The study emphasises that while administrative controls are essential for standardising and monitoring IPC processes, their implementation often falters, especially in overburdened public institutions. Investments in IPC infrastructure and policy must be complemented by systematic efforts to enhance process efficiency, facilitate interdepartmental cooperation and encourage resource optimisation. Only then can the whole reputational advantages—both internal and external—be attained. In conclusion, the results confirm the mediating role of hospital efficiency in the link between IPC variables and internal reputation. Every element of IPC has a distinct role; nevertheless, it is the hospital’s capacity to seamlessly incorporate these measures into routine operations that influences their perception among internal stakeholders. These findings corroborate the claims in the examined literature while providing empirical specificity, hence reinforcing the argument for IPC-centred efficiency methods as critical contributors to internal reputational value in Indian hospitals. In a prominent study by Archana and Mittal (2023) 34 discussed the pressing need of using the hierarchy of controls in measuring IPC. Recent advancements in healthcare technology adoption among women healthcare workers have shown measurable impacts on system efficiency and patient care delivery, as shown by Shahi et al. (2022). 35 Additionally, the integration of federated learning in AI-enhanced healthcare systems supports secure, decentralised data handling, further reinforcing hospital performance and reputation, as mentioned by Shahi and Mittal (2024). 36
However, it is important to acknowledge that this study relies on self-reported data, which is inherently subject to bias, such as overestimation of compliance or socially desirable responses. Furthermore, there was a lack of cross-validation with actual hospital infection rates or clinical audit data, which limits the ability to correlate perceptions with objective performance metrics. These limitations may affect the generalisability and robustness of the findings and highlight the need for triangulated methodologies in future research.
Systematic Literature Review
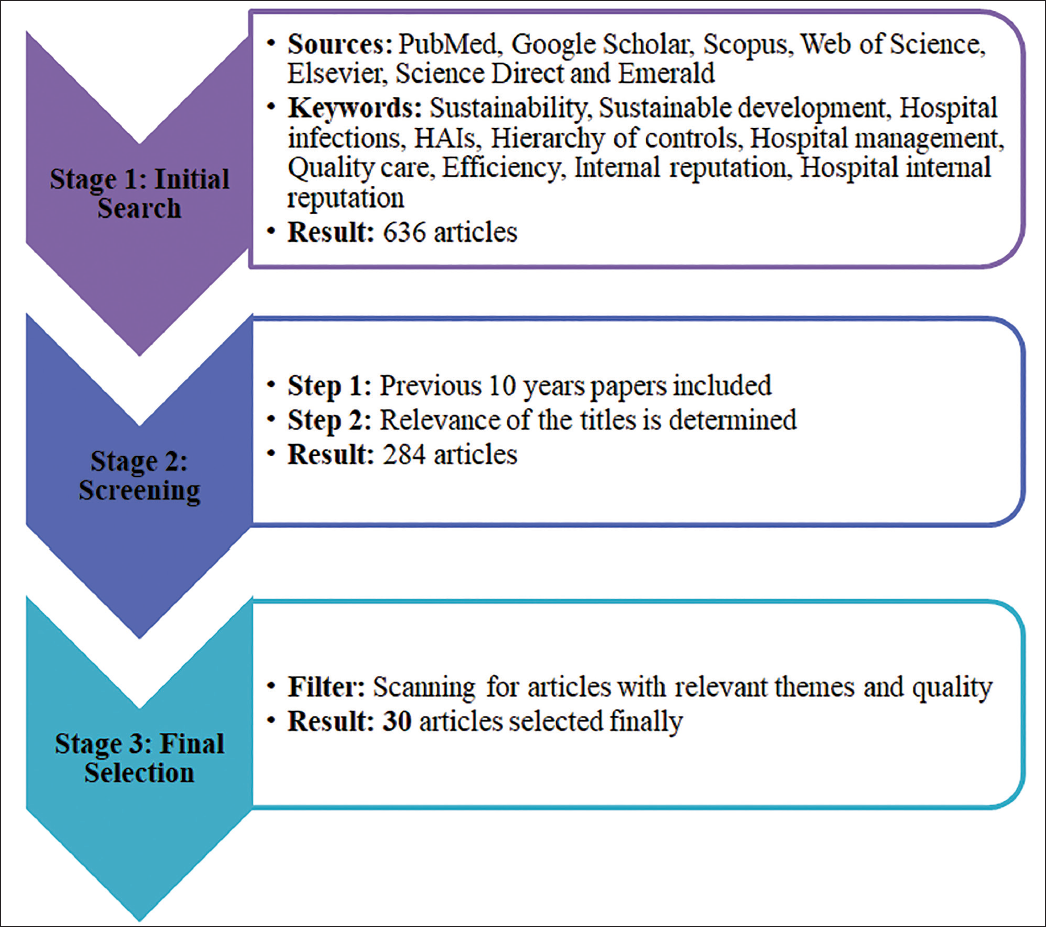
There are several databases that can be used to proceed with the literature study. For example, PubMed, Google Scholar, Scopus, Web of Science, Elsevier, Science Direct and Emerald. To identify the most relevant articles, different stages were followed, as given in the flow chart (Figure 3) underneath.
Overview of the Literature Review Document Screening.
Conclusion
The present study concludes that the IPC measures hospital efficiency and internal hospital reputation. It offers detailed insights into the hierarchy of IPC strategies—including elimination, substitution, engineering and administrative controls, environmental measures and PPE—highlighting their positive influence on hospital efficiency. Furthermore, the analysis confirms that hospital efficiency acts as a mediating factor between IPC measures and the internal reputation of Indian hospitals. The section concludes by summarising the study’s objectives and findings, and the final section outlines key implications, limitations and directions for future research.
Footnotes
Acknowledgement
We want to acknowledge our mentor and guide, Professor Dr Amit Mittal, Chitkara Business School, Chitkara University, Rajpura, Punjab, India.
Authors’ Contribution
Archana Shahi: Conceptualisation, Methodology, Data curation, validation, formal analysis, Writing-original draft Renu Thakur: Supervision, Review, Publication support.
Statement of Ethics
This study did not involve human participants, animals, or sensitive data; therefore, ethics approval was not required.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Anonymity
This submission does not contain any information that may compromise the anonymity of the authors, reviewers, or institutions involved.
Data Availability Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
ICMJE Statement
The authors have completed the ICMJE disclosure form. No additional relationships, activities, or interests were reported.
Patient Consent
This article does not contain any individual patient data; therefore, patient consent was not required.