
Abstract
Background
The issue of adverse childhood experiences (ACEs) has received critical attention in understanding the complexity of neurodevelopmental disorders (NDDs). Despite growing empirical support demonstrating the role of ACEs in neurodevelopment, there is little research on their distinct role in the onset, severity, and progression of NDDs, specifically attention deficit/hyperactivity disorder (ADHD), autism spectrum disorder (ASD), and cognitive impairments.
Summary
The goal of this systematic review is to critically summarise the existing research on the relationship between ACEs and NDDs, assess current knowledge about their interdependency, identify the gaps in the literature, and suggest future direction and clinical application. Based on the PECO and PRISMA frameworks, we have systematically searched four electronic databases—ScienceDirect, Web of Science, EBSCO, and PubMed. Thirty-two studies that meet the inclusion criteria are further evaluated for quality using the Medical Education Research Study Quality Instrument (MERSQI) and Critical Appraisal Skills Programme (CASP) parameters. Most studies fall in the moderate-to-high quality range. The review critically evaluates the interplay between ACEs and three types of specific NDDs—ADHD, ASD, and cognitive impairments. The findings provide strong empirical confirmation of the consistent bidirectional, cyclical, and dose-response association between the ACEs and NDDs.
Key Message
Shedding a contemporary light on recent evidence, this study focuses on important gaps in the existing literature pertaining to the association of ACEs and NDDs across the developmental trajectory of the individual. There are several promising areas for further study involving high-quality research (quantitative, qualitative, and mixed-methods) to investigate the dynamic and complex interplay between ACEs and NDDs and to design appropriate interventions.
Keywords
Introduction
The issue of adverse childhood experiences (ACEs) has received critical attention in understanding the complexity of neurodevelopmental disorders (NDDs). ACEs are potentially traumatic events comprising various forms of abuse (physical, emotional, and sexual), neglect (emotional and physical), and household dysfunction (family violence, household substance abuse, household mental illness, parental separation or divorce, and household member incarcerated) that a child experiences before 18 years of age.1–5 The original ACE study, which surveyed around 14,000 adults, was the first to demonstrate a graded relationship between the breadth of exposure to ACEs during childhood and later health risks. 5 The prevalence of ACEs is quite alarming, as it is observed in a prevalence study on children (n = 4,90,423) from 18 countries that 58% children experience ACEs (one ACE = 22%, two ACEs = 13%, three ACEs = 8%, four or more ACEs = 15%). 6
NDDs are a constellation of conditions that affect the nervous system and cause developmental deficits, such as attention deficit/hyperactivity disorder (ADHD), autism spectrum disorder (ASD), or intellectual disabilities, affecting social communication, cognition, behaviour, and motor skills. 7 In 2019, a report estimated that approximately 317 million children and young people were disturbed by a range of health conditions resulting in developmental disability. 8 In India, almost one in eight children aged 2–9 has at least one NDD, highlighting a significant public health concern. 9
Several studies have documented that ACEs can disrupt brain architecture, such as the prefrontal cortex, hippocampus, and amygdala.10–12 ACEs can lead to hyperactivation of the hypothalamic-pituitary-adrenal (HPA) axis, resulting in cortisol dysregulation and affects the stress response systems. 13 These neurobiological disruptions result in allostatic load, leading to long-term damage in brain regions that align with the concept of toxic stress theory. 14 Toxic stress can interfere with the normal development of the brain, which increases the risk for stress-related difficulties in adulthood. In view of these findings, it is construed that the presence of ACEs is likely to bring potential threats to the neurodevelopment of individuals with NDDs.
Despite growing empirical support demonstrating the role of ACEs in neurodevelopment, there is little research on their distinct role in the onset, severity, and progression of NDDs, specifically ADHD, ASD, and cognitive impairments. Since ACEs and NDDs often coexist, 15 the purpose of this systematic review is to provide a critical summary of the existing literature on the interplay between ACEs and NDDs (including onset, severity, and progression), to evaluate what is currently known about the interdependency of ACEs and NDDs, to identify the gaps in the literature, and to suggest future direction and clinical application. Thus, through this systematic review, we aim to answer the pertinent question: How does exposure to ACEs increase the acceleration of the manifestation of symptoms of NDDs and deteriorate the behaviour and functioning of the individual throughout the developmental trajectory?
Method
Study Design
To conduct the systematic review, we adopted the PECO (Population, Exposure, Comparison, and Outcome) 16 framework. Using this framework, we defined the four components of PECO: Population (children, adolescents, or adults diagnosed with NDDs and exposed to ACEs), Exposure (Specific ACEs, such as abuse, neglect, and household dysfunction), Comparison (Individuals having NDDs without ACEs exposure), and Outcome (risk of neurodevelopmental outcomes, including onset, severity, and progression of NDDs, specifically ADHD, ASD, and cognitive impairments).
Protocol and Eligibility Criteria
After defining the four components of PECO, we screened the studies according to the guidelines of the preferred reporting items for systematic reviews and meta-analyses (PRISMA).
17
Studies focusing on the interlinking of ACEs and NDDs were included. Studies were considered eligible if they focused on children, adolescents, and adults with NDDs who were exposed to ACEs or if they attributed the ACEs to the onset, severity, and progression of NDDs. We excluded the following studies given below. Focused on the prenatal population Did not focus on direct measurement of ACEs Explored biological mechanisms (epigenetics) and not directly linked to NDDs diagnoses Focused on mental health outcomes, but not NDDs Focused on NDDs, but not directly linked to ACEs
Data Sources and Search Strategies
To identify the relevant studies according to the eligibility criteria, we systematically searched primarily four electronic databases—ScienceDirect, Web of Science, EBSCO, and PubMed. We restricted our search to research articles written in English and published in peer-reviewed journals from January 2016 to April 2025. There was no restriction on document type in the search. We searched these databases primarily using four predefined terms, such as ‘adverse childhood experience AND neurodevelopmental disorder’, ‘adverse childhood experience AND attention deficit/hyperactivity disorder’, ‘adverse childhood experience AND autism spectrum disorder’, and ‘adverse childhood experience AND cognitive impairment’. We used the Boolean operator ‘AND’ to link ACEs and NDDs.
Data Extraction and Selection
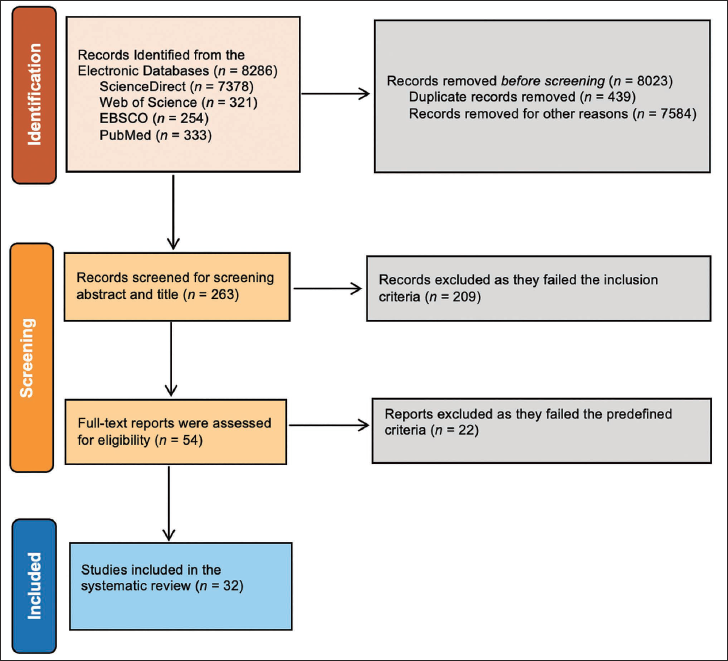
We selected the research articles through two stages for the systematic review. First, the title and abstract of each study were reviewed by three authors as reviewers (RJ, NS, and SR) acting independently in accordance with the predefined eligibility criteria. Second, the full text of the potentially eligible research articles were independently read and thoroughly reviewed by three reviewers to examine whether the research article was eligible for inclusion. When there were disagreements among the reviewers, they discussed together and made a final decision unanimously on the inclusion or exclusion of the research article in the review. Thus, the initial search resulted in 8,286 research articles (ScienceDirect = 7,378, Web of Science = 321, EBSCO = 254, and PubMed = 333). After removing duplicate records and excluding studies that did not align with the research question or lacked accessibility, 263 records were reviewed based on titles and abstracts, and 54 full-text articles were assessed for eligibility based on predefined eligibility criteria. Final, 32 studies met the eligibility criteria to be included in the review. The PRISMA 17 flow diagram depicting the progression from identification to inclusion of these 32 studies is presented in Figure 1.
The PRISMA Flow Diagram.
Results
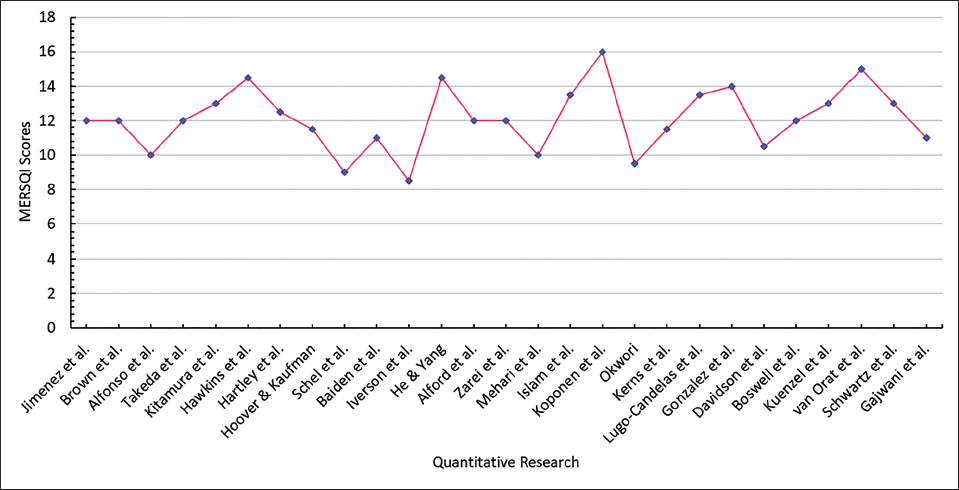
This systematic review included 32 research articles primarily involving two types of studies—quantitative research (n = 26) and review (n = 5)—comprising literature review, narrative review, systematic review, and meta-analysis. One study used a mixed-method approach. The quality of the quantitative studies was assessed using the six parameters of the medical education research study quality instrument (MERSQI), 18 whereas the quality of the review was evaluated through 10 domains of the critical appraisal skills programme (CASP) 19 checklists. In the mixed-method study, the quantitative component was assessed by using MERSQI parameters. The articles were independently evaluated by each of the reviewers and verified by all reviewers to minimise subjectivity and maximise accuracy. Disagreements were resolved through meticulous discussions. The results of the quality assessment of these 32 studies are presented in the form of line graphs in Figures 2 and 3, respectively.
Quality of Included Quantitative Research (n = 27, Including the Quantitative Component of One Mixed-method Study) Assessed Through MERSQI.
Quality of Included Review (n = 5) Assessed Through CASP Checklists.
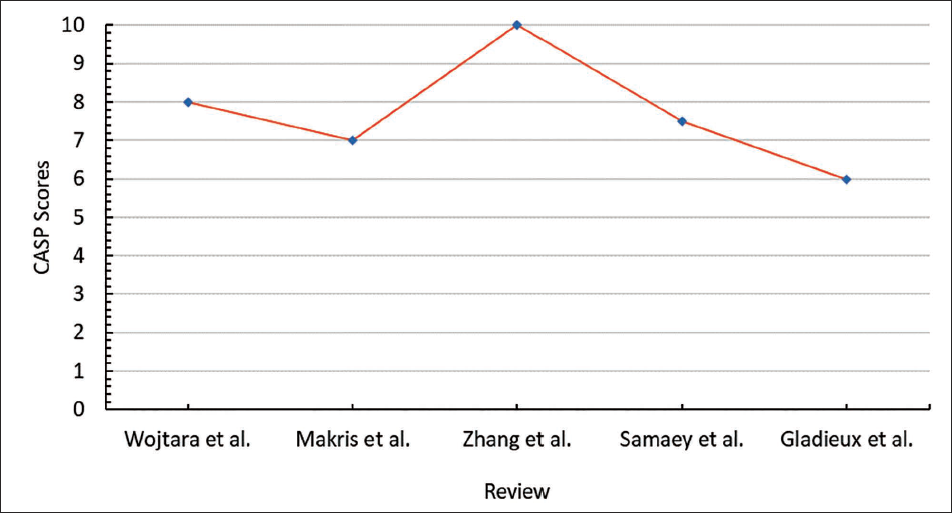
It is evident from the line graphs that among quantitative studies, the study by Koponen et al. obtained the score of 16 out of the maximum score of 18 of MERSQI, whereas among reviews, the study by Zhang et al. received the maximum score of 10 of CASP. However, most studies fall in the moderate-to-high quality range.
The 32 studies (quantitative = 26, mixed-method = 1, review = 5) included in this review were categorised and discussed under two major themes—NDDs and specific NDDs (ADHD, ASD, and cognitive impairments).
Neurodevelopmental Disorders (NDDs)
Among 32 included studies, 10 studies focused on the association between ACEs and NDDs. While a few of the studies mentioned the presence of multiple NDDs, others did not indicate any specific type of NDDs. An overview of these 10 studies examining the association between ACEs and NDDs is presented in Table 1, highlighting the purpose, methods, findings, and quality assessment scores using MERSQI and CASP.
Summary of the Ten Included Studies on NDDs.

*MERSQI Score, #CASP Score.
Studies consistently reported a high incidence rate of ACEs in children with NDDs. A study analysing the data from the National Survey of Children’s Health found that children diagnosed with ADHD or ASD tended to experience ACEs. 20 Similarly, research established a dose-dependent relationship between ACEs and multiple neurodevelopmental outcomes, suggesting that ACEs were significantly associated with ADHD, ASD, and learning disabilities. 15 A survey conducted on children reported no significant relationship between ACEs and neurodevelopmental diagnosis or externalising symptoms, but identified a significant relationship between ACEs and some behavioral outcomes, such as sleep problems or greater functional impairment at home. 21
A longitudinal study of adolescents found that those with fewer ACEs had a reduced risk of developing NDDs. 22 Additionally, a study showed that both ACEs and prenatal substance exposure before birth increased the chances of developing NDDs. Children who faced both ACEs and prenatal substance exposure had the most serious challenges, including delays in learning, managing emotions, and interacting with others. 23 Further, research reported that ACEs on their own could harm children’s health and development, even without other conditions. However, when children had both ACEs and NDDs, the effects were worse, showing the need for better support that could address both issues. 24 A recent cross-sectional study found that there was a high prevalence of ACEs not only in children with NDDs but also in their parents, suggesting intergenerational transmission of adversity. 25
ACEs, like trauma or stress in early childhood, are known to have a significant impact on the development of the brain, including the HPA axis. This pathway regulates the release of stress hormones, such as cortisol. Evidence suggests that early life stress disrupts cortisol levels, which in turn affect brain development. These disruptions are linked to the development of disorders, such as ADHD and ASD. 13 However, ACEs can also lead to physical changes in the brain, including a smaller hippocampus (important for memory and learning) and thinning of the cortex (involved in thinking and decision-making).26, 27 A neuroimaging study using structural magnetic resonance imaging revealed that ACEs were linked with reduced thickness in the rostral anterior cingulate cortex, indicating neural vulnerability to diagnosis. 26 Similar studies observed that higher ACEs scores are associated with reduced left hippocampal volume, indicating a long-term impact of ACEs on memory and cognitive processing. 27 These changes supported how ACEs affected brain alterations.
Specific Neurodevelopmental Disorders (NDDs)
Of 32 included studies, 22 studies relate ACEs with three specific NDDs exclusively, ADHD (n = 9), ASD (n = 7), and cognitive impairments (n = 6).
Attention Deficit/Hyperactivity Disorder (ADHD)
An overview of the nine studies examining the association between ACEs and ADHD is presented in Table 2.
Summary of the Nine Included Studies on ADHD.
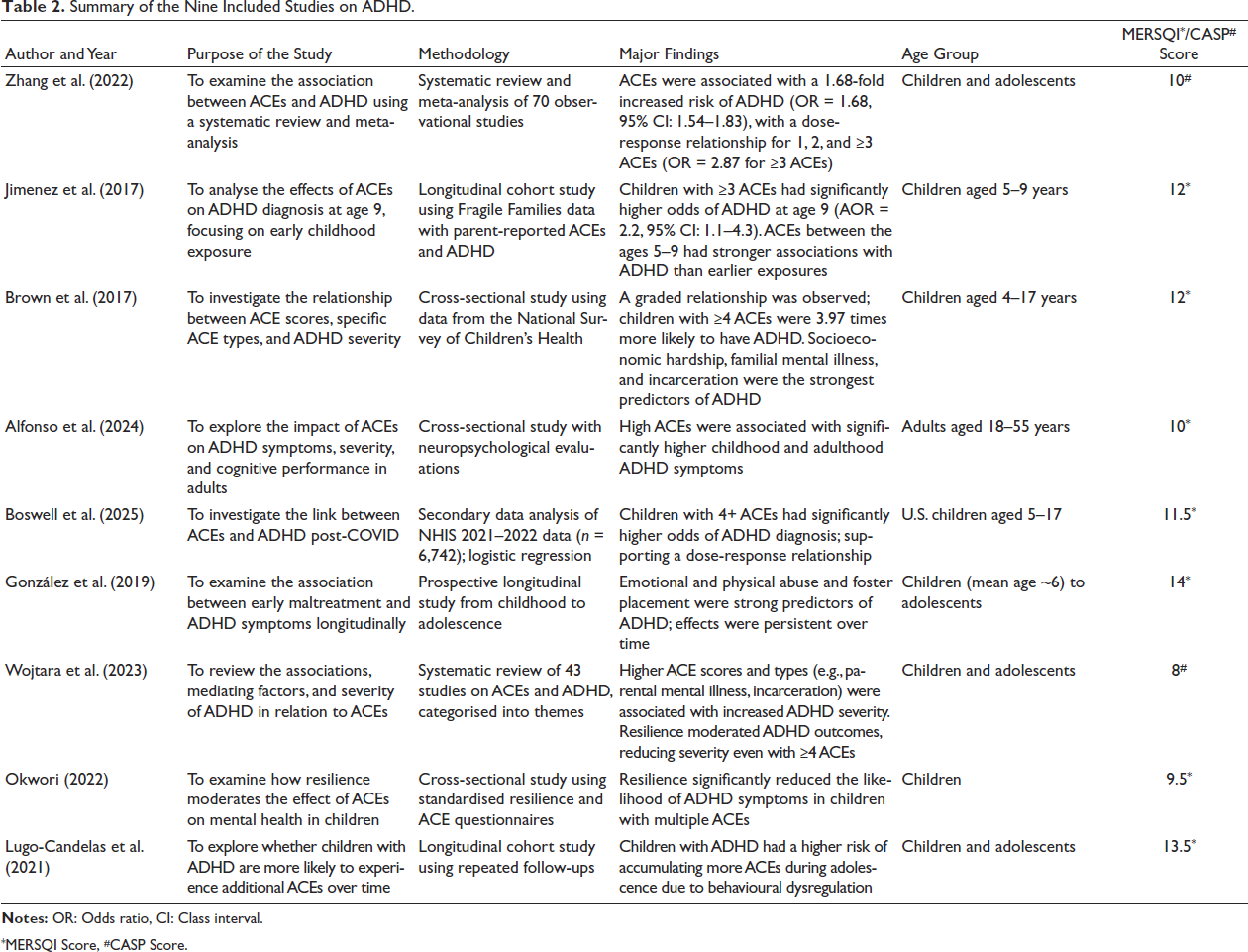
*MERSQI Score, #CASP Score.
Most of the reviewed studies showed a cumulative effect between ACEs and ADHD, indicating that the higher the number of ACEs exposure, the more severe the symptoms of ADHD. A meta-analysis of 70 observational studies involving approximately four million individuals reported a significant association between ACEs and ADHD, one of the specific NDDs. 28 Similarly, children who encountered two ACEs between the ages of five and nine had 110% increased odds of ADHD, and children who experienced three or more ACEs between the ages of five and nine had 120% increased odds of ADHD, resulting in a dose-response relationship. 29 Supporting these findings, further research indicated a strong cumulative relationship showing that children who experienced more than four ACEs had approximately four times increased odds of ADHD compared to those having no exposure to ACEs. 30
Numerous studies have constantly revealed that exposure to ACEs can result in altered brain development, especially in areas such as the prefrontal cortex and hippocampus, the regions that are crucial for emotional regulation and cognitive control. A cross-sectional study found that individuals with higher ACEs exposure reported significantly higher symptoms of ADHD, including impulsivity, inattention, and hyperactivity. 31 Compared to individuals with lower exposure to ACEs, the study mentioned that high exposure to ACEs was associated with greater ADHD symptom severity in both childhood and adulthood, indicating a persistent effect of early adversity on symptom expression across the lifespan. A recent study that analysed children with ADHD in the post-pandemic era observed that children with four or more ACEs had significantly increased odds of ADHD diagnosis, supporting the dose-response relationship. 32 Further, research identified that not all ACEs had the same impact on ADHD. 30 For example, while few studies emphasised emotional and physical abuse, and foster placement as strong predictors of ADHD, 33 others observed parental incarceration to have more impact on ADHD. 34 Moreover, while studies demonstrated an association between the number of ACEs and ADHD prevalence, 35 a bidirectional relationship between ACEs and ADHD was noticed, with an observation that individuals with ADHD were more likely to face additional problems later in life due to impulse control and behavioural challenges. 36
Autism Spectrum Disorders (ASD)
An overview of the seven studies examining the association between ACEs and ASD is presented in Table 3.
Summary of the Seven Included Studies on ASD.
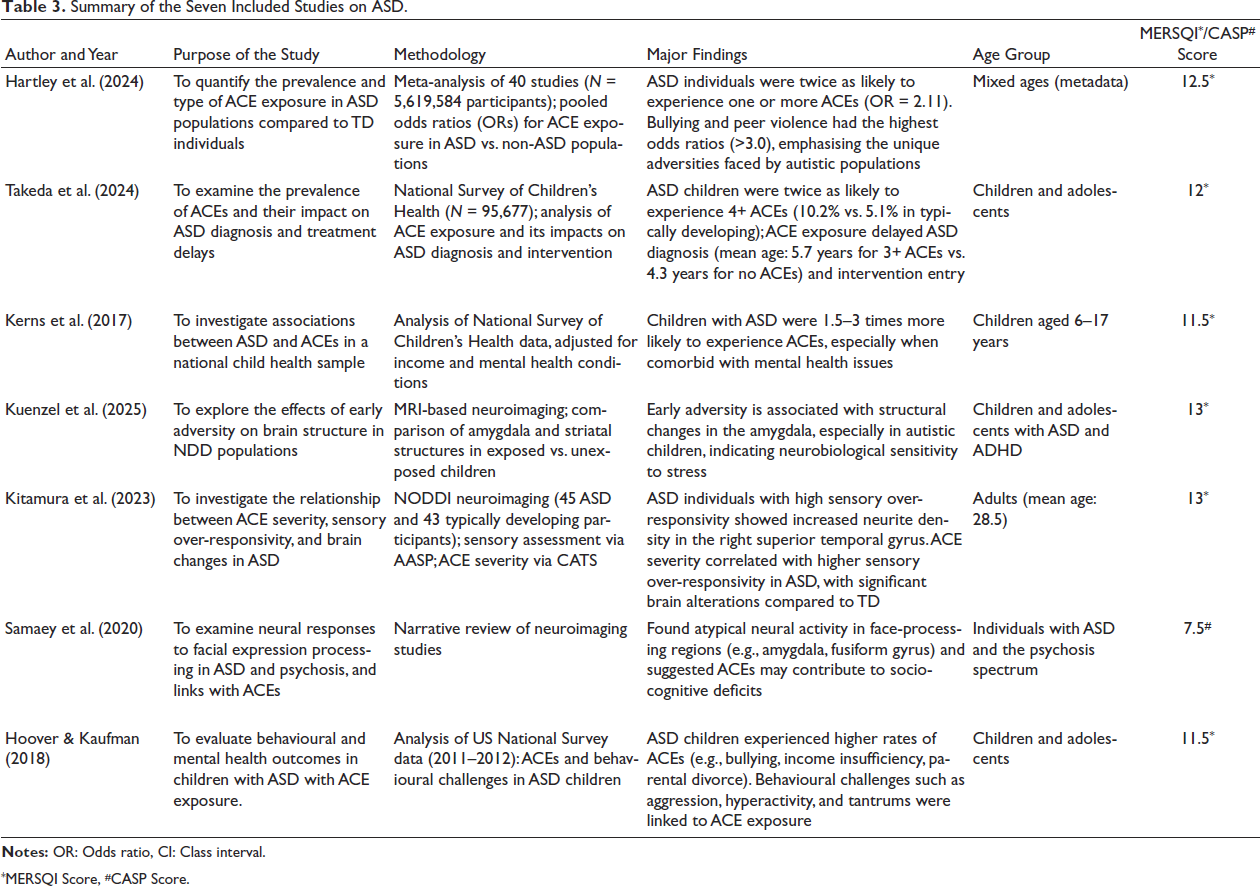
*MERSQI Score, #CASP Score.
According to a meta-analysis, people with autism had twice the likelihood of having at least one ACE as compared to people without autism. 37 Similarly, compared to children who were typically developing, children with ASD had a two-fold higher likelihood of experiencing four or more ACEs. 38 Findings revealed that individuals with ASD had a 1.5 to three times higher likelihood of encountering ACEs compared to their peers. 39 A recent study that examined the brain structure differences identified that early adversity was associated with altered amygdala volume in children with ASD, indicating neurobiological sensitivity to stress. 40 On the other hand, the children who were typically developing did not exhibit any such disturbances. Similar results were found in a study where individuals with ASD who experienced severe ACEs exhibited increased neurite density in the right superior temporal gyrus associated with sensory over-responsivity, suggesting that they were more vulnerable to the effects of ACEs and that they process sensory information (like sounds, lights, or touch) might make the effects of early childhood trauma worse. As a result, they might be more likely to experience changes in the brain, especially in areas that help process sensory information. 41 These changes could affect how they respond to the world around them. Similarly, ACEs contributed to differential neural processing of facial expressions in individuals with ASD, which could accelerate the manifestation of socio-cognitive difficulties. 42 Further research revealed that individuals with ASD who experienced ACEs exhibited higher behavioural disturbances. Evidence suggests that individuals with ASD who experienced severe ACEs were at higher risk for psychiatric comorbidities. 43
Cognitive Impairments
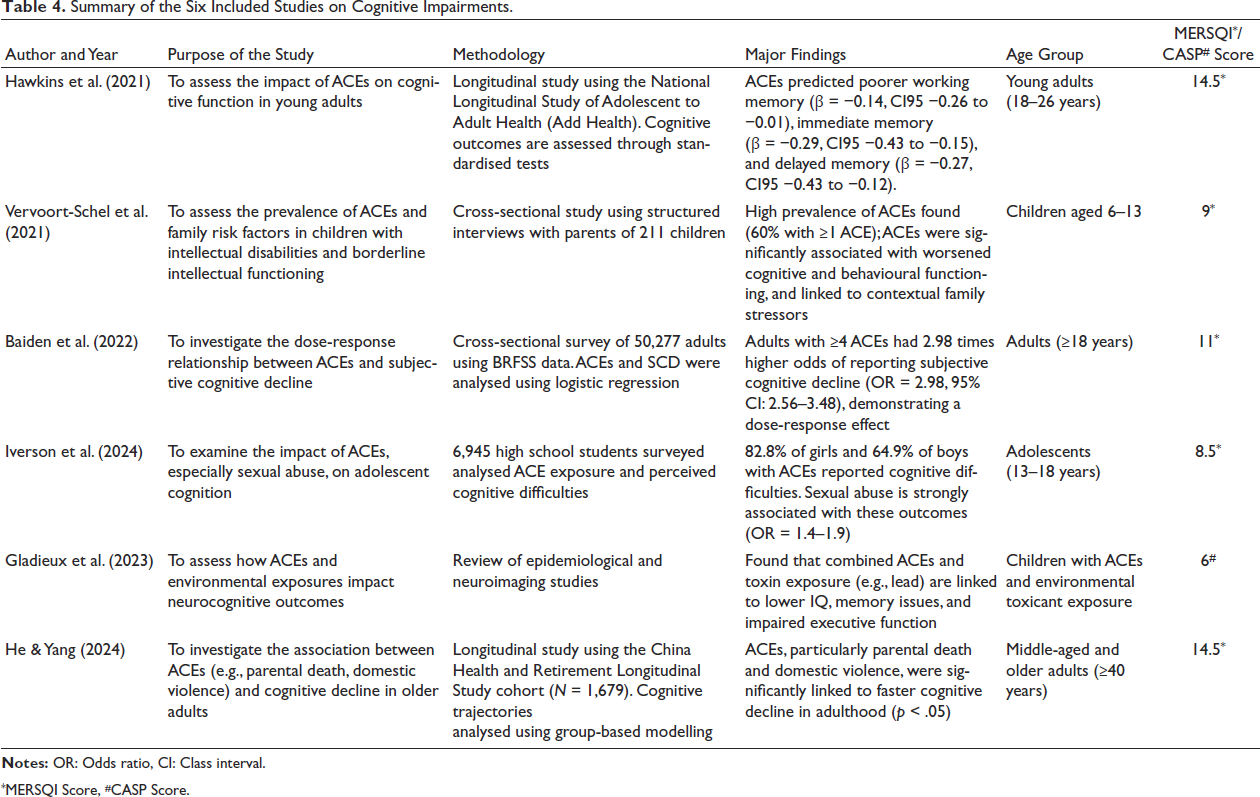
An overview of the six studies analysing the association between ACEs and cognitive impairments is presented in Table 4.
Summary of the Six Included Studies on Cognitive Impairments.
*MERSQI Score, #CASP Score.
In a longitudinal study, it was observed that ACEs were linked with impaired cognitive function, such as delayed memory, lesser working memory, and poorer immediate memory. 44 Similarly, a survey observed subjective cognitive decline in people with ACEs and found a dose-response relationship between the severity of ACEs and subjective cognitive decline. 45 Further, it was noticed that there was a high prevalence of ACEs among children with intellectual disabilities, and ACEs were associated with worsened cognitive effects and behavioural outcomes. 46
A study conducted on high school students had found that a high percentage of girls and boys (82.8% and 64.9%, respectively), who experienced ACEs (especially sexual abuse), reported cognitive difficulties. 47 ACEs, particularly in low socioeconomic status, were associated with a risk of neurocognitive deficits, such as lowered intelligence quotient (up to 6.8 points), memory, and learning difficulties. 48 In a longitudinal study of older adults, it was found that ACEs, such as parental death and domestic violence, were significantly associated with faster cognitive decline. 49
Furthermore, research highlights the significant brain disruptions associated with ACEs. For example, ACEs result in chronic stress, such as hormonal changes and elevated cortisol, leading to hippocampal atrophy as well as disruption in the functioning of the prefrontal cortex, affecting memory and cognition. 44 Similarly, subjective cognitive decline, leading to reduced focus, memory, and mental clarity, disrupts neural networks, including prefrontal-hippocampal connections. 45
Discussion
In the present study, we conducted a systematic review of 32 studies comprising longitudinal studies, cross-sectional research, and neurobiological investigations. The present systematic review reveals an interplay of ACEs and NDDs, suggesting a consistent and dose-response association. One of the significant insights from the review is that the relationship between ACEs and NDDs is not only bidirectional but also cyclical. Children with NDDs tend to experience ACEs due to stigma or a lack of support. Conversely, children exposed to ACEs are more susceptible to developing symptoms that meet clinical criteria for neurodevelopmental diagnoses.36, 41
Neurodevelopmental outcomes, such as attention deficits, hyperactivity, social communication impairments, and executive dysfunction, are commonly reported as a result of the interplay between ACEs and NDDs. Children who experience multiple ACEs are at elevated risk of developing an accumulated burden of adversities and neurodevelopmental disruption.32, 41 The findings also suggest that ACESs have a deleterious impact on the brain, affecting the development of the prefrontal cortex, hippocampus, and amygdala, which are crucial for executive functioning, memory, emotional regulation, and social cognition.50, 51 Furthermore, imaging studies reveal alterations in the structure and function of the brain, particularly in children exposed to persistent adversities. Studies including neuropsychological assessments and cognitive batteries have observed impairments in working memory, attention, and processing speed in children with high ACEs exposure. 44 These impairments are often attributed to the hyperactivation of the HPA axis, which plays a central role in the physiological stress response. 52
While genetic tendencies contribute to the onset of NDDs, 53 the findings of this systematic review indicate that the presence of ACEs acts as an environmental catalyst that accelerates symptom severity and comorbid impairments. This is supported by the findings of a study in which children diagnosed with ADHD have shown a significantly higher prevalence of ACEs exposure and those with four or more ACEs have over three times the odds of ADHD diagnosis compared to those with none. 32 Regarding ASD, we have not come across any substantial evidence of ACEs as the cause of ASD, though children with ASD are observed to be more vulnerable to experiencing adversity.20, 41 Further, the findings of the present review suggest a significant association between cognitive impairments and ACEs exposure. This corroborates the findings of a study where the young adults exposed to ACEs are four times more likely to report cognitive difficulties. 54 However, no link between ACEs and cognitive performance is observed when socioeconomic status and maternal education are controlled. 55
The strength of this systematic review lies in its integration and synthesis of the recent studies from diverse fields, providing a comprehensive examination of the interplay between ACEs and NDDs. It spans multiple types of evidence, including epidemiological surveys, neurobiological studies, systematic reviews, meta-analyses, and longitudinal research to demonstrate a critical understanding of how early adversity shapes neurodevelopmental outcomes. While studying ADHD, ASD, and cognitive impairments, this review aligns with the perspective of developmental psychopathology, highlighting the interaction of biological and environmental risk factors across disorders. 56 Essentially, this review emphasises the biological validity of the link between ACEs and NDDs, supported by neuroimaging and neuroendocrine studies.
The findings of this review have multifaceted clinical implications. Focusing on early screening and diagnosis of ACEs, the findings propose trauma-informed care in developmental settings. Since it is ascertained that ACEs are instrumental in accelerating the manifestation of symptoms of NDDs, early identification of adverse exposures could improve the treatment planning by addressing both ACEs and NDDs. The findings also focus on integrated intervention strategies that combine appropriate therapy in clinical and community settings, supportive services, and community rehabilitation. Further, greater emphasis could be placed on improving access to mental health care, promoting positive parenting, raising awareness on various acts, policies, and laws, and creating safer environments.
The present review has identified important gaps in the existing literature on the interplay between ACEs and NDDs. Through this systematic review, it is observed that the majority of the studies are based on ex-post-facto research, limiting the inferences of causality. We have come across very little experimental research during this systematic review. No significant intervention study has been found in this field. Further, it is observed that there is an absence of consistency and uniformity in the assessment of ACEs. We noticed that there is a wide variation among the parameters of measures of ACEs. Over-reliance on self-report assessment is also observed. Several studies have not specified the specific types of NDDs; rather, they have discussed NDDs as a whole. Many studies have not considered genetic predispositions using genetically sound methodology, such as twin studies and sibling comparisons. For example, a child might have inherited traits, such as impulsivity, which may be more likely to elicit negative caregiving responses, leading to increased ACEs. It is further observed that the studies involving neurobiological aspects appear to suffer from sampling problems and sampling bias as they use small and selective samples primarily from clinical settings. Furthermore, most of the reviewed studies are from Western countries which limits the understanding of the cultural loading of ACEs. Most of the studies have failed to consider the important covariates and contextual factors that may influence the relationship between ACEs and NDDs. Considering all these, the generalisability of much published research on this issue appears problematic. Moreover, there is a critical gap in research to explore the protective and preventive factors for ACEs in individuals with NDDs. However, we have not come across any significant qualitative research depicting the insiders’ perspectives of the individuals with NDDs having exposure to ACEs and their parents or caregivers.
Limitations
Although the present systematic review provides a bird’s-eye view of the critical synthesis of the current literature on the interplay between ACEs and NDDs, there are a few limitations. We have searched for research articles written exclusively in English from peer-reviewed journals indexed in four electronic databases—ScienceDirect, Web of Science, EBSCO, and PubMed. Further, it is observed that studies reporting significant or strong associations between ACEs and NDDs are more likely to be published in such journals. Furthermore, the exclusion of grey literature and non-peer-reviewed studies may limit the comprehensiveness of this review.
Conclusion
This systematic review has been one of the first attempts to thoroughly evaluate the interplay between ACEs and three types of specific NDDs—ADHD, ASD, and cognitive impairments—and provide a basis for further research. The findings provide strong empirical confirmation of the consistent bidirectional, cyclical, and dose-response association between the ACEs and NDDs. Shedding a contemporary light on recent evidence, this study focuses on important gaps in the existing literature regarding the association between ACEs and NDDs across the individual’s developmental trajectory. Thus, there are several promising areas for further study involving high-quality research (quantitative, qualitative, and mixed-methods) to investigate the dynamic and complex interplay between ACEs and NDDs and to design appropriate interventions.
Footnotes
Abbreviations
ACE: Adverse Childhood Experience; ADHD: Attention Deficit/Hyperactivity Disorder; ASD: Autism Spectrum Disorder; CASP: Critical Appraisal Skills Programme; DSM-5: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; HPA Axis: Hypothalamic-Pituitary-Adrenal Axis; MERSQI: Medical Education Research Study Quality Instrument; NDD: Neurodevelopmental Disorder; PECO: Population, Exposure, Comparison, Outcome; PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Acknowledgements
We thank all researchers whose studies we have referred to while conducting the systematic review. Specifically, we express our gratitude to the researchers whose studies we have cited in this article.
Authors’ Contribution
Statement of Ethics
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Not applicable.