
Abstract
Background
Parkinson’s disease (PD) is a neurodegenerative disorder that affects both motor and non-motor functions of the body. Recently, scientists have attributed that gut dysbiosis plays a crucial role in the development and progression of PD.
Purpose
In this study, we aim to determine the role of probiotic supplementation on gut dysbiosis, inflammatory responses at the systemic level, neurodegeneration and motor deficits.
Methods
To develop a rat model of PD, 6-hydroxydopamine was bilaterally injected into the striatum. Starting from the first week after surgery, probiotics were administered orally for a period of four weeks. In this study, 18 rats were randomly divided into three groups (n = 6 each): the sham group, the PD group and the PD + Probiotics group. Motor function was measured using paw print analysis, while non-motor function was assessed through gastric emptying. Neuronal survival was evaluated with cresyl violet staining, and blood-based biomarkers were measured to assess inflammation. General body conditions, including body weight, food intake and water intake, were monitored daily.
Results
Probiotic supplementation significantly improved body weight, food intake, water intake and gastric emptying, along with improving gait. Additionally, probiotic supplementation reduced neuronal loss in the brains of PD rats. There was also a reduction in inflammatory markers, such as interleukin-6 and glutaminase, along with an elevation in brain-derived neurotrophic factor levels in the serum. This study is the first to demonstrate the beneficial effects of probiotics in improving motor deficits and gastric emptying in a PD model.
Conclusion
Our findings suggest that probiotic supplementation has the potential to slow down PD progression by preventing gut dysbiosis and neurodegeneration.
Introduction
Parkinson’s disease (PD) is the second most prevalent non-communicable neurological disorder, 1 characterised by the loss of dopamine neurons in the substantia nigra pars compacta. 2 The number of patients with PD in India is approximately 1.2 million, representing a prevalence of 1%–1.5% among those over 65 years of age, according to a report by the Parkinson’s Disease and Movement Disorder Society. While L-Dopa and cholinesterase inhibitors may slow the progression of this incurable disease,3, 4 other symptoms, such as a decline in non-motor functions, 5 an increase in gastrointestinal (GI) problems 6 and systemic inflammatory response,7, 8 tend to worsen. Thus, finding new interventions to mitigate non-motor or systemic symptoms associated with PD is a pressing need.
PD manifests with various motor symptoms, such as muscle rigidity, akinesia and resting tremor, 9 as well as non-motor symptoms, including GI manifestations (e.g., abnormal salivation, delayed gastric emptying, etc.)6, 10, 11 and chronic inflammation, such as heightened neuronal oxidative stress and elevated concentrations of interleukin-6 (IL-6) and tumor necrosis factor (TNF) in the bloodstream. 12 These symptoms exert a substantial adverse effect on the overall quality of life. 13
The healthy flora of the intestinal microbiota maintains blood–brain-barrier (BBB) integrity. 14 Dysbiosis of the microbiome can compromise barrier integrity through endotoxin formation, which initiates inflammatory pathways. 15 Recent evidence demonstrates that dysbiosis of gut microbiota correlates with the severity of PD in both motor and non-motor functions.16, 17
Probiotic supplementation has the ability to prevent neurodegeneration 18 by protecting gut flora. 18 In PD rats, probiotic intervention not only decreased dopaminergic neuronal loss 19 and inflammatory cytokines (e.g., IL-6) but also increased antioxidant activity, mitochondrial function and locomotor activities.18, 20, 21 A randomised controlled trial on PD patients demonstrated that probiotic intervention improved gut functions and the expression of immunoregulators.22, 23 However, the mechanisms by which probiotics act on the enteric nervous system (ENS) to improve gut functions in PD remain unknown. Therefore, the present study aimed to evaluate the mechanism of action of probiotics in improving motor and non-motor symptoms in the early stages of a 6-hydroxydopamine (6-OHDA) lesion rat model of PD.
Methods
Animals
Male albino Wistar rats (270–320 g) were procured from the Central Animal Facility, All India Institute of Medical Sciences (AIIMS), New Delhi. They were housed individually in polycarbonate cages in the Department of Physiology and had ad libitum access to food pellets (Ashirwad Industry, India) and clean water. Temperature (22°C–26°C), humidity (50%–55%) and 14:10-h light–dark cycle were kept constant throughout the study. All experiments were approved by the Institutional Animal Ethics Committee of AIIMS (282/IAEC/1-2021).
Experimental Design
The rats were randomly divided into three groups with n = 6 in each group: (a) Group 1—vehicle injection (0.2% ascorbic acid in the striatum, sham group); (b) Group 2—6-OHDA injection in the striatum (PD group); and (c) Group 3—6-OHDA injection in the striatum and oral probiotics (PD + Probiotics).
6-OHDA PD Model
PD was induced by injecting 6-OHDA into the striatum. To reduce respiratory tract secretions during surgery, each animal received an injection of glycopyrrolate (25 mg/kg body weight). After a 5-minute interval, anaesthesia was induced via intraperitoneal injection of thiopentone at a dosage of 50 mg/kg of body weight. Rats were then positioned in a stereotaxic apparatus (Model-1404, David Kopf Instruments, USA) using coordinates from the rat brain atlas by Paxinos and Watson, with bilateral lesions targeted at coordinates anterior/posterior: +0.2 mm; medial-lateral: ±3.2 mm; ventral/dorsal: −5.5 mm. Bilateral lesions were induced by infusing 2 µL of 6-OHDA (7.5 µg/µL in 0.2% ascorbate saline) at a rate of 1 µL/min using a Harvard Nanomite pump. The syringe remained in place for 5 min before being slowly withdrawn. Desipramine was administered intraperitoneally at a dose of 20 mg/kg body weight 30 min prior to the 6-OHDA infusion to protect other monoamine neurons from damage. After the surgery, the incision was closed with sutures, and appropriate postoperative care was administered. 24
Probiotic Intervention
Oxxyslab (EOS2021, Ardea, Italy), containing a mixture of the following probiotic strains, Streptococcus thermophilus DSM 32245, Bifidobacterium lactis DSM 32246, Bifidobacterium lactis DSM 32247, Lactobacillus acidophilus DSM 32241, Lactobacillus helveticus DSM 32242, Lactobacillus paracasei DSM 32243, Lactobacillus plantarum DSM 32244 and Lactobacillus brevis DSM 27961 (each 5.4 × 106 CFU), was used in the study.
General Health Assessment
Rats were observed daily, and their body weight, food intake and water intake were noted down one week before surgery and thereafter weekly. General health and gross motor function were assessed by observing in-cage behaviour and during brief, gentle handling to check for rigidity (hunched posture and increased tail tone), bradykinesia (slowed movement and/or absence of rearing), dystonia (clenched paws), autonomic signs (piloerection), abnormal thermoregulation and signs of dehydration (dry mucous membranes or tenting skin).
Assessment of Motor and Non-motor Function
Gait
Gait was analysed using footprint patterns (walking tracks). It was a three-day experiment, with the first two days allotted for training and the last day for recording. The rat’s paws were coated with non-toxic ink/dye (red and blue colour ink for fore and hind paws, respectively) and were allowed to walk along a brightly lit narrow alley (100 cm long with 20 cm side walls) leading to a dark goal box of 20 × 20 × 20 cm. Three footprints, present in the central region of the alley, excluding those close to the entry point and the goal box, were considered for analysis of stride length, step length, step width and overlap between hindpaw and forepaw of both right and left sides.24, 25
Solid Gastric Emptying
Following a 12-h fast, rats were allowed free access to food for 1 h. Two hours later, rats were sacrificed, and the stomach contents were flushed and weighed. Food was weighed before and after the feeding period to confirm equal consumption between groups. 26 Results were normalised to body weight.
ELISA Assay
Blood samples collected in BD Vacutainer vials were left for 30 min at 2°C–8°C and then centrifuged at 1000 × g for 15 min under 4°C. The straw-coloured serum from the upper layer of the preparation was collected, kept as an aliquot and preserved at −20°C until use for determining biochemical parameters. The levels of different blood biomarkers, namely brain-derived neurotrophic factor (BDNF), IL-6, ALS and glutaminase (GLS), in serum were measured by Enzyme-Linked Immunosorbent Assay (ELISA) kits according to the manufacturer’s instructions.
Nissl Staining
Following anaesthesia with thiopentone (50 mg/kg), rats were sacrificed, and their brains were removed and stored in 4% paraformaldehyde solution at 4°C overnight. Subsequently, the brains were processed in a graded sucrose solution for 48 h. The specimens were rapidly frozen, and 14-µm-thick coronal sections were prepared using a cryostat. Cresyl violet (Nissl) staining was performed to assess normal and pyknotic cells in the striatum. The coronal sections of the brains were stained with 1% cresyl violet, dehydrated in a graded series of ethanol, immersed in xylene and mounted on DPX. Finally, the pyknotic and normal cells were evaluated. Neurons were observed using an optical microscope at ×400 magnification (Nikon, Japan) and analysed with ImageJ.
Statistical Analysis
Two-way ANOVA followed by Tukey’s post hoc test was used to analyse the effects of treatment and time on body weight, food intake, water intake and paw print analysis. To study intergroup variation at week 5 after surgery, one-way analysis of variance (ANOVA) was used. The differences in the mean values of blood-based biomarkers and gastric emptying were compared using the Kruskal–Wallis test. The results are presented as mean (M) ± standard deviation (SD). The data were analysed using GraphPad Prism 8, and differences were considered significant when P ≤ .05.
Results
Changes in Body Weight, Food Intake and Water Intake in 6-OHDA Rats
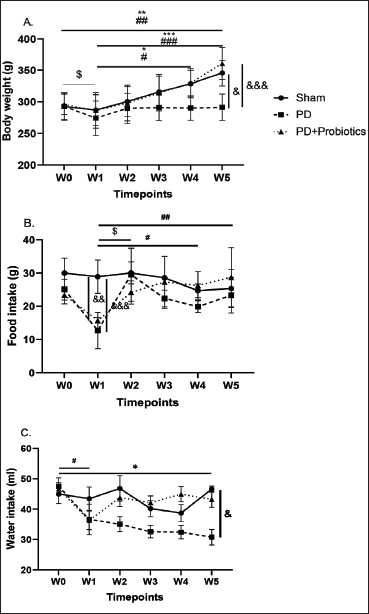
Two-way ANOVA unveiled significant treatment effects (F(2,90) = 13.38, P < .0001) and time effects (F(5,90) = 10.35, P < .0001) on body weight. Tukey’s post hoc analysis revealed significant weight gain in sham (P ≤ .001) and PD rats receiving probiotics (P ≤ .001) at week 5 after surgery compared to week 1 and baseline. Intergroup comparison at week 5 showed significant loss of weight in PD rats compared to sham and PD + Probiotics (P = .015 and P = .0003, respectively) (Figure 1A).
Similarly, two-way ANOVA demonstrated significant treatment effects (F(2,90) = 12.30, P < .0001), time effects (F(5,90) = 6.771, P < .0001) and interaction effects of time and treatment (F(10,90) = 3.535, P = .0006) on food intake. Post hoc analysis showed a decrease in food intake at week 1 in PD (P < .0001) and PD + Probiotics (P = .0022) rats compared to baseline. However, in PD + Probiotics rats, food intake increased gradually over the weeks and was significantly higher at week 5 (P ≤ .01) compared to week 1 (Figure 1B).
Tukey’s post hoc analysis showed a significant decrease in water intake in the PD group only at week 5 (P = .024) compared to the sham group (Figure 1C).
Gait Analysis
The paw print analysis was conducted to assess gait before 6-OHDA injection (baseline) and at one and 5 weeks post-lesion.
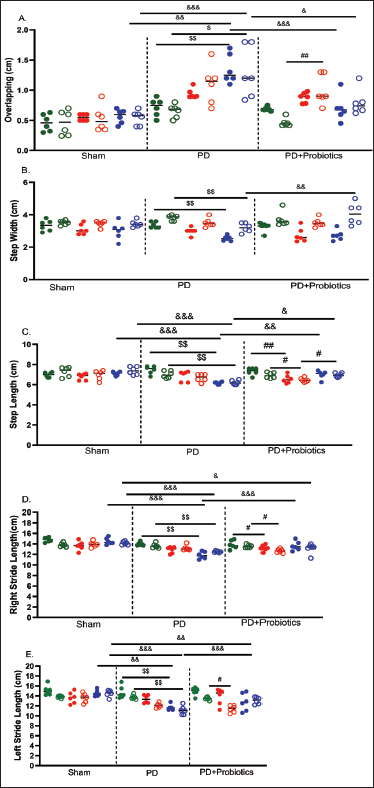
A two-way ANOVA highlighted significant effects of treatment (F(2,45) = 20.41, P < .0001), time (F(2,45) = 13.09, P < .0001) and a treatment × time interaction (F(4,45) = 3.165, P = .0225) on right overlap. Tukey’s post hoc analysis revealed a notable increase in PD (P = .0016) at week 5 compared to baseline. An increase in right overlap in PD rats was also observed in comparison to sham (P = .006) and PD + Probiotics (P < .001) in the 5th week. Similar results were recorded in left overlapping (Figure 2A).
A two-way ANOVA highlighted a significant time effect (F(2,45) = 13.03, P < .0001) on step width. Tukey’s post hoc analysis revealed a decrease in forepaw (P = .0027) and hindpaw step width (P = .0117) in PD rats after five weeks of surgery compared to baseline. Additionally, one-way ANOVA showed a decreased hindpaw step width in PD rats compared to PD + Probiotics (P = .0095) at week 5 (Figure 2B).
A decrease in forepaw (P = .0016) and hindpaw (P = .0281) step length was observed in PD + Probiotics after one week of surgery (P = .0016). However, it gradually improved with the administration of probiotics, and by week 5, hindpaw step length had increased significantly compared to week 1 (P = .02), whereas both forepaw (P = .0027) and hindpaw (P = .0016) step lengths decreased in the PD group at week 5 compared to baseline. A significant decrease was also evident in the PD group for both forepaw and hindpaw step lengths compared to the sham (P ≤ .0001) and PD + Probiotics (P ≤ .05) groups at week 5 (Figure 2C).
A two-way ANOVA revealed significant effects of treatment (F(2,45) = 20.18, P < .0001), time (F(2,45) = 11.71, P < .001) and a treatment×time interaction (F(4,45) = 4.985, P = .0021) on the right stride length. Post hoc analysis indicated a decrease in forepaw (P = .0016) and hindpaw stride length (P = .001) in PD rats after five weeks compared to baseline. Intergroup comparison at week 5 showed a decrease in forepaw (P ≤ .0001) stride length in PD rats compared to sham and PD + Probiotics, whereas hindpaw stride length decreased only in comparison to sham (P ≤ .0001) (Figure 2D). Similar results were observed for the left forepaw and hindpaw stride length (Figure 2E).
Effect of Probiotics in Gastric Emptying
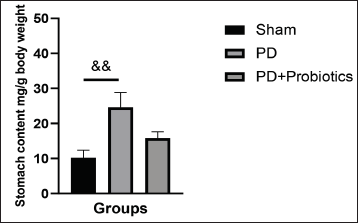
6-OHDA lesioned PD rats had higher residual stomach content two hours after a meal, indicating a significant delay in solid gastric emptying compared to sham (P = .0088) (Figure 3). Following probiotics intervention, a trend for a decrease in stomach content was evident.
Blood-based Biomarkers
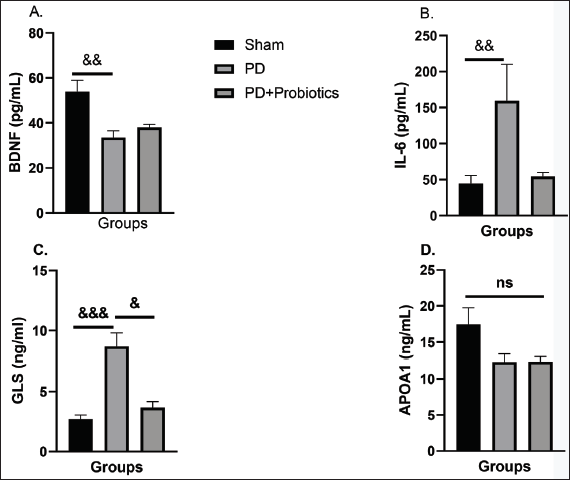
To delve deeper into the mechanisms underlying the neuroprotective effects of probiotics, we examined their impact on various blood-based biomarkers. ELISA results revealed a decrease in BDNF levels (P = .008) and increased concentrations of IL-6 (P = .001) and GLS (P = .0008) in PD rats compared to sham rats. Intervention with probiotics reversed these effects, significantly reducing GLS levels (P = .046) and IL-6 concentrations in PD + Probiotics rats, which were comparable to those in the sham group. We assessed lipid metabolism in PD rats by examining apolipoprotein A1 concentration. Although there were no significant differences in lipid metabolism, we noticed a tendency for decreased levels in both PD and PD + Probiotics rats compared to the sham group (Figure 4A–D).
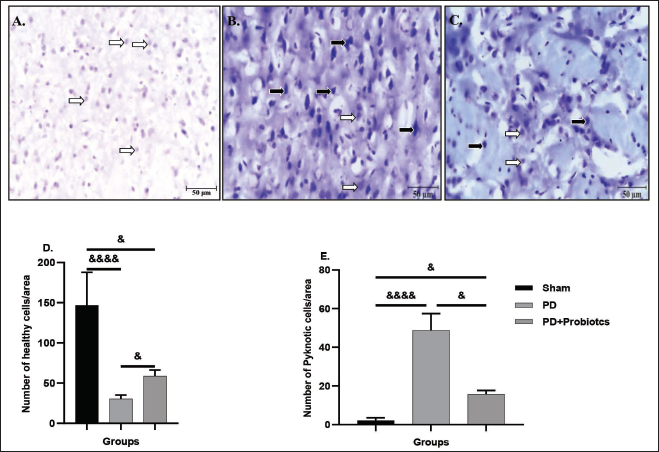
Effect of Probiotics on Neuronal Damage
The number of Nissl-stained cells was assessed. Figure 5A–C presents representative examples of Nissl staining across all studied groups. The number of healthy cells in the striatum of the PD group was significantly reduced compared to both the sham group (P < .0001) and the PD + Probiotics group (P = .0483) (Figure 5D). Additionally, increased pyknotic cells were observed in the striatum of the PD group, unlike in the sham group (P < .0001). However, in the PD + Probiotics group, the number of pyknotic cells was significantly lower compared to the PD group (P = .0478) (Figure 5E).
Discussion
In the present study, probiotics showed restoration of functional alterations caused by neurotoxin (6-OHDA)-induced PD, characterised by bilateral lesions of the nigrostriatal system. We observed that bilateral microinjection of 6-OHDA into the striatum region led to reduced body weight, food intake and water intake, altered gait, decreased gastric emptying, increased inflammation, GLS activity and increased neurodegeneration. Interestingly, the administration of probiotics to these rats significantly ameliorated these effects. These findings underscore the potential therapeutic benefits of probiotics in mitigating both the symptoms and underlying pathophysiology of PD.
Changes in the gut microbiome are increasingly recognised as influential factors in various neurological conditions. Reports indicate that GI symptoms, including constipation, dysphagia, hypersalivation and swallowing disorders, coupled with gut dysbiosis and leaky gut, precede symptoms of autism, anxiety, depression and PD by 5–10 years.27, 28 Impairment of the intestinal barrier allows bacterial translocation across tight junctions into the mesenteric lymphoid tissue, triggering mucosal immune cell activation and the release of inflammatory cytokines, along with vagal nervous system activation. 29 These events may lead to the release of neuroactive peptides that impact the central nervous system (CNS) and ENS.30, 31 Patients often experience GI symptoms such as constipation and bloating well before the onset of PD’s motor symptoms, suggesting a potential role for gut inflammation and α-synuclein deposition in the ENS, initiating a process that spreads via vagal and glossopharyngeal nerve trunks to the CNS.32, 33 Studies have shown that alterations in microbiota composition in PD patients, including reduced abundance of Prevotellaceae and increased Enterobacteriaceae, are associated with postural instability and gait disorders. 34 Further evidence supports the role of gut dysbiosis in PD pathogenesis, with microbial species from PD patients showing distinct profiles compared to healthy controls, suggesting potential therapeutic avenues targeting the gut microbiome. Studies conducted in Japan also highlighted the role of specific bacteria role in exacerbating PD symptoms, emphasising the intricate relationship between gut microbiota and neurological health. 35
The gut microbiota presents a promising avenue for PD treatment, with research on the Mediterranean diet, probiotics and faecal microbial transplantation showing significant potential. Probiotics, non-viable components with health benefits linked to microbiota modulation, offer a novel therapeutic strategy. 36 Several studies have indicated efficacy of probiotics in alleviating Parkinson’s GI symptoms, particularly constipation and abdominal discomfort.37, 38 Yet, the precise mechanisms and safety remain unclear, though potential mechanisms include symptom relief, inflammation inhibition, antioxidant stress reduction and neuronutrition.39, 40 Further research is needed to elucidate the role of probiotics in PD management.
The Restoration of Body Weight, Food Intake and Water Intake
Our findings reveal significant reductions in body weight, food consumption and water intake in the rat model of PD compared to the sham group. These observations are consistent with previous studies indicating weight loss and decreased appetite and thirst in PD patients.41–43 The disruption in the basal ganglia-thalamocortical circuit, involving the striatum, globus pallidus, thalamus and cortex, can lead to impairments in appetite regulation, food intake and water intake. 44 Notably, administering a consortium of probiotics resulted in significant improvements in increasing body weight, albeit with partial improvement in food intake and water consumption. These results are in line with prior research showing increased body weight following probiotic administration in rotenone 45 and 6-OHDA-induced PD rat models.46, 47 Some studies have suggested that increased food intake after probiotic intervention may be due to the production of satiety hormones, 48 while others have reported no impact of probiotics on food intake in normal rats49, 50 and in 6-OHDA-induced PD rats. 46 Additionally, one study did not observe any effect of probiotics on water intake. Weight loss in PD can complicate motor symptoms. 51 We evaluated motor symptoms by assessing gait patterns and noted the beneficial effects of probiotics on these aspects.
Improved Gait Functions
In our study, the PD rat model exhibited reduced stride length and increased paw overlap, resembling the motor symptoms commonly observed in PD patients, such as bradykinesia and postural instability. 52 These gait disturbances are associated with the degeneration of dopaminergic neurons in the substantia nigra, resulting in impaired coordination and movement control. 53 Remarkably, administering probiotics significantly improved gait balance in our PD rat model, which echoes the findings of previous studies. They noted augmented stride length and limb gap after an 8-week intervention with Lactobacillus salivarius initiated six weeks post-6-OHDA lesion. In 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP)-induced PD models, probiotic intervention led to elongated stride length. 54 A 15-day probiotic intervention in LPS-induced rats also yielded improved gait compared to PD rats. 55 Moreover, one study noted an increase in step and stride length alongside a decrease in step width after a 16-week probiotic intervention. This modulation of motor behaviour could potentially be attributed to the neuroprotective impact of probiotics on dopaminergic neurons and the expression of tyrosine hydroxylase in the substantia nigra, 56 as well as in the striatum. Additionally, it might involve the elevation of dopamine levels in the brain. 54
Easing Gastric Emptying and Prevention of Inflammation
Our investigation revealed a significant delay in gastric emptying in the PD rat model, indicating disruptions in GI motility. 26 This delayed gastric emptying is a well-documented feature of PD and can contribute to various GI symptoms, such as bloating, constipation and early satiety.6, 57, 58 Moreover, our model exhibited heightened levels of inflammatory markers, including increased levels of pro-inflammatory cytokines like IL-6. These findings are consistent with emerging evidence implicating neuroinflammation through the activation of microglia and astrocytes, alongside enhanced expression of IL-6 and TNF in the brains of PD patients. 59 Probiotic supplementation demonstrated improvements in gastric emptying and inflammation by alleviating IL-6, nuclear factor-κB and TNF, possibly through their anti-inflammatory properties, facilitation of gut–brain communication and modulation of the gut microbiota.47, 60 A three-strain Lactobacillus capsule was found to be safe, and the outcomes offered preliminary evidence suggesting its potential benefits on gastric emptying among healthy adults aged 40 and above. 61 However, the findings from Ohtsu et al.’s (2021)62 study did not provide sufficient evidence to confirm the positive impact of Lactobacillus gasseri OLL2716 on delayed gastric emptying, possibly due to a limited sample size.
While prior research has demonstrated impaired gastric emptying in PD rats compared to controls,6, 26 no study has yet elucidated methods for its restoration. Our current investigation indicated that this combination of probiotic strains aided in restoring gastric emptying.
Decreased BDNF and Increased GLS
Our investigation revealed a notable reduction in BDNF levels within the PD rat model, potentially exacerbating PD pathogenesis through the impairment of neuroplasticity and synaptic function. 63 Furthermore, heightened GLS activity was observed in PD rats, consistent with prior findings linking GLS dysregulation to PD-related glutamate excitotoxicity. 64 Notably, although probiotics did not produce a significant change in BDNF levels, they did alleviate GLS activity. This contrasts with prior studies, such as the one by Srivastav et al., 54 where pretreatment with a probiotic blend in an acute MPTP-induced PD model resulted in elevated levels of BDNF in the brain. Reduced GLS activity may protect dopaminergic neurons and, in turn, alleviate motor symptoms.
Prevention of Neurodegeneration
In the present study, a significant increase in pyknotic cells was observed in the striatum of PD rats. However, in the group treated with probiotics, the number of pyknotic cells significantly decreased compared to the PD group. This reduction in neurodegeneration may be attributed to decreased systemic inflammation, as previously suggested by Alipour Nosrani et al. 21 They observed nuclear vacuolation and pyknosis, along with increased oxidative stress, in a 6-OHDA rat model, where the Probiotics group exhibited significantly reduced pyknosis and oxidative stress.
Conclusion
In summary, our study demonstrates that probiotic intervention significantly impacted various pathologies of PD, encompassing alterations in body weight, food intake and water intake, as well as gait balance. These effects may be attributed to a reduction in inflammation, neurodegeneration and an improvement in gastric emptying. Our findings underscore the multifaceted nature of PD and elucidate its various pathological aspects. Specifically, our research revealed significant changes in the PD rat model, including decreased body weight, food intake and water intake, alongside gait imbalance, delayed gastric emptying, increased inflammation, increased neurodegeneration, decreased BDNF levels and elevated GLS activity. These findings highlight the complexity of PD and its impacts on the diverse physiological systems. Moreover, the reversal of these pathological effects following probiotics administration suggests their potential as a therapeutic approach in PD management. However, further investigations are necessary to fully elucidate the long-term effects and clinical feasibility of probiotics in treating PD. Continued research in this area is essential to validate and refine the potential of probiotics as a viable therapeutic strategy for PD patients.
Abbreviations
BBB: blood–brain barrier; BDNF: brain-derived neurotrophic factor; GLS: glutaminase; IL-6: interleukin-6; PD: Parkinson’s disease
Footnotes
Acknowledgements
The authors express their gratitude to the team at the Cognitive Neurophysiology Laboratory and the Nanomedicine and Neurophysiology Laboratory, Department of Physiology, AIIMS Delhi, for their assistance throughout this study. We also acknowledge the financial grant provided by the Department of Science and Technology, Government of India, during this period.
Authors’ Contribution
S.S.: Planned the work, analysed and interpreted the data and wrote the manuscript. S.J.: Assisted in planning the experiments and supervised the entire work and analysis. R.C.: Assisted with the surgical procedures and conducted behavioural tests. R.C.: Contributed to writing the manuscript. T.C.N.: Assisted with histological studies and image analysis. E.A.: Assisted in data analysis. D.M.R.: Contributed to planning the experiments, data analysis and interpretation. S.P.: Contributed in the statistical analysis. S.D.: Helped in writing the first draft of the manuscript. V.D.M.: Assisted in data analysis and contributed to writing the manuscript. K.P.K.: Conceived the main idea of the work, supervised the entire project and contributed to writing the manuscript.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Cognitive Science Research Initiative, Department of Science and Technology (DST/CSRI/2017/33) and Innovation in Science Pursuit for Inspired Research, Department of Science and Technology (DST/INSPIRE/03/2021/000408).
ICJME Statement
We declare that this article has been prepared in accordance with the ICMJE guidelines.
Patient Consent
Not applicable.
Statement of Ethics
The study received approval from the Institutional Animal Ethics Committee (Ethical number: 282/IAEC/1-2021) and was conducted in compliance with the Laboratory Animals Welfare Act, the National Institutes of Health’s Guide for the Care and Use of Laboratory Animals (Bethesda, MD, USA) and the EU Directive 2010/63/EU on animal experiments.