
Abstract
Background
Examination stress is a very well-known model of psychological stress in students. It induces changes in systolic (SBP) and diastolic blood pressure (DBP), along with changes in heart rate variability (HRV) and baroreflex sensitivity (BRS), due to autonomic perturbations.
Purpose
To find out if Raj Yoga meditation (RYM) practice affects autonomic and cardiovascular function in healthy young subjects during periods of examination stress. Our primary objective was to evaluate the effect of one month of supervised RYM practice on ameliorating examination-induced changes in cardiovascular and autonomic function. The secondary objective was to measure the stress levels of medical students before and after RYM.
Methods
Pre-training measurements of SBP, DBP, HRV, and BRS were done, and the Medical Student Stressor Questionnaire (MSSQ) was administered to 80 participants one month before examinations. They were then trained in RYM. Post-training assessment of the same parameters was done after examinations and also after two months.
Results
In our study, RYM training decreased DBP (p = 0.01) but not SBP. BRS showed a trend towards an increase after RYM practice, but it was not statistically significant (p = 0.44). The standard deviation of the NN interval (SDNN) (p = 0.03), low-frequency (LF) nu (0.003), and high-frequency (HF) nu (0.04) showed a statistically significant change. Average RR, median RR, average rate, square root of the mean squared differences of successive NN intervals (RMSSD), pRR, total power, LF (µs2), and LF/HF ratio were not statistically significantly different between the three groups. There was a statistically significant decline in MSSQ scores for MSSQ I (p = 0.04), MSSQ II (p = 0.04), and MSSQ IV (p = 0.03).
Conclusion
Short-term practice of supervised RYM during stressful periods is protective for the cardiovascular and autonomic systems and decreases stress in medical students.
Introduction
The term “meditation” in common parlance is used to refer to varied techniques such as the use of natural sounds such as chirping birds or flowing water, yogic postures, breathing exercises, word repetition, contemplation on a single thought or concentrating on a point, and guided meditation. These techniques help the practitioner by affecting several components, such as the senses, emotions, breath, mind, and intellect. Some meditation techniques are relatively easy to learn and practice, while others are tough, and therefore the participants do not remain consistent in their efforts. 1 Although there is no consensus definition of meditation, yet a generalized description to understand the scientific basis of meditation, which can help to serve as a starting point, can be stated as “a learned technique with which to change a state of being attentive to identified stimuli, to a state of unfocused attention.” 2 From a physiological perspective, meditation can also be referred to as a kind of homeostatic regulatory process, in which the individual engaging in meditative practice tries to maintain an unperturbed internal environment whenever there is a perceived threat to homeostasis. Since these practices of meditation originated in the ancient Vedic times in India; therefore, the classical literature lays more emphasis on its philosophical dimension.
Meditation is a part of “Ashtang yoga,” which has been described vividly in the classical Indian scripture Yoga Sutra written by the great Indian sage Patanjali (600–400 BCE). 3 Simply stating, Ashtang yoga depicts a tree with eight branches. In simple words, these branches represent universal ethics, individual ethics, postures, breath control, control of senses, concentration, meditation, and bliss. Thus, by following this eightfold path of yoga, one can relax the mind, and a peaceful mind can control the body better. 3 Much literature is available on the physical and mental health benefits of the daily practice of postures and breathing exercises. 4 However, how meditation benefits an individual’s physiological functioning is not yet known. Raj yoga is a form of meditation in which the steps for attaining the highest state of consciousness have been clearly laid out. A non-governmental organization (NGO) named Brahma Kumaris World Spiritual University (BKWSU) conducts training courses of Raj Yoga meditation (RYM). 5 RYM can be understood more scientifically as a method of self-relaxation, with a divine connection. It helps in realizing the true self by contemplating on the “supreme being,” and engaging in a dialogue with the divine. Raj yoga practice has been suggested to lead to several psychological and physiological benefits in healthy individuals and diseased patients. 6
Performance in examinations determines the future prospects of students, and therefore examination stress is well known to induce psychological stress in students. Changes in stress markers such as salivary cortisol, immunoglobulin A, and luteinizing hormone in students during examination stress7–9 have been reported. Examination stress also induces changes in systolic blood pressure (SBP), diastolic blood pressure (DBP), mean blood pressure (MBP), heart rate variability (HRV), and baroreflex sensitivity (BRS)10–13 most probably due to autonomic perturbations. Performing yoga leads to a reduction in sympathetic activity and an enhancement of cardiovagal function. 14 Daily meditation practice may cause a change in autonomic tone from primarily sympathetic to parasympathetic predominance. There is insufficient evidence in the literature regarding the effects of RYM on autonomic and cardiovascular function in apparently healthy young subjects during periods of examination stress.
Therefore, our primary objective was to evaluate the effect of one month of supervised RYM practice in ameliorating examination-induced changes in cardiovascular and autonomic function measured by SBP, DBP, HRV, and BRS. Secondary objectives were to measure the stress levels of medical students before and after RYM intervention and to find out if autonomic function parameters (HRV and BRS) and stress levels as measured by the Medical Student Stressor Questionnaire (MSSQ) are correlated.
Methods
This study had a prospective pilot cohort design with purposive sampling. A sample size of 80 is considered appropriate to test the feasibility of a new intervention, 15 so we also took the same sample size in our study. Approval was obtained from the Research and Ethics Committee of the institute. After this orientation, lecture for first-year students regarding the beneficial effects of yoga on various physiological systems of the body was conducted by two investigators involved in the study. Informed consent was obtained from interested participants. Students with a history of substance dependence, except caffeine, or significant medical illnesses such as hypertension, asthma, and diabetes mellitus were excluded from the study. Screening for substance dependence was done using a self-reported questionnaire. A detailed history and clinical medical examination were done to exclude major medical illnesses such as diabetes, hypertension, and asthma.
Data Collection Procedure
All recordings were done in a calm, temperature-controlled room where the ambient temperature was maintained between 21°C and 25°C. Subjects reported to the laboratory between 8 and 11 AM and after having their last meal twelve hours before reporting time. All participants were contacted telephonically two days before their recording. They had only a light breakfast for at least two hours before reporting to the laboratory for measurements. They were instructed to abstain from caffeine-containing beverages for twenty four hours before testing.
The pre-training measurements of SBP, DBP, HRV, and BRS were done one month before examinations. Along with this, the MSSQ questionnaire was also administered. Then, the participants started RYM practice. After completing one month of training, the post-training assessment of SBP, DBP, HRV, BRS, and MSSQ was done. The timing of this second measurement coincided with the time when the students were about to take their first professional examinations, which was a very stressful period for them. The third measurement of cardiovascular and autonomic parameters was done two months after completion of RYM, at a time when the students’ exams were over and the examination-induced stress was also not there.
Anthropometric Profile
The weight was measured in kilograms with an electronic balance. For measuring height, the subjects stood erect with their heads in the Frankfurt plane in front of a wall-mounted, non-extensible measuring tape with no shoes and their feet together. Body mass index (BMI) was calculated using the formula: Weight (kg)/Height (m2). An aneroid sphygmomanometer was used to measure systolic and diastolic blood pressure.
ECG and Beat-to-Beat Digital Blood Pressure
All measurements were done after resting in supine posture for ten minutes and breathing spontaneously at a comfortable tidal volume. Lead II ECG was recorded simultaneously along with the beat-to-beat blood pressure using a human non-invasive continuous blood pressure recording machine (Model ML 283, Finapres Medical Systems Amsterdam, The Netherlands). For ECG recording, the sampling frequency was 1 kHz. The bandpass filter was set at 0.5 Hz for low and 35 Hz for high cutoff frequencies. A sampling frequency of 200 Hz was used for beat-to-beat BP signal acquisition. Signal recording was done in Lab Chart software version 8 (AD Instruments, Australia) and saved for BRS and HRV analysis later on.
Medical Student Stressor Questionnaire (MSSQ)
MSSQ was used to identify the source of stress. The MSSQ was administered at the beginning and end of the RYM intervention. This questionnaire has been validated in several countries, including India. 16 The source of stress specific to medical students is classified into several domains, such as academic-related stress (Domain I), interpersonal stress (Domain II), teaching and learning-related stress (Domain III), social stress (Domain IV), drive/desire-related stress (Domain V), and group activity-related stress (Domain VI).
Baroreflex Sensitivity (BRS) Analysis
The sequence method was used for calculating BRS. Same period, ECG and blood pressure segments were first selected. Then, using a software, the linear regression slope between beat-to-beat SBP and the RR interval was calculated. Then, sequences in which SBP and RR intervals concurrently increased or decreased for at least three consecutive beats were identified and used to calculate the BRS value.17–20 Nevrokard software (Version 6.2.0, Nevrokard Kiauta, Izola, Slovenia) was used for analysis.
Heart Rate Variability (HRV) Analysis
A five-minute segment of electrocardiographic (ECG) data was used to compute HRV in the time and frequency domains. 21 Individual QRS complexes are detected from a continuous ECG record, and the NN interval (intervals between adjacent QRS complexes due to sinus node depolarizations, i.e., the instantaneous heart rate) was determined. From this, the square root of the variance, that is, standard deviation of the NN interval (SDNN) was calculated. Mathematically, variance (SDNN) is equal to the total power of spectral analysis, so it reflects all the cyclic components responsible for variability in instantaneous heart rate. SDNN represents the overall HRV, including both long- and short-term variability.
The most commonly used time domain measurement is the square root of the mean squared differences of successive NN intervals (RMSSD). The number of interval differences of successive NN intervals greater than 50 ms (NN50) and the proportion derived by dividing NN50 by the total number of NN intervals (pNN50) measure short-term variation and estimate high-frequency (HF) variations, that is, parasympathetic activity. They are also highly correlated. 22
From the frequency and magnitude of the series of changing RR intervals, the power density calculation for separate frequency ranges was done. Low frequency (LF) reflects baroreceptor activity and is modulated by both the sympathetic and parasympathetic nervous systems. The parasympathetic nervous system modulates the HF range component (0.15–0.4 Hz) and is connected with respiration and blood pressure changes. The LF/HF ratio reflects sympathovagal balance.
RYM Intervention
A seven-day RYM introductory course was conducted in the yoga laboratory of our institute by an expert RYM trainer. Each session was of one hour duration. In the first three days, the RYM expert discussed with the participants different types of stress and how they can cope with it. After this, the participants were trained in RYM through positive imagery and guided meditation techniques. In the next two days after this (fourth and fifth days), participants were shown videos by the RYM trainer (BK Neha) entitled “Discover the Spirit Within,” “Essentials of Raja Yoga,” and “Who Am I?” along with their daily meditation. A point of light was focused on the screen, and students focused their attention on it while keeping their eyes open. Subsequently, on the sixth and seventh days, when the participants had got accustomed to the technique of RYM, they were told to identify with one positive quality (e.g., peace, happiness, love, or calmness) and then to keep focusing their attention on it while in meditation. After this RYM introductory course, students continued practicing the same technique for the entire month. By general consensus, the students agreed to practice daily meditation between 8:00 and 9:00 AM in the Department of Physiology before their routine classes. Investigator (AB) supervised their daily meditation practice. She also took half-hourly sessions each day to explain to the participants the physiological basis of stress in the modern world and the scientific basis of how meditation helps relieve it.
Statistical Analysis
The data were checked for normality using the Shapiro-Wilk test. Normally distributed dependent variables were analyzed using repeated measures ANOVA with pair-wise comparison (Bonferroni). In the case of a non-parametric distribution of data, Friedman’s ANOVA was applied for the dependent variable, with the Wilcoxon sign rank test for pair-wise comparisons. A p-value < 0.05 was considered significant.
Results
The mean age, weight, and BMI of eighty healthy medical undergraduates were 18.70 ± 0.77 years, 61.30 ± 11.40 kg, and 22.34 ± 3.76 kg/m2, respectively.
Table 1 shows anthropometric, cardiovascular, and autonomic function parameters before, after, and after two months of RYM.
Anthropometric, Cardiovascular, and Autonomic Function Parameters Before, After, and After Two Months of RYM.
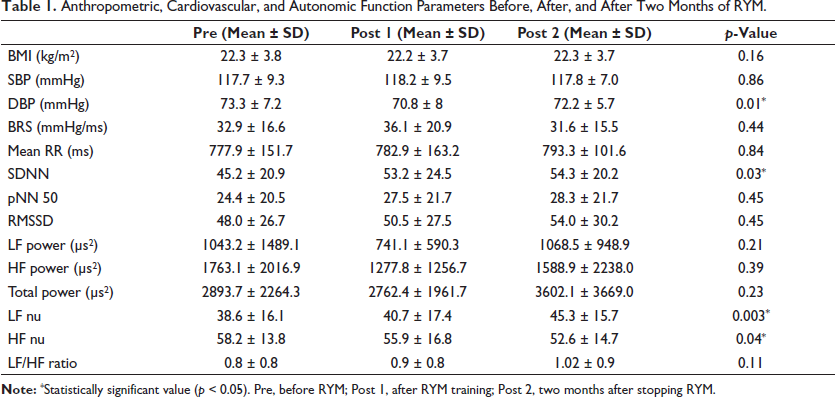
SBP did not show any statistically significant change among the three groups. The mean DBP showed a statistically significant difference between the three groups (p = 0.01). Post hoc analysis of the results indicates that the decrease in DBP after RYM training and was statistically significant (p = 0.01). DBP before RYM training was 73.27 mmHg, decreased to 70.75 mmHg after RYM training, but returned to 72.15 two months after stopping RYM training.
The changes in BRS values were not statistically significant (p = 0.44). It showed a trend toward an increase after RYM practice. The BRS value at baseline was 32.9 ms/mmHg. It increased to 36.1 after one month of intervention and returned to 31.6 ms/mmHg after two months.
Figure 1a shows the frequency domain HRV parameters before, after, and after two months of RYM.
Frequency Domain HRV Parameters Before, After and After 2 Months of RYM. b) Time Domain HRV Parameters Before, After and After 2 Months of RYM.
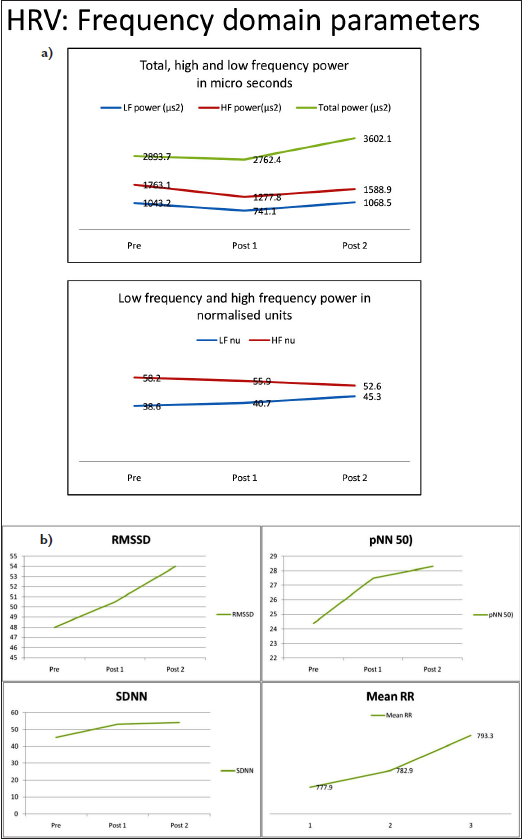
Figure 1b shows the time domain HRV parameters before, after, and after two months of RYM.
In all the time and frequency domain parameters, only SDNN (p = 0.03), LF nu (0.003), and HF nu (0.04) show a statistically significant change.
In the HRV parameters, no statistically significant difference in average RR, median RR, average rate, RMSSD, pRR, total power, LF (µs2), and LF/HF ratio was seen between three groups.
LF nu was statistically significantly different between the three groups (p = 0.003). At baseline, LF was 38.6 nu. It increased to 40.7 nu after intervention and 45.3 nu after two months. Post hoc analysis revealed no significant difference between the pre- and post-intervention values. A significant difference was present in the values of LF before and two months of intervention (p < 0.001) and also between LF values post-intervention and after two months of intervention (p < 0.01).
No statistically significant difference existed between pre- and post-intervention SDNN. The SDNN pre-values, when compared to values two months after the intervention, showed a statistically significant difference (p = 0.001).
HF nu values were also statistically significant between the three-time points (p = 0.04). The value of HF at baseline was 58.2 nu and decreased to 55.88 nu and 52.63 nu post intervention and after two months of the intervention, respectively. Post hoc analysis revealed a statistically significant decrease in HF values after two months compared to values at baseline (0.01) but no significant difference in the pre- and post-values.
Although LF/HF % was not statistically significant different between the groups, there was an increasing trend in these values. The mean value at baseline was 0.77. It rose to 0.85 after intervention and 1.02 after two months of intervention.
Table 2 shows the MSSQ scores of participants before and after the RYM intervention.
MSSQ Scores of Participants Before and After the RYM Intervention.
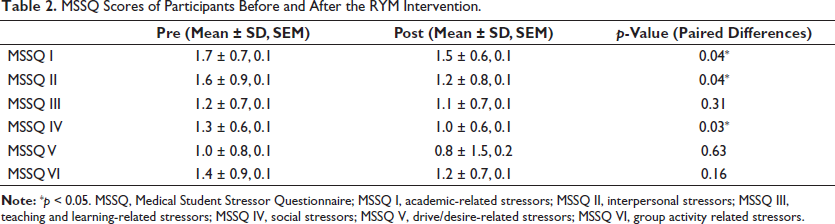
In the MSSQ scores also, there was an overall trend of decline in all domains after the intervention, and it was statistically significant in MSSQ I (p = 0.04), MSSQ II (p = 0.04), and MSSQ IV (p = 0.03) scores.
Table 3 shows the correlation coefficient between BRS and various MSSQ domains.
Correlation Coefficient Between BRS and Various MSSQ Domains.

Statistical analysis shows a weak correlation between BRS and MSSQ scores in various domains. Similarly, HRV parameters and MSSQ scores also show a weak correlation.
Discussion
We report for the first time the utility of one month of supervised RYM training in ameliorating changes induced in the autonomic and cardiovascular systems by examination stress in undergraduate medical students. Our findings indicate that one month of supervised RYM training leads to no change in SBP and a decline in DBP for first-year medical undergraduate students. BRS values show an increasing trend. There is an insignificant increase or no change in most of the time- and frequency-domain measures of HRV. Stress scores show a decline in all domains but a significant decrease in stress related to teaching and learning, inter- and intrapersonal-related stress, and stress related to group activities.
Recent studies show that examination-related stress increases SBP and DBP and lowers BRS values during the exam period compared to the semester time in healthy college students.10–12 An examination can lead to significant stress, which can put the cardiovascular system at risk even in young, healthy individuals. The stress levels are even higher for medical students during their pre-examination period. Constant exposure to stress is harmful in the long run as it disrupts the homeostatic balance and may be a risk factor for derangements in the cardiovascular and respiratory systems, 12 leading to disease. In a study conducted on medical students using academic examinations as a model of mental stress, it was found that the mean arterial pressure increased and the mean RR interval, SDNN, and pNN50 were significantly reduced during examinations. However, RMSSD shows no significant difference. The absolute power in the LF band was significantly less during examinations. The mean arterial pressure was significantly higher during examinations. 13
With the above facts in mind, we used examination stress as an acute stress model for medical students to evaluate how the daily practice of RYM helps prevent examination stress-induced changes in cardiovascular and autonomic parameters. We also wanted to inculcate a routine that would help students handle a highly competitive world without getting stressed. Regular meditation enhances the capabilities of the sensitive mind and makes the intellect more sharp. Total awareness of actions leads to a relaxed approach and enables one to interact with society judiciously and effectively. 23
In our study, when students practiced RYM during examination stress period, the SBP did not change and the DBP declined. The BRS reading showed a trend toward an increase. There was an insignificant increase or no change in most of the time- and frequency-domain measures of HRV. There was a trend toward an increase in the mean RR interval, SDNN, pNN50, and RMSSD after one month of RYM practice compared to baseline values. This increasing trend was seen even after two months. However, this increase was statistically significant for only SDNN. Compared to the pre-training scores, stress scores decreased in all domains after RYM training. There was a significant decrease in inter- and intrapersonal-related stress, teaching- and learning-related stress, and group activities-related stress. These findings are most likely because our students were practicing RYM during the period of examination stress and, hence, were protected from the ill effects of examination-related stress on the cardiovascular and autonomic systems. Thus, daily practice, or RYM, for a month helps to counteract mental stress caused by examination and thus calms down the examination stress-induced state of cardiac sympatho-excitation. The effect of daily practice of RYM is evident even after two months of the intervention.
To investigate recordings of short durations, the time domain measurements (SDNN and RMSSD) are used. However, the frequency methods provide more easily interpretable results to understand physiological regulations. There is no consensus regarding the LF component. According to some studies, LF (in normalized units) is a quantitative marker for sympathetic modulations while other studies consider LF to denote both sympathetic and vagal activities. Therefore, some investigators consider the LF/HF ratio to reflect sympatho-vagal balance or sympathetic perturbations. Since HRV is an indirect marker of changes in autonomic inputs to the heart, autonomic withdrawal and a high level of sympathetic input will cause a decrease in HRV. 24
The mean RR interval indicates the ratio of the sympathovagal balance. Thus, RYM practice during examination stress leads to a tilt of sympathovagal balance toward the parasympathetic side, as depicted by an increase in the mean RR interval.
The trend toward an increase in SDNN during examinations reflects an increase in total HRV due to the practice of RYM during mental stress, which is also evident by the increase in total spectral power. The mean values of the LF and HF also show similar trend toward an increase. However, all these findings are not statistically significant.
Changes in both pNN50 and RMSSD denote HF changes in heart rate and parasympathetic variations. Out of the two RMSSD is a better parameter than pNN50 for resting HRV changes.22, 25
An increase in RMSSD value after intervention in comparison to pre-intervention levels indicates a change in the HF component of parasympathetic modulation due to RYM practice. Although the normalized HF values after RYM training show a decrease from baseline values, this decrease is smaller than the values of HF after two months of RYM training and is not statistically significant. The normalized LF values also show an increase from baseline after one month of RYM practice, but this increase is not statistically significant. Thus, practicing RYM during examination stress prevented the changes in the LF component due to examination-induced excitation of the sympathetic system and the withdrawal of parasympathetic influences.
The ratio of changes in sympathetic versus. parasympathetic tone is measured using the LF/HF. No significant change across the pre- and post-intervention recordings in the mean LF nu, HF nu, and the LF/HF ratio was seen in our study. Thus, the sympatho-vagal balance was not altered due to examination stress when the students practiced daily RYM. Thus, the parameters that indicate the relative proportion of the modulation of the two limbs of the cardiac ANS remain constant under conditions when RYM is practiced concomitantly with a period of mental stress.
Several studies have shown that although yoga may influence autonomic function, it may not necessarily reflect a change in HRV.26–33 Although in-depth reviews are available on various aspects of yoga and HRV,34, 35 there is no firm conclusion from these studies for several reasons. 14
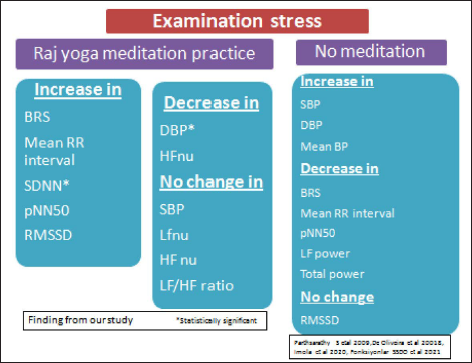
Figure 2 summarizes the findings of our study on cardiovascular and autonomic parameters when students practice meditation during a period of examination stress in comparison to the findings available in the literature regarding the effect of examination stress.
Summary of the Role of Meditation in Ameliorating Examination Stress Induced Changes in Cardiovascular and Autonomic Parameters.
Stress levels among Asian medical undergraduate students are much higher than in the West. 36 The undergraduate medical students undergoing psychiatric treatment may just be the visible tip of the iceberg. There might be a large proportion of students who are having behavioral problems, disturbed interpersonal relationships, or deteriorating performance, but they hesitate to come forward to seek help for it. Psychiatrists attribute this disturbing trend to the competitive education systems, which have put the present-day youth at a crossroads without any means of coping with this stressful environment. In a professional college, students are further tormented and stressed by a new environment. The highly demanding curriculum and excessive academic competition create intense demands on students in physical, emotional, intellectual, financial, and social aspects. This leads to a failure of coping and contributes to high stress levels in medical students. 37
Performing yoga leads to less examination-related stress in medical students. 35 However, the type of yoga practice that students performed in an earlier study 35 was a one hour program beginning with a prayer, some yogic postures, breathing exercises, relaxation exercises, and meditation, which was different from the RYM practiced in our study. Another difference in this study was the use of Spillberger’s anxiety scale, which measures anxiety (situational and general levels) in an individual as a stable personality trait in a general context. In contrast, we used the MSSQ, a scale specifically developed to assess anxiety in medical students in various domains.
Conclusion
Even a short-term practice of supervised RYM during stressful periods is protective for the cardiovascular and autonomic systems and decreases stress in medical students.
Footnotes
Abbreviations
SBP, systolic blood pressure; DBP, diastolic blood pressure; MBP, mean blood pressure; HRV, heart rate variability; BRS, baroreflex sensitivity; RYM, Raj Yoga meditation; MSSQ, Medical Student Stressor Questionnaire; NN interval, intervals between adjacent QRS complexes; SDNN, the standard deviation of the NN interval; RMSSD, square root of the mean squared differences of successive NN intervals; NN50, number of interval differences of successive NN intervals greater than 50 ms; pNN50, the proportion derived by dividing NN50 by the total number of NN intervals; LF, low frequency; HF, high frequency; BMI, body mass index.
Acknowledgements
We acknowledge the contribution of students in the MBBS first year, whose enthusiastic participation was the main driving force for the successful accomplishment of this project. We also sincerely acknowledge BK Neha Didi for gently training and guiding the participants in performing the steps of RYM.
Authors’ Contribution
All authors are accountable for all aspects of the work, ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
A.B., A.S.M., and A.K.S. were responsible for conceptualizing the research and deciding on the methodology to be followed.
A.B. was responsible for the acquisition of data, and A. B., S.S., and A.S. M. analyzed and interpreted the data.
A.B., S.S., R.R., and K.K.D. were involved in drafting the manuscript and critically reviewing it for important intellectual content. Overall mentorship and approval of the final version were done by A.S.M. and K.K.D.
Statement of Ethics
Ethical approval was obtained by the Ethics Committee of our institute (GMCH, Chandigarh) vide letter no. IEC/2017/05 dated 25/04/2017.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Department of Science and Technology-UT, Chandigarh, vide sanction no. S&T&RE/RP/03/2017/233-239 dated 08/03/2017.
ICMJE Statement
This article complies with the International Committee of Medical Journal Editors (ICMJE) uniform requirements for the manuscript.