
Abstract
Background
College students face stressors like academic workload, competition, time management and financial concerns, which affect their psychological, physiological and cognitive functions. Meditation techniques can help mitigate these challenges.
Objective
The study aimed to investigate the influence of the Mind Sound Resonance Technique (MSRT), a meditation method, on cognitive functions and psychophysiological variables among college students.
Methods
Fifty experienced yoga practitioners (aged 19–30 years, with 30 of them being female) participated in a randomised controlled study. The subjects were split into two groups at random: the meditation group (n = 25) and the supine rest (SR) group (n = 25). Participants in the meditation group underwent one month of MSRT training, whereas those in the SR group rested supine for the same amount of time. Self-reported psychological assessments and the Stroop-colour word test were collected at baseline and after one month of intervention. On both days (day 1 and day 30), a continuous electrocardiogram (ECG) was also recorded for heart rate variability (HRV) at rest (pre-task), during task and post-task.
Results
The MSRT group exhibited significant changes in HRV at baseline, during the Stroop task and post-task conditions, along with significant cognitive and psychological changes. The study found significant differences in cognitive tasks [accuracy rate (P < .05), reaction time (P < .05)] and HRV (P < .05) between the MSRT and SR groups. No significant change was observed in the SR group.
Conclusion
MSRT appears to have the potential to enhance cognitive and psychophysiological functions in college students. In this regard, MSRT may be implemented to alleviate the effects of stressful environments and improve the overall well-being of college students.
Introduction
The student population is a unique group that is passing through a challenging period of their lives. 1 It is a very important milestone in a student’s life to enter college or university. They experience many stressful events during this time. 2 As education progresses to a higher level, students face more stressful events such as substantial studying, an extensive academic course load, assignments and projects, competition in the classroom, time management, financial concerns, familial pressures and adjusting to a new environment.3, 4
Studies have shown that in the past decade, college students reported experiencing psychological distress, depression and anxiety. Surveys show that 65% of Australian tertiary students experienced high or very high distress, while 35% had self-harm or suicide thoughts. 5 Asian countries have shown an increase in rates of depression (29.4%), anxiety (42.4%) and stress (16.4%) compared to other regions. 6
Research shows that college students experience stressors that may indicate their risk of developing mental health issues. 4 Many detrimental outcomes, such as social distancing, difficulty concentrating in class, attendance issues and incomplete assignments might result from poor mental health. This may result in lost opportunities and, ultimately, a diminished sense of self-worth.7, 8 Studies have clearly shown that behavioural patterns, mental illnesses and unfavourable psychological variables might impact cardiovascular health. 9 When there are issues with the body’s automatic functions and heart health, cognitive abilities decrease. 10 Prolonged stress can cause changes in the body’s automatic functions, like increased cortisol levels and a shift in the balance of the body’s stress response systems.11, 12
Heart rate variability (HRV) is often used as a marker for overall health, with lower HRV indicating higher levels of stress and potential heart issues. 13 Therefore, it is essential to measure the HRV to evaluate physical and mental health. 14 By addressing stress and mental health issues early on, individuals can prevent long-term consequences on their physical health and overall well-being. Taking steps to reduce stress, such as practising mindfulness, exercise and seeking therapy, can greatly improve both mental and physical health outcomes. 15
Mind Sound Resonance Technique (MSRT) is one of the sound-based meditation techniques that use mantra to generate resonance, which is used to induce deep relaxation for mind and body. 16 The practice of MSRT has been shown to positively influence various aspects of mental and physical well-being. 17 Additionally, it has been demonstrated to reduce blood pressure, heart rate, stress, anxiety and depression, while also enhancing self-esteem in both clinical and non-clinical populations.18, 19 Studies have also reported that MSRT decreases state anxiety, improves psychomotor performance and boosts cognitive functions, such as sustained attention and information processing speed.20, 21 Despite these promising findings, the relationship between psychophysiological changes and mental health remains underexplored. Thus, the present study aims to evaluate the impact of a one-month MSRT practice on HRV, cognitive performance and its relation to mental health among college students. This research seeks to fill the gap by examining how psychophysiological changes induced by MSRT can contribute to overall mental well-being. We also hypothesised that one month of MSRT practice may improve HRV, cognitive performance and mental well-being.
Methods
Participants
A total of 50 participants (30 female), 19–30 years with a mean age of 23 ± 3.3 years were recruited from a yoga university in Bangalore. The sample size was calculated using ‘G Power Software 3.1.9’ based on the previous study
22
using the congruent score of the Stroop test with effect size 0.59; power 0.95 and alpha-value 0.05. The calculated sample size was 40 but due to possible dropout, we considered 50 samples. Participants were enrolled in the study from September 2021 to March 2022. Recruited participants were randomly allocated into two groups, that is, MSRT (n = 25; 14 female) and supine rest (SR) (n = 25; 16 female) using
Characteristics of Participants
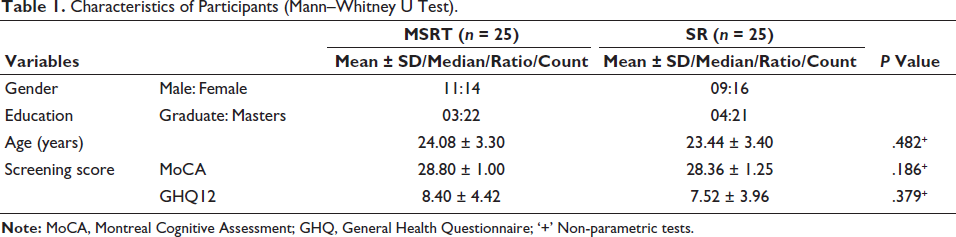
Table 1 shows the demographic data of the recruited participants in the present study. There were 50 participants (30 females) age group of 19–30 years.
Characteristics of Participants (Mann–Whitney U Test).
Design of the Study
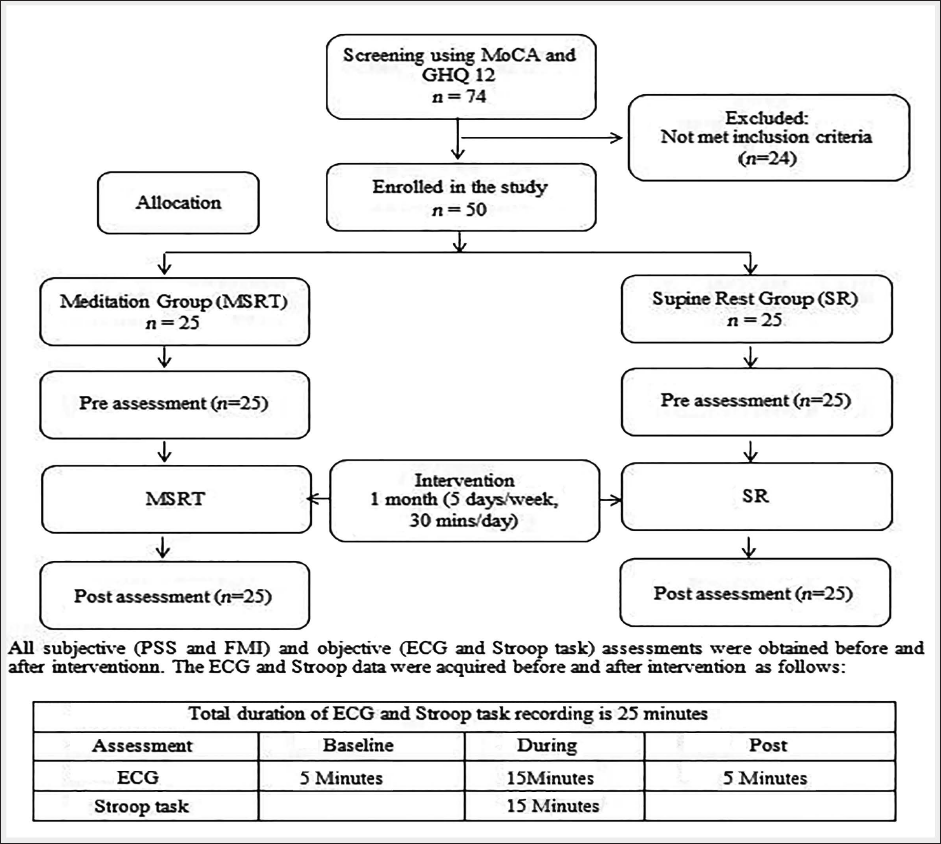
The study employed a randomised controlled trial (RCT) design. The experimental procedures are depicted in Figure 1. Participants attended the laboratory on two distinct occasions and participated in the pre-test on day 1 and the post-test following a one-month intervention.
The Schematic Presentation of Participants’ Recruitment and Experimental Protocol.
Intervention
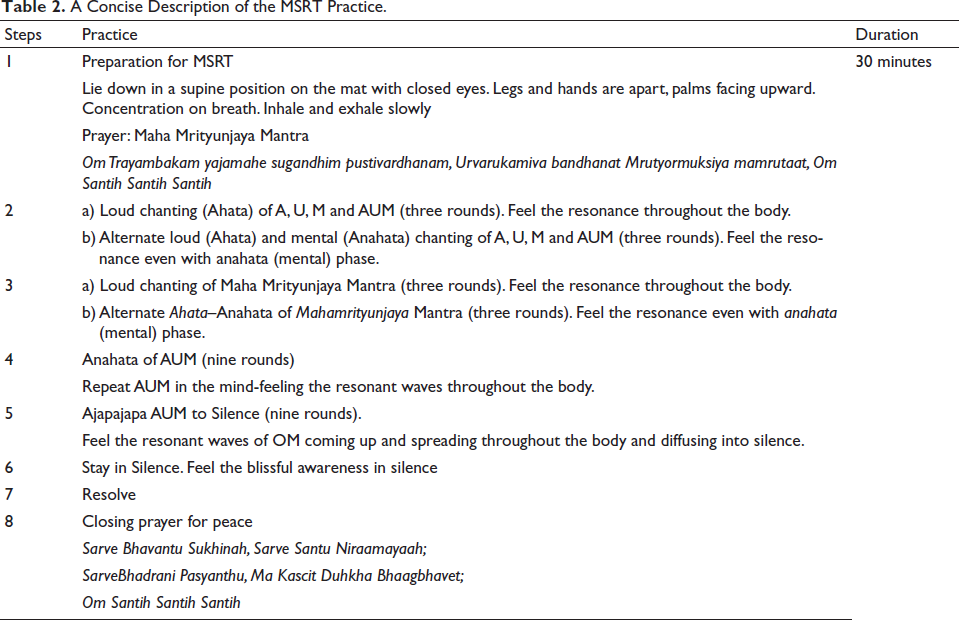
The intervention was conducted over one month (five days/per week and for 30 minutes/day) and the time of each intervention was the same. The practice of MSRT has been mentioned in Table 2.
A Concise Description of the MSRT Practice.
The SR group were asked to lie down on their back with closed eyes 26 legs and hands apart and keep observing their breath for the entire session for 30 minutes. They were instructed to lie down on their back, legs and hands apart with closed eyes and keep observing their breath for the entire session. They practised SR for five days/week for one month. An experienced teacher was allocated to supervise the sessions. All subjects, regardless of their group allocation, were advised to follow their routine day-to-day schedule and not practice at home to maintain homogeneity of intervention.
Procedure
All assessments were acquired in the Cognitive Neuroscience laboratory of the S-VYASA Deemed to be University. The demographic information (age, education, MoCA, GHQ) was obtained on the first day of administering the task. Participants were advised to have a good sleep and avoid drinking anything with caffeine on the previous day of recording. Before the data acquisition participants were instructed to sit upright throughout the session on a comfortable chair in front of a 21-inch LCD monitor kept at a 70 cm distance in a light-dampening and sound-attenuating chamber where the temperature was maintained around 24.0°C ± 1.0°C. After fixing the instruments the continuous assessment was processed during pre-tasks, Stroop tasks and post-tasks; during which continuous electrocardiogram (ECG) recordings were also acquired. The recording was done at 5.30
Cognitive Assessment (Stroop Task)
The computerised Stroop task was used in this study including three experimental conditions: neutral, congruent and incongruent.27, 28 Each block lasted between 2–4 minutes and was interspersed with 60-second resting blocks. Overall, there were three experimental task blocks (one neutral, one congruent and one incongruent) and two resting blocks, for a total length between 8–14 min. In total, there were 60 neutral trials (Block 1), 60 congruent trials (Block 2) and 60 incongruent trials (Block 3). All trials began with a fixation cross for 1.5 seconds, and all visual stimuli appeared in the centre of the computer screen for 2.5 seconds. Participants responded with two fingers (index and middle finger) from each of their hands on the response pad. In the neutral block, participants were instructed to respond based on names of colours (RED/BLUE/GREEN) visualised in white colour with a black background. In the congruent block, participants were asked to respond based on name words (RED/BLUE/GREEN) visualised in the same colour (e.g., RED printed in red colour). In the incongruent block, participants were asked to respond by seeing the colour of ink (RED/BLUE/GREEN) where the visualised word was different from the actual colour (e.g., the word RED was presented in blue). Before the actual task, participants were given practice blocks of 12 trials for each condition. Participants were instructed to press the numeric key on the keyboard for responses (i.e., one for RED, two for GREEN and three for BLUE).
The incorrect responses were not used for further analysis (i.e., for response accuracy [RA] and Reaction Time). Further >90% accuracy was considered for the final analysis. The percentage of the correct responses was used for RA, and the average value of the time was taken for response time (RT). 29
Heart Rate Variability
HRV refers to the variation between consecutive heartbeats. HRV is regulated by the sympathetic and parasympathetic nervous systems as well as other controls, and thus, HRV serves as a quantitative indicator of the heart’s autonomic control (European Society of Cardiology and American Society of Pacing and Electrophysiology). The ECG was assessed throughout a session that lasted 25 minutes (pre-tasks, during Stroop task and post-task) using a 16-channel polygraph system (MP 100 BIOPAC, AcqKnowledge software, BIOPAC System Inc., USA). As part of the ECG recording process, Ag/AgCl pre-gelled electrodes were used (Tyco Healthcare, Germany) and the standard limb lead II configuration was used. Offline analysis of the data was performed using a 1024 Hz sampling rate. For analysis, noise-free data was included.
Perceived Stress Scale
Cohen’s perceived stress scale (PSS) is a valid and reliable tool to measure perceived stress. 30 It is the most widely used psychological instrument for measuring the perception of stress. Perceived stress was assessed using the PSS-10 version. It consists of 10 questions, each having five responses. The time given to perform this test was 5 minutes. Each response was given a score of 0, 1, 2, 3 and 4. Total perceived stress was determined by the sum items: 1, 2, 3, 4R, 5R, 6. 7R, 8R, 9, 10 (items 4, 5, 7 and 8 are considered reversing scores before calculating sum items; e.g., 0 = 4, 1 = 3, 2 = 2, 3 = 1 and 4 = 0). The maximum score is 40. 31 The normative scores for PSS-10 are 14.52–16.51 where a score of 20 or above is considered as stress. 32 The effect size of this study is 0.013.
Freiburg Mindfulness Inventory
The Freiburg Mindfulness Inventory (FMI) (Walach et al, 2006) is a short form and is intended to measure the general factor of mindfulness. This scale is more appropriate for use in the general population and participants without any theoretical knowledge of mindfulness, or meditation experience. 33 Though the short version of FMI does not measure any of these facets, it still covers all aspects of mindfulness. Items included ‘I am open to the experience of the present moment’ and ‘I am impatient with myself and with others’. 34 Testing procedure FMI is a condensed version, consisting of 14 items and is highly correlated with the long version. It is rated on a 4-point Likert scale with answer options ranging from 1 to 4. The answer options are as follows: 1-rarely, 2-occasionally, 3-often and 4-almost always. The participant is asked to answer as best as he/she can. The total score was calculated by adding all the scores on the 14 items of the FMI. Item 13 is reversed scored, as it is worded negatively in the FMI-14. Higher scores indicate higher levels of mindfulness. For the FMI-14, a negative correlation was observed with anxiety and depression which is entirely due to the Acceptance factor of mindfulness. 35 FMI has good internal consistency with Cronbach α = 0.86. The correlation of this short form with the long 30-item version is r = 0.95. Reliability is alpha = 0.86. 34 The effect size of this study is 0.052.
Data Extraction
ECG was recorded during three states, that is, (a) pre-task, (b) during task (Stroop) and (c) post-task. The ECG data was extracted using AcqKnowledge 4.1 and Kubios HRV Software 2.2. Before analysis, the acquired data were visually reviewed offline, and only noise-free data were considered for further analysis. The Fast Fourier Transform (FFT) was used to obtain the HRV power spectrum. The following HRV variables were studied in frequency domain measures: (a) low frequency (LF) band (0.05–0.15 Hz), (b) high frequency (HF) band (0.15–1.50 Hz) and (c) the LF/HF ratio. The LF and HF band values were expressed as normalised units. The following components of time domain HRV were analysed: (a) MeanHR (number of heart beats per minute), (b) mean RR interval (the mean of the intervals between the instantaneous heart rate), (c) SDNN (the standard deviation of the IBI of normal sinus beats is measured in ms, (d) RMSSD root mean square of successive differences between normal heartbeats. Due to poor signal quality in the ECG waveform, the data of one participant from the MSRT group and one participant from the SR group were rejected during extraction. Data from 48 participants (MSRT, n = 24; SR, n = 24) was carried out for further analysis.
Data Analysis
The Shapiro–Wilk test was used to check the normality of the data. Baseline data of the MSRT and SR groups were compared using an independent sample t-test or Mann–Whitney U test based on normality. Within-group changes were assessed using paired t-test or Wilcoxon Signed rank test. Analysis of Covariance (ANCOVA) was applied to find the differences in the post-intervention values between MSRT and SR groups by controlling for baseline differences. Pearson’s correlation analysis was performed to check the association between HRV, cognitive tasks and psychological variables. IBM SPSS version 21.0 (IBM Corporation, USA), and JAMOVI version 2.6.19 were used for statistical analysis.
Results
Cognitive Variables
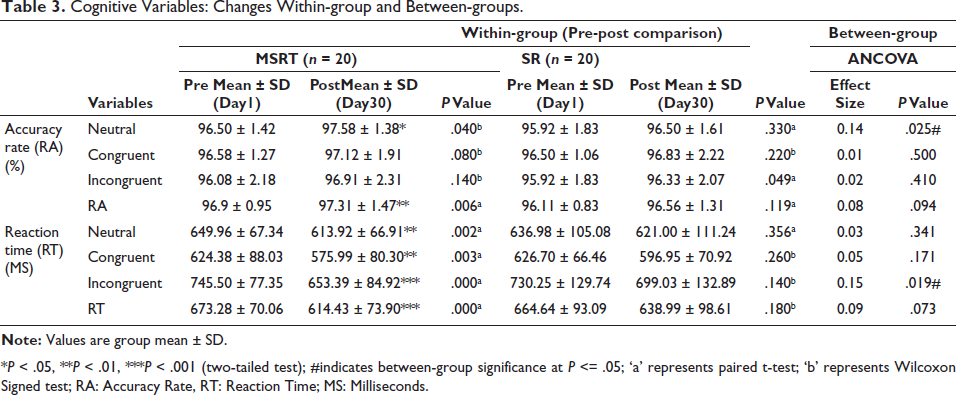
The pairwise comparison of the Stroop task for reaction time (RT) between pre and post-intervention in the MSRT group showed a significant decrease in neutral with a mean difference of −36.04, 95% CI [15.07, 57.00] (P = .002), Congruent with a mean difference of −48.39, 95% CI [18.93, 77.85] (P = .003), Incongruent with a mean difference of −92.11, 95% CI [63.19, 121.03] (P = .000), and RT with a mean difference of −58.85, 95% CI [36.10, 81.59] (P = .000). Similarly, the pairwise comparison of the Stroop task for accuracy rate (RA) between pre and post-intervention in the MSRT group showed a significant increase in neutral condition with a mean difference of 1.08, 95% CI [0.00, 0.94] (P = .040), RA with a mean difference of 0.41, 95% CI [−1.54, −0.30] (P = .006). No significant difference was found in the SR group either in accuracy, or reaction time. Between-group (MSRT/SR) analysis shows a significant difference in accuracy during the neutral task with an effect size of 0.14 (P = .025); in reaction time during the incongruent task with an effect size of 0.15 (P = .019) shown in Table 3.
Cognitive Variables: Changes Within-group and Between-groups.
Note: Values are group mean ± SD.
*P < .05, **P < .01, ***P < .001 (two-tailed test); #indicates between-group significance at P <= .05; ‘a’ represents paired t-test; ‘b’ represents Wilcoxon Signed test; RA: Accuracy Rate, RT: Reaction Time; MS: Milliseconds.
Heart Rate Variability
Pairwise comparison indicated a significant changes in MSRT group for ‘pre-task’ condition between pre and post-intervention, MeanHR with a mean difference of −3.24, 95% CI [−6.00, −0.49] (P = .023), LF/HF ratio with a mean difference of −0.25, 95% CI [0.00, 0.06] (P = .000), LFnu with a mean difference of -3.64, 95% CI [−6.15, −1.12] (P = .006), HFnu with a mean difference of 3.95, 95% CI [0.55, 7.35] (P = .025); during Stroop task condition, MeanRR with a mean difference of 54.15, 95% CI [2.95, 105.36] (P = .039), MeanHR with a mean difference of −4.276, 95% CI [−7.35, −1.20] (P = .008), LFnu with a mean difference of −4.43, 95% CI [−7.54, −1.31] (P = .007), HFnu with a mean difference of 5.00, 95% CI [1.21, 8.79] (P = .012); and during post-task condition, MeanRR with a mean difference of 58.23, 95% CI [13.83, 102.64] (P = .012), MeanHR with a mean difference of −3.43, 95% CI [−6.67, −0.19] (P = .039), LFHF ratio with a mean difference of −0.41, 95% CI [0.00, 0.06] (P = .000), LFnu with a mean difference of -6.54, 95% CI [−9.37, −3.69] (P = .000), HFnu with a mean difference of 4.83, 95% CI [1.34, 8.33] (P = .009). No significant within-group difference was found in the SR group during the pre-task condition shown in Table 4, the Stroop task shown in Table 5, and the post-task condition shown in Table 6. Between-group (MSRT/SR) analysis shows a significant difference during post-task in MeanRR with an effect size of 0.34 (P = .012); MeanHR with an effect size of 0.23, P = .044; and LFnu with an effect size 0.28 (P = .024); HFnu with effect size 0.22, P = .048 shown in Table 6.
Heart Rate Variability: Changes Within-group and Between-groups During Pre-task Condition.
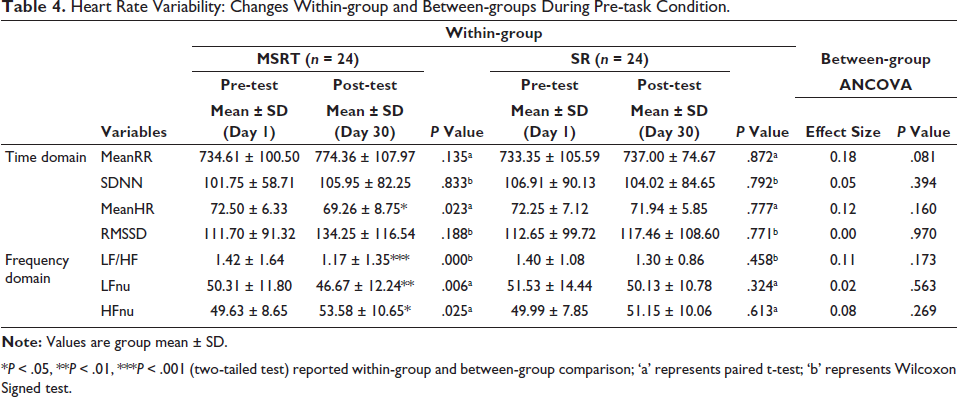
*P < .05, **P < .01, ***P < .001 (two-tailed test) reported within-group and between-group comparison; ‘a’ represents paired t-test; ‘b’ represents Wilcoxon Signed test.
Heart Rate Variability: Changes Within-group and Between-groups During Cognitive Task (Strop) Performance.
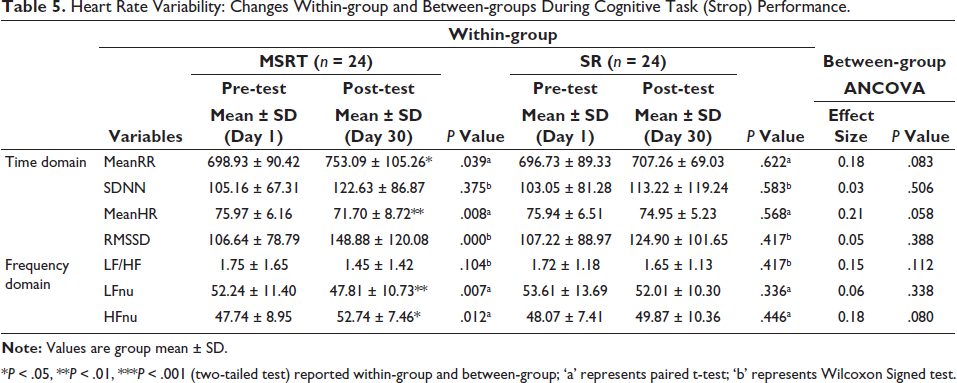
*P < .05, **P < .01, ***P < .001 (two-tailed test) reported within-group and between-group; ‘a’ represents paired t-test; ‘b’ represents Wilcoxon Signed test.
Heart Rate Variability: Changes Within-group and Between-groups During Post-task Condition.
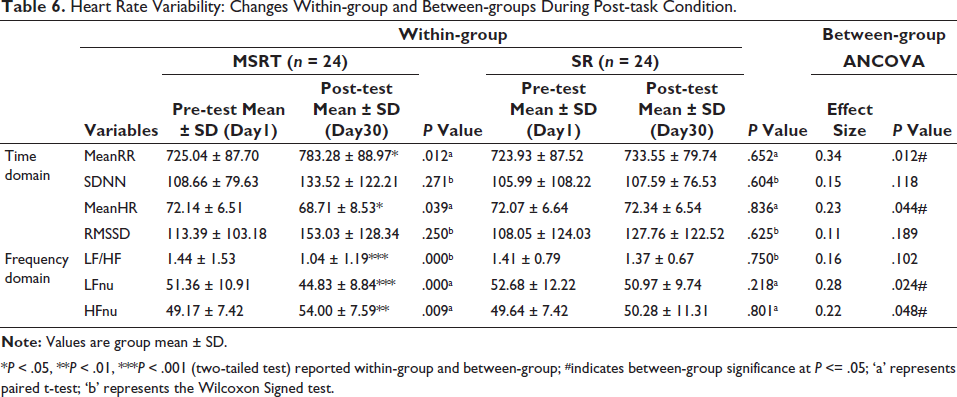
*P < .05, **P < .01, ***P < .001 (two-tailed test) reported within-group and between-group; #indicates between-group significance at P <= .05; ‘a’ represents paired t-test; ‘b’ represents the Wilcoxon Signed test.
Self-assessment Psychological Variables
The pairwise comparison of self-reported psychological variables between pre- and post-intervention in the MSRT group showed a significant decrease in PSS with a mean difference of −1.04, 95% CI [0.15, 1.93] (P = .024), and a significant increase in FMI with a mean difference of 2.60, 95% CI [0.00, 0.06] (P = .003) in post compared to baseline. We did not find any significant difference in the SR group shown in Table 7.
Psychological Variables: Changes Within-group and Between-groups.
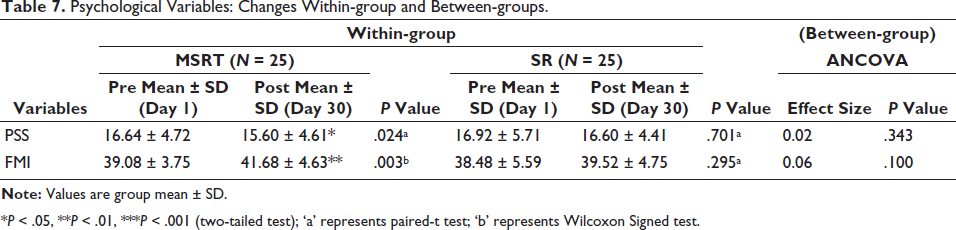
*P < .05, **P < .01, ***P < .001 (two-tailed test); ‘a’ represents paired-t test; ‘b’ represents Wilcoxon Signed test.
Correlation
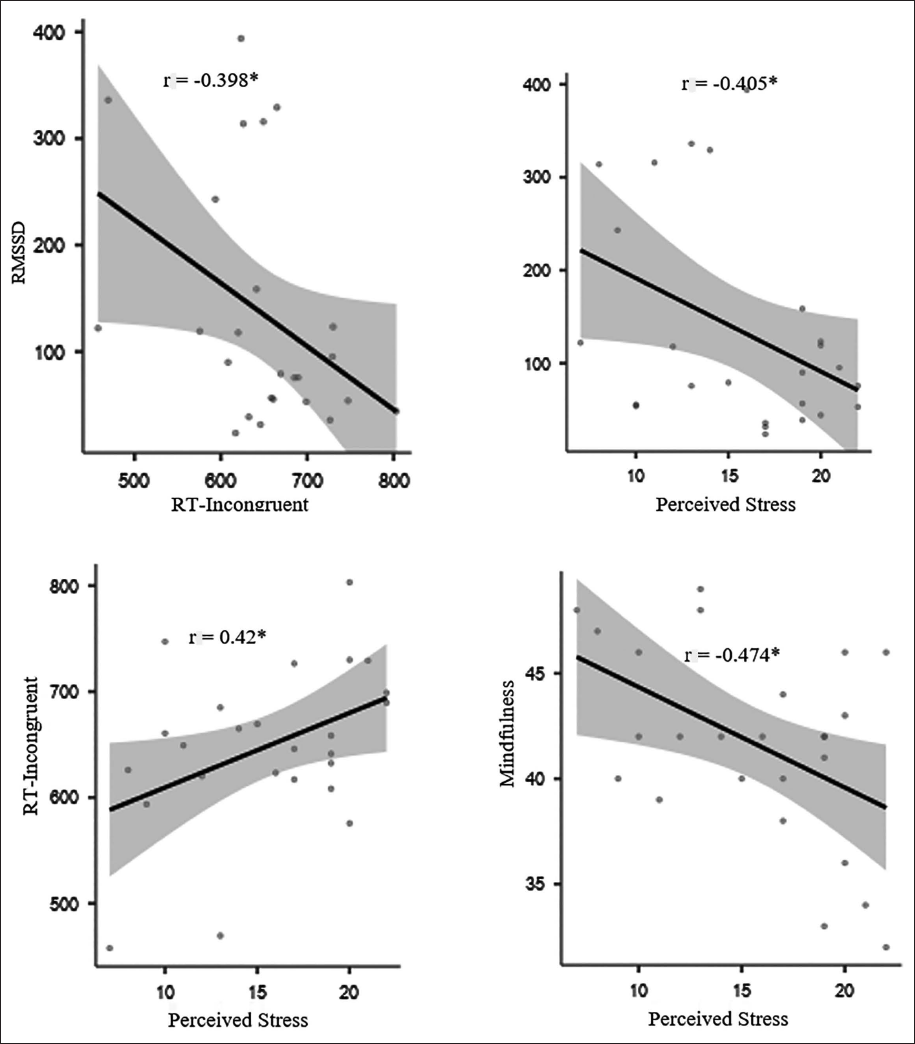
Pearson’s correlation has shown a negative relationship between RMSSD with reaction time (incongruent) (r = −0.398; P < .05) and perceived stress (r = −0.405; P < .05). It has been observed that reaction time (incongruent) is positively correlated with perceived stress (r = 0.042; P < .05). Similarly, psychological parameters showed a negative correlation of mindfulness with perceived stress (r = 0.474; P < .05) shown in Figure 2.
Pearson’s Correlation Between Psychophysiological Parameters.
Discussion
The purpose of the current study was to determine how the MSRT affected psychological outcomes, cardiac modulation utilising HRV, and cognitive performance, particularly executive function as measured by the Stroop-colour word test. The results imply that MSRT practice greatly increases the speed and accuracy of cognitive processing, especially when it comes to tasks involving attention and conflict resolution—two essential executive function components. Reaction times significantly decreased in the Stroop test under neutral, congruent and incongruent conditions. This indicates that following the intervention, cognitive processing accelerated, with the most notable improvement observed in the most cognitively taxing condition. Because the meaning and colour of a word might conflict, the incongruent state necessitates a higher cognitive burden.36, 37 This shows that managing cognitive conflict, a crucial component of executive functioning was one area in which the MSRT intervention was very successful in helping participants. The executive functions test results after MSRT practice show improvements in participants’ attention control, cognitive flexibility and inhibitory control. Previous studies have shown that meditation, including MSRT, can enhance brain regions responsible for conflict monitoring, such as the anterior cingulate cortex (ACC)38, 39 supporting the finding that MSRT improves conflict resolution.
The drop in mean HR after MSRT practice aligns with the well-documented calming effects of meditation and other mindfulness techniques on the autonomic nervous system (ANS). A lower HR typically reflects a state of relaxation and reduced sympathetic (stress-related) activity, which correlates with enhanced parasympathetic (rest-and-digest) function. 40 Research on yoga and meditation practices has consistently found reductions in HR following interventions, indicating improved autonomic regulation and reduced physiological arousal. 41 Such reductions are also indicative of a lower baseline stress level, supporting the idea that MSRT helps foster a calmer state, even before engaging in cognitively demanding tasks. The autonomic responses of the MSRT group members were better during the Stroop exercise. The longer intervals between heartbeats shown by the rise in Mean RR suggest that meditation assisted individuals in maintaining a calmer state even when faced with cognitive strain.42, 43 Participants in the MSRT group may have had lower heart rates throughout the cognitive test due to a decrease in mean heart rate during the task. This might indicate greater cardiovascular control and less physiological arousal. The alterations in LFnu and HFnu imply that MSRT increased parasympathetic activity and decreased sympathetic responses even in the presence of cognitive stress. This suggests that by fostering physiological relaxation and lowering stress reactivity, meditation may assist people in managing difficult cognitive tasks more effectively. A meta-analysis by Pascoe et al (2017) reported that yoga and meditation significantly improve HRV and parasympathetic functioning. 44 Increased HRV is commonly associated with stress resilience and enhanced self-regulation, making it a valuable indicator of overall physiological health.
The MSRT group continued to show better HRV after the cognitive activity. The higher MeanRR and lower MeanHR indicate a quicker and more effective post-task recovery from stress. The capacity to bounce back swiftly from stressful situations is a crucial sign of healthy autonomic functioning.
The prolonged parasympathetic dominance post-task is highlighted by the further decline in the LF/HF ratio, as well as the fall in LFnu and increase in HFnu. According to these results, practicing meditation regularly with MSRT improves the body’s capacity to preserve autonomic balance and recover from stress more quickly, which benefits both mental and cardiovascular health in general.45, 46 There were notable variations in the post-task condition between the MSRT group and the control group (SR). In particular, the MSRT group had greater HFnu, lower LFnu, lower MeanHR and higher MeanRR. When compared to the control group, these between-group differences amply illustrate the better benefits of MSRT meditation in enhancing parasympathetic activity and lowering stress responses. Brew et al (2011) demonstrated that meditation activates the ACC and insula, both involved in enhancing autonomic control, which may explain the observed reductions in heart rate and increases in HRV. MSRT, through sound resonance, likely stimulates similar neural pathways, promoting a shift toward parasympathetic dominance. The MSRT group showed a marked reduction in PSS scores and a significant increase in FMI scores. This suggests that participants felt less stressed and more mindful after the intervention. These changes were absent in the SR group, highlighting the unique efficacy of MSRT. The reduction in perceived stress is further supported by studies such as Carmody and Baer (2008), which demonstrated that mindfulness meditation leads to reduced stress perception. 47 The increase in mindfulness also aligns with findings from Brown and Ryan (2003), who proposed that mindfulness enhances attention and awareness, thereby reducing psychological distress. 48 Meditation practice could enhance connectivity in neural circuits that regulate stress responses, supporting the findings of reduced stress markers in the MSRT group49, 50 also found that mindfulness-based practices increase grey matter density in brain regions related to emotional control and autonomic functions, which might explain the improved physiological responses seen in MSRT participants.
Correlational analysis reveals interesting relationships between executive function, cardiac activity and behavioural outcomes. The negative correlation between RMSSD and reaction time (incongruent task) suggests that individuals with better parasympathetic regulation tend to perform faster on cognitively demanding tasks. Similarly, the negative correlation of RMSSD with perceived stress implies that individuals with higher HRV experience lower stress levels, which is consistent with the role of HRV as a biomarker of stress resilience. 51 Additionally, the positive correlation between reaction time (incongruent) and perceived stress suggests that higher stress levels may slow down cognitive processing, particularly in tasks requiring executive control. The negative relationship between mindfulness and perceived stress further supports the notion that mindfulness practices can reduce stress. 52 MSRT practice promotes mindfulness, reducing cognitive interference and improving focus by suppressing the brain’s default mode network which reduces mind-wandering and stress. Mindfulness enhances present-moment attention and emotional regulation, which in turn decreases perceived stress and improves performance in tasks requiring cognitive control. 53 The noteworthy variations seen across groups bolster the distinct influence of MSRT on enhancing HRV, demonstrating that meditation has a quantifiable and direct impact on autonomic function.
This research suggests that MSRT could be a valuable tool for enhancing the well-being and academic performance of college students. The study demonstrates that MSRT may improve cognitive function, cardiac health and psychological well-being. Specifically, the study found that MSRT practice led to faster reaction times during cognitive tasks and positive changes in HRV, indicating improved cardiac health and stress resilience. Moreover, MSRT resulted in reduced perceived stress and increased mindfulness, suggesting potential benefits for mental well-being. To enhance the practical relevance of these findings, educational institutions could integrate short MSRT sessions into curricula or student wellness programmes, promoting attention, cognitive flexibility and stress management. Similarly, college counselling services could utilise MSRT as a stress-reduction tool for students, capitalising on its observed benefits for perceived stress and mindfulness.
The MSRT may influence neural pathways and brain function through several interconnected mechanisms. The auditory stimulation from sound resonance synchronises neural oscillations and activates the auditory cortex, promoting relaxation. Rhythmic auditory stimuli from sound resonance may stabilise heart rhythms. Engaging with sound at one’s resonance frequency stimulates respiratory sinus arrhythmia (RSA), which increases vagal tone and promotes relaxation. 54 This practice may engage the prefrontal cortex improving attentional focus and reducing amygdala activity, lowering stress responses. This auditory stimulation results in more balanced autonomic regulation, benefiting cognitive function and emotional stability.
Limitations and Future Suggestions
The current study on MSRT has several limitations. The small sample size limits the generalizability of its findings, necessitating larger, more diverse samples to confirm the observed effects on cognitive performance, HRV and psychological outcomes. The study’s short-term follow-up also leaves the long-term sustainability of these improvements unclear. Additionally, the lack of an active control group (e.g., other meditation techniques) makes it difficult to isolate the specific benefits of MSRT. Reliance on self-reported data for psychological variables introduces potential biases, and the absence of objective measures like neuroimaging or hormonal analysis weakens the physiological evidence. Furthermore, the study focused on a specific population, limiting generalizability to different demographics or health conditions. Lastly, the study did not explore the detailed neural or autonomic mechanisms behind MSRT’s effects, suggesting future research should incorporate tools like fMRI, EEG or autonomic testing for a deeper understanding of its impact. Future research could also investigate the potential benefits of combining mindfulness practices with other stress-reduction techniques, such as exercise or cognitive-behavioural therapy, to maximise the positive effects on overall well-being. Overall, continued research in this field has the potential to offer valuable tools for individuals seeking to manage and reduce their stress levels in a healthy and sustainable way.
Conclusion
The present study demonstrated that MSRT significantly improved executive functions, such as accuracy and reaction time, cardiac health and enhanced psychological well-being among college students. These findings align with evidence that meditation induces structural and functional brain changes, particularly in the prefrontal cortex, and promotes stress reduction. Additionally, MSRT was associated with increased parasympathetic activity, improved mood and lower stress and anxiety levels. These findings support incorporating MSRT into educational and wellness programmes to boost academic performance, mental well-being and long-term cardiovascular health. Further research with larger samples is warranted.
Abbreviations
MoCA: Montreal Cognitive Assessment, GHQ: General Health Questionnaire, RCT: random control trail, MSRT: mind sound resonance techniques, SR: supine rest, ECG: electroencephalography, FFT: Fast Fourier Transformation, SNS: sympathetic nervous system PNS: parasympathetic nervous system, HRV: heart rate variability, MeanRR: the mean of the intervals between the instantaneous heart rate, MeanHR: number of heart beats per minute, SDNN: square root of the squared difference of successive NN intervals, RMSSD: root mean square of successive differences between normal heartbeats, LFnu: low frequency, HFnu: high frequency, LF/HF: ratio between SNS and PNS activity, SCWT: Stroop-colour word test, RA: response accuracy, RT: response time, PSS: perceived stress scale, FMI: Freiburg mindfulness inventory, CI: confidential interval.
Footnotes
Acknowledgements
The authors are thankful to S-VYASA for granting permission to conduct the study on the institution’s premises and for the use of the cognitive laboratory. We thank all the participants for their involvement in this study. We are also grateful to the staff and others who directly or indirectly supported the completion of this study.
Author Contributions
Sushanta Kumar Mohanty: Conceptualization, formal analysis, methodology, data collection and curation, writing- original draft. Amit Singh: Methodology, validation, visualization, writing – review & editing. Krishna Dwivedi: Data curation, and formal analysis. Subrana Surajita Mohanty: Methodology, data collection and data extraction. Nagarathna Raghuram: Conceptualization, supervision, resources, and final editing. HR Nagendra: Conceptualization, supervision, resources, and final editing. Deepeshwar Singh: Conceptualization, supervision, methodology, resources, writing – review & editing.
Clinical Trial Registry
The trial was registered with the Clinical Trial Registry of India (CTRI/2021/09/036596).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Ethics Committee (RES/IEC-S-VYASA/213/2021).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
The signed informed consent form was obtained from each participant after explaining the assessment procedures in the study.