
Abstract
Background
Elderly are a vulnerable population with an increased risk of hypertension-related cardiovascular mortality. Yog involving various asan, pranayam and meditation has been shown to decrease blood pressure in adults, but studies involving only elderly participants, practicing pranayam and meditation at home through a mobile guided system are lacking.
Purpose
To study the efficacy of home-based mobile-guided pranayam and meditation in the management of hypertension in the elderly.
Methods
The present study was carried out at the All India Institute of Medical Sciences, Rishikesh. Trial was started after registration in Clinical trial registration India (
Results
After 24 weeks, the intervention group exhibited a statistically significant reduction in SBP (decrease of 4.7 mmHg) compared to the control arm. Additionally, the intervention arm reported a significant improvement in sleep quality.
Conclusion
Study results indicate that home-based mobile-guided pranayam and yog nidra meditation are a valuable adjunct to the standard hypertension treatment in elderly individuals, not only lowering blood pressure but also enhancing sleep quality.
Introduction
Hypertension is a dominant risk factor for cardiovascular mortality. Globally, 7.7–10.4 million deaths are attributed to elevated blood pressure (BP) levels every year. 1 An increase in SBP by 20 mmHg and DBP by 10 mmHg is associated with a doubled risk of mortality from stroke, heart disease, or another vascular disease. 2 Randomised clinical trials among hypertensive individuals have demonstrated that a decrease of every 10 mm Hg in SBP reduces cardiovascular disease events by 20%, coronary heart disease by 17%, stroke by 27%, and heart failure by 28%. 3
It has been estimated that between 2015 and 2050, the world’s population above 60 years will nearly double from 12% to 22%. 4 A recent nationwide study reported an overall hypertension prevalence of 22.6% in India, with rates increasing significantly with age—reaching 48.4% among individuals aged 60 years and older. 5 As the prevalence of hypertension increases with age, we need to focus on the elderly to reduce the hypertension burden and associated morbidity and mortality
Besides antihypertensive medicines, lifestyle modifications that have been recommended as an equal first-line approach for controlling hypertension include: (a) weight loss in overweight or obese subjects and (b) DASH (dietary approaches to stop hypertension) diet. 3 Recent evidence has shown other methods like yog and various stress reduction techniques to be effective measures to reduce hypertension, simultaneously avoiding the side effects associated with antihypertensive medications.
Patanjali has defined yog as a means to join, direct, and concentrate one’s attention. The eight elements of yog are: yam, niyam, asan, pranayam, pratyahar, dharana, dhyan, and samadhi. Among these, asan, pranayam, and dhyan are among the frequently practiced forms. 6 Asan involve physical posturing techniques that are difficult for elderly individuals to perform; hence, pranayam and dhyan/meditation become preferred in the elderly. Pranayam includes deliberate breathing modification. 7 The purpose of meditation is to connect oneself to one’s deep inner self. 8
Numerous studies have demonstrated significant reductions in blood pressure and improvements in various lifestyle parameters following the practice of pranayam and meditation. However, the majority of these studies have primarily focused on middle-aged populations. The elderly, who exhibit a higher prevalence of hypertension and are more susceptible to its complications, remain underrepresented in this area of research. There is, therefore, a critical need to direct greater attention toward this vulnerable demographic.
The aim of this study is to evaluate the efficacy of home-based, mobile-guided pranayam and meditation in the management of hypertension in the elderly. To the best of our knowledge, this is the first study to assess the impact of a home-based, mobile-guided pranayam and meditation program on blood pressure and sleep quality, specifically in elderly individuals. Given that age-related musculoskeletal changes—such as arthritis, increased bone fragility, and reduced muscular strength—can hinder the performance of vigorous physical activity and yogic postures, 9 this study includes only pranayam and meditation as interventions, deliberately excluding postural exercises (asan).
Methods
Study Design and Setting
This is a randomised controlled trial conducted at the Outpatient Department of General Medicine, AIIMS Rishikesh, India.
Study Protocol
The study was conducted after approval from the institutional ethics committee. After taking written informed consent, 105 subjects were included in the study after meeting the inclusion and exclusion criteria.
Inclusion criteria: Elderly subjects between 60 and 75 years of age, diagnosed with hypertension (classified as per 2017 AHA/ACC guidelines).
Exclusion criteria: Subjects with active medical illness (diabetes mellitus, tuberculosis, chronic lung disease, symptomatic ischemic heart disease), recent (in last 30 days) myocardial infarction or stroke, any vertebral deformities, any diagnosed sleep disorder (obstructive sleep apnoea syndrome, narcolepsy, restless leg syndrome), and bedridden subjects.
Sample size: After reviewing the concerned literature, it was determined that a sample size of 52 participants per study arm (rounding off to a total: n = 105) will provide sufficient power (0.80) to detect a difference between groups, with a two-tailed α of 0.05 and effect size of 0.57. For sample size estimation, final SBP as an outcome variable of control and intervention arms was used from a study by Das et al. 10
Aim
To study the efficacy of home-based mobile-guided pranayam and meditation in the management of hypertension in the elderly.
Objectives
Primary objective: To determine the effect of home-based mobile-guided pranayam and meditation on SBP & DBP in individuals with hypertension & compare with standard treatment for blood pressure management.
Secondary objective: To determine the efficacy of home-based mobile-guided pranayam and meditation for change in sleep quality of the elderly.
Randomisation
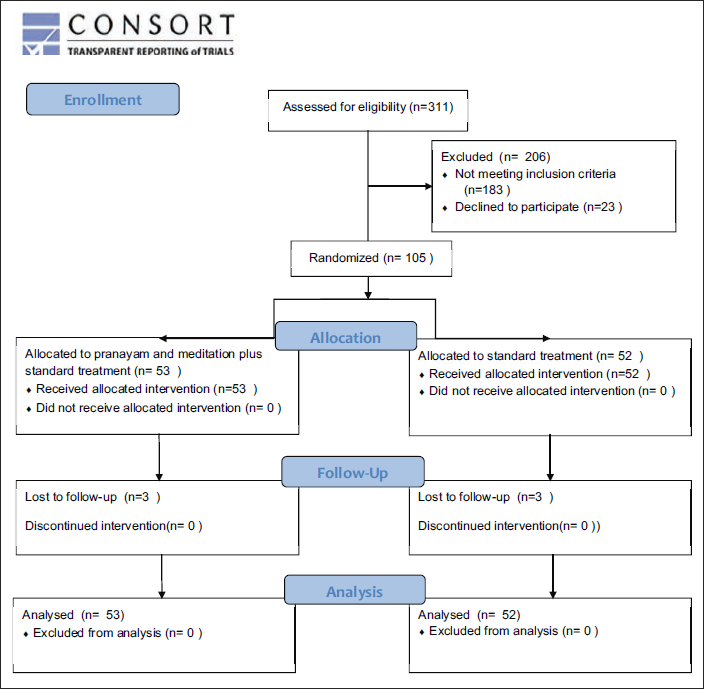
A total of 311 subjects were assessed for eligibility. Eligible participants were allocated to two arms (ratio 1:1) with the help of a computer-generated randomised sequence. A third person with no clinical involvement generated the random allocation sequence, ensuring an unpredictable allocation sequence. Sequentially numbered opaque sealed envelopes were used to conceal treatment allocation. Envelopes were opened sequentially & only after writing the participant’s name & other details to remove any chances of selection bias.
After enrolment, history was taken and a physical examination was done, systolic and diastolic blood pressures were recorded. PSQI (Pittsburgh Sleep Quality Index) questionnaire was filled out by the participant.
Intervention
The control arm was advised standard treatment as per 2017 AHA/ACC guidelines for hypertension (pharmacological and non-pharmacological). 3 The participants were advised: to go for a brisk walk for at least 40 minutes/day; to lower their alcohol consumption (no more than 2 drinks/day for men &1 drink/day for women); to restrict sodium consumption and follow DASH diet; to avoid smoking and pharmacological drug treatment was continued. The principal investigator advised participants in the intervention arm to follow the same standard treatment as the control arm, along with mobile-guided pranayam and yog nidra meditation. The principal investigator taught the pranayam and yog nidra meditation to participants in the intervention arm on the first day of enrolment at the outpatient department (OPD). Total duration of pranayam and yog nidra meditation was 40 minutes. Yogic Intervention Module, as shown in Table 1, was followed.
Yogic Intervention Module for Elderly Hypertensive Subjects.
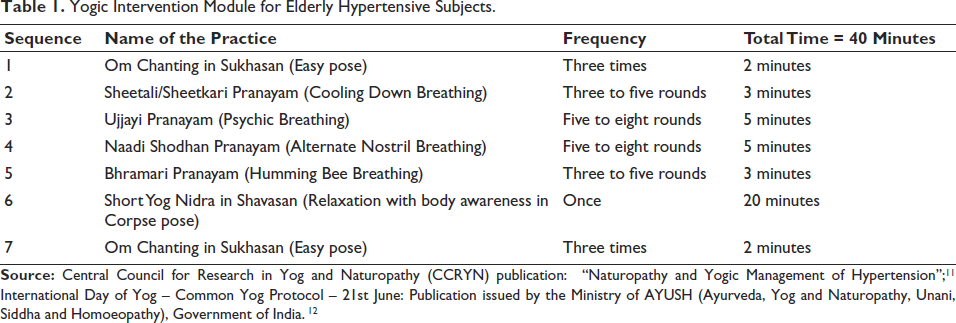
After learning the yog practice on the first day at OPD visit, participants were asked to log in from their devices for the pranayam and yog nidra practice at home, using video communication via the Zoom application. The module was practiced daily for 24 weeks, at 7:00
Blood pressure (BP) was recorded in both arms using an aneroid sphygmomanometer (Diamond Dial Deluxe), with repeat measurements taken at intervals of 1–2 minutes. The average of two readings was used for analysis. Sleep quality was assessed using the Pittsburgh Sleep Quality Index (PSQI), a self-reported questionnaire that evaluates sleep quality over the past month and has been validated in the Indian population. The questionnaire was either read out or given to the participants.
The yogic practices involved in this study were selected from the Central Council for Research in Yog and Naturopathy (CCRYN) publication ‘Naturopathy and Yogic Management of Hypertension’. 11 The yog protocol was developed based on the International Day of Yog - Common Yog Protocol - 21st June issued by the Ayurveda, Yog and Naturopathy, Unani, Siddha and Homoeopathy (AYUSH) Ministry of the Government of India, as shown in Table 1. 12 Yog nidra audio was taken from - Guided Meditation for sleep and relaxation by Sri Sri Ravishankar. 13
Blinding – due to the nature of the intervention, blinding was not possible for the participants and principal investigator, but the data analysis was done by a third person who was blind. Hence, this was a single blind study.
Statistical Analysis
MATLAB R2022a and R software were used for data analysis. The Shapiro-Wilk test was used to assess the normality of data. The data were then represented as mean and standard deviation. An independent t-test was used to compare the two arms, while a paired t-test was applied to assess changes within the same arm at baseline and follow-up. For data that were not normally distributed—namely, age, systolic blood pressure (SBP), and diastolic blood pressure (DBP)—the Wilcoxon-Mann-Whitney test was used to compare between arms, and the Wilcoxon signed-rank test was used for within-arm comparisons at different time points. A p-value of <0.05 was considered statistically significant. Data analysis was conducted according to the intention-to-treat (ITT) principle. To check the independent effect of the intervention on change in SBP and DBP, a multivariate linear regression analysis was done.
Results
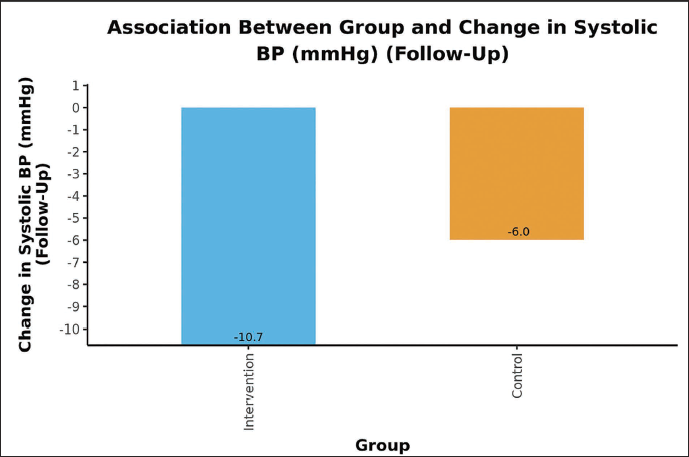
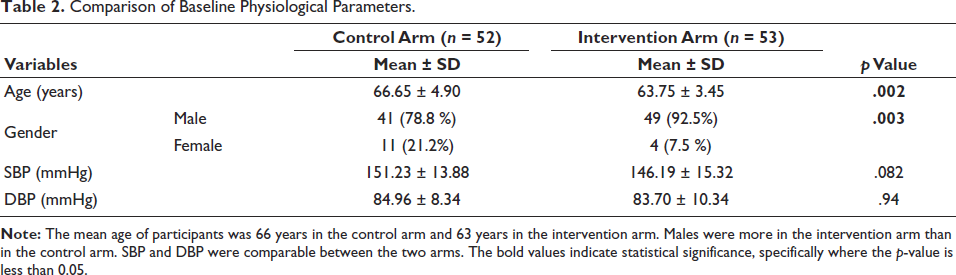
One hundred and five participants were enroled in the study, out of which six participants were lost to follow-up (Figure 1). The study’s findings reveal a significant impact of home-based mobile-guided pranayam and yog nidra meditation on systolic blood pressure (SBP) and sleep quality in elderly hypertensive individuals. The baseline physiological parameters (SBP and DBP) and PSQI scores were largely comparable between the control and intervention arms (Tables 2 and 3). While both groups experienced significant reductions in SBP and DBP within their respective arms from baseline to 24 weeks (Tables 4 and 5), the intervention group demonstrated a notably greater reduction in SBP over 24 weeks. Specifically, Figure 2 and Table 6 show a mean SBP decrease of 10.72 mmHg in the intervention arm compared to a 6.00 mmHg decrease in the control arm, a statistically significant difference (p < .001). The inter-group comparison for DBP change was not statistically significant (Table 6, p = .142).
Study Flow Chart.
Comparison of Baseline Physiological Parameters.
Comparison of Baseline PSQI Score

Mean Change in Physiological Parameters of Control Arm After 24 Weeks.

Mean Change in Physiological Parameters of Intervention Arm After 24 Weeks.

Comparison of Mean Change in Physiological Variables After 24 Weeks.

Beyond blood pressure, the intervention also led to a significant improvement in sleep quality. Figure 3 and Table 7 clearly illustrate a substantial mean reduction of 2.60 points in the PSQI score for the intervention arm, indicating improved sleep, compared to a much smaller 0.65-point reduction in the control arm (p < .001). Table 8 contains only the significant results because the function does not generate t-statistics for the variables which are not significant. Thus, the table shows that for SBP change, intervention (group minus control) and gender (gender minus male) are the significant variables.
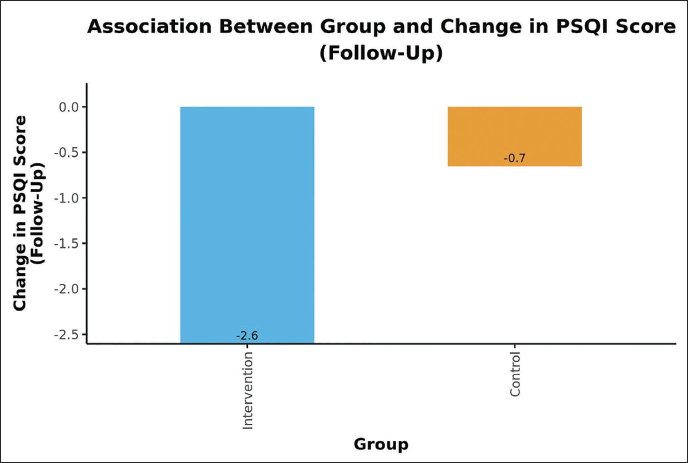
Comparison of Mean Change in PSQI Score After 24 Weeks.

Regression Analysis for Change in SBP Over 24 Weeks in the Intervention Arm.
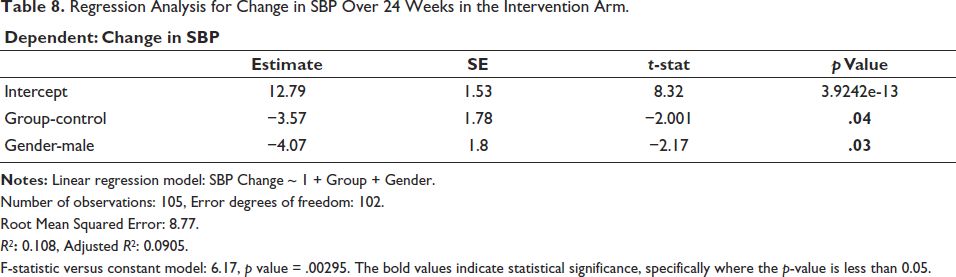
Number of observations: 105, Error degrees of freedom: 102.
Root Mean Squared Error: 8.77.
R 2 : 0.108, Adjusted R 2 : 0.0905.
F-statistic versus constant model: 6.17, p value = .00295. The bold values indicate statistical significance, specifically where the p-value is less than 0.05.
Discussion
Participants in the intervention arm had a mean age of 63 years and 66 years in the control arm (p value .002). There were 92% males in the intervention arm and 78% in the control arm. Kapoor et al., in their study, found that females in India have poor health-seeking behaviour. 14 Thus, fewer female participants recruited in our study can be attributed to the poor health-seeking behaviour of females in India, leading to low footfalls in hospitals. The rest all the baseline parameters were comparable in the two arms.
In a multicentre randomised control trial (RCT) by Dhungana et al., 121 hypertensive subjects between 18 and 70 years practiced yog in the form of postures, pranayam and meditation for 90 days, after which a significant decrease in SBP and DBP by −7.6 mmHg and −3.8 mmHg, respectively, was seen. 15 Our study also found a statistically significant reduction in SBP, with a difference of −4.7 mmHg between the two arms (p < .001). A statistically significant reduction in DBP was noted within the two arms after 24 weeks of follow-up. On comparing the two arms, the decrease in DBP was not statistically significant, which could be attributed to the non-inclusion of physical exercise in our study. DBP reduction is seen more in the exercisers. 16
The reduction in blood pressure observed in our study can be attributed to decreased sympathetic nervous system activity and enhanced parasympathetic tone induced by pranayam and meditation. During pranayam practice, the focus on controlled breathing and mindful awareness helps shift attention away from external stressors, promoting mental relaxation. This relaxed state facilitates autonomic balance by reducing sympathetic drive and enhancing vagal activity, which in turn leads to a decline in heart rate and blood pressure. Previous studies have reported similar findings, including improvements in baroreflex sensitivity and attenuation of both sympathetic and renin-angiotensin system activity following yogic interventions. 17
Similarly, yog nidra meditation decreases anxiety, leading to a decrease in stress-induced sympathetic overactivity and hence a reduction in BP. 18 Earlier studies have shown that the combination of three components of yog: asan, pranayam and meditation is responsible for a higher reduction in SBP and DBP compared to any two components. 19
To check whether the change in BP was truly due to intervention or due to the baseline differences in the composition of the two arms, we did a multivariable regression analysis taking group, age, and gender as the independent variables. The adjusted R 2 was 0.09 (p value .04) for the intervention. Which shows, pranayam and yog nidra meditation were a significant variable for reducing SBP in the intervention arm. Gender was also significantly related to SBP reduction in the intervention arm, more reduction seen in females. An RCT by Wolff et al. also showed a greater reduction in SBP in females than in males after yogic intervention. 20 In our study, the change observed in DBP in the intervention arm, compared to the control arm, was not found to be significant.
In an RCT by Datta et al., yog nidra meditation practiced for 5 weeks in 41 subjects, led to significant improvement in sleep quality, assessed through polysomnography and PSQI scores. 21 In our study, sleep quality improved significantly after 24 weeks of intervention as observed by a mean change in PSQI score of −2.6.
A part of the study after participant enrolment and randomisation was done during the COVID-19 pandemic, and during that time, our study came out to be more handy, as during the pandemic elderly were restricted to homes and being a high-risk group for hypertension they were at greater risk for complications associated with high blood pressure. Doing daily pranayam and yog nidra meditation through the mobile-guided online platform helped them manage their hypertension while being at home and, simultaneously, avoiding the stress and expenditure associated with visits to the hospital. Mobile health-based services/telemedicine are easily accessible, reduce the dependence of the elderly on others, and are helpful for isolated patients due to pandemics (e.g., COVID-19) and in medically underserved areas. It leads to better treatment adherence and is a recommended platform for managing hypertension in the elderly. 22
Previous literature suggests that the inclusion of asans in yog-based interventions may contribute to a more pronounced reduction in diastolic blood pressure. Asans involve mild to moderate physical activity, which can improve vascular compliance and autonomic balance, thereby supporting DBP reduction. Studies by Hagins et al. and Wolff et al. have shown that yog protocols integrating all three elements—asan, pranayam, and meditation—result in greater improvements in both SBP and DBP compared to protocols excluding physical postures.19, 20 Since our study excluded asans to accommodate the elderly population, this may explain the non-significant reduction in DBP observed in our findings.
Administering the yog protocol presented certain challenges. Ensuring consistent participation and adherence to daily virtual sessions over a 24-week period required sustained effort from both participants and the research team. Although attendance was monitored via Zoom and weekly reminders were provided, maintaining long-term engagement was difficult, particularly in the absence of in-person supervision. Technical issues such as internet connectivity problems, limited digital literacy among some participants, and distractions in the home environment occasionally disrupted the quality of sessions. The inability to reinforce practices through face-to-face interactions, due to the COVID-19 pandemic, further limited opportunities for real-time correction of technique and motivation.
This study has a few limitations that should be acknowledged. First, the sample size was relatively small (n = 105), which may limit the generalisability of the findings. Larger studies with more diverse populations are needed to validate these results. Second, due to the COVID-19 pandemic, in-person follow-up visits were restricted, which may have impacted the consistency of data collection. Future research should aim to incorporate more frequent follow-up visits to enhance data accuracy and monitor adherence. Despite these limitations, the study provides important evidence supporting the integration of yogic practices in hypertension management.
Conclusion
Based on our study results, we recommend mobile-guided pranayam and yog nidra meditation for the control of hypertension in elderly subjects. The elderly, who are a dependent population, if equipped with mobile guided services, through telemedicine, can manage their blood pressure and have better sleep quality while staying at home. This will also decrease the requirement of frequent hospital visits, thus reducing the financial burden.
In this study, a non-significant reduction in DBP could be due to the non-inclusion of asan, considering the elderly population. So, we recommend adding asan for hypertension control in the younger population.
In future, more extensive, large sample size studies must be conducted to affirm our findings further.
Footnotes
Abbreviations
AHA/ACC: American heart association/American college of cardiology
SBP: Systolic blood pressure
DBP: Diastolic blood pressure
CTRI: Clinical trial registration India
BP: Blood pressure
DASH: Dietary approaches to stop hypertension
PSQI: Pittsburgh sleep quality index
OPD: Outpatient department
CCRYN: Central Council for Research in Yog and Naturopathy
AYUSH: Ayurveda, Yog and Naturopathy, Unani, Siddha and Homeopathy
n: number
ITT: Intention to treat
SD: Standard deviation
RCT: Randomised controlled trial
Acknowledgement
We would like to acknowledge the All India Institute of Medical Sciences, Rishikesh, for giving us this opportunity and the subjects who participated in the study. We also wish to express our sincere appreciation to Sri Sri Ravishankar for creating Yog Nidra Audio.
Authors’ Contribution
Dr Akshita - Primary author, who conducted the study.
Dr Monika Pathania - Helped with the study design.
Dr Ranjeeta Kumari and Dr Navdeep Ahuja - Helped with the statistical analysis.
Dr Minakshi Dhar - Helped with patient recruitment.
Dr Praag Bhardwaj - Helped with online zoom meeting sessions.
Sumathi Jayaraman, Director, SSIAR - Helped with Yog Nidra Module.
Statement of Ethics
The study was conducted after approval from the Ethics Committee of AIIMS Rishikesh (AIIMS/IEC/20/644).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
ICMJE Statement
Attached in a separate Word document as supplementary files.
Patient Consent
Written informed consent was given by all the participants recruited in the study.