
Abstract
Background
Numerous investigations indicate the presence of a reciprocal association between type 2 diabetes (T2D) and a range of mental health conditions. However, research on the factors that contribute to depression and anxiety in T2D patients in India is scarce.
Purpose
The present study aims to identify the prevalence and predictors of depression and anxiety in patients with T2D in India.
Methods
A cross-sectional study that included 2,730 patients with T2D was conducted at the Freedom from Diabetes Clinic in Pune, India. Anxiety and depression were measured by the Patient Health Questionnaire-9 (PHQ-9) and Generalized Anxiety Disorders-7 (GAD-7) Scale. Binary logistic regression was applied to identify the factors predicting anxiety and depression.
Results
The prevalence of depression and anxiety were 20.3% and 17.3%, respectively. The major predictors of anxiety and depression were female gender, obesity, unmarried marital status, poor glycaemic control and the presence of comorbid conditions.
Conclusion
This study’s findings highlight a significant prevalence of depression and anxiety among patients with T2D in India, with key predictors including gender, obesity, marital status, glycaemic control and comorbid conditions. These findings highlight the critical need for integrated mental health support in routine diabetes care to manage depression and anxiety.
Introduction
Mental health is an important aspect in the management of all diseases, including type 2 diabetes (T2D). 1 The American Diabetes Association (ADA) recommends that a comprehensive medical evaluation of patients with diabetes should include an assessment of psychosocial/emotional health concerns, if indicated. In conjunction, the International Diabetes Federation (IDF) recommends that mental health assessment should be included as part of diabetes management. 2
T2D is a worldwide health problem that is linked to various comorbidities, such as cardiovascular disease, retinopathy, neuropathy, nephropathy, non-alcoholic fatty liver disease, polycystic ovarian syndrome and potentially some types of cancer. 3 Apart from physical complications, T2D also affects mental health, making the patients more vulnerable to diabetes fatalism. 1 . According to research, depression and anxiety are the two most common mental health issues affecting individuals with T2D globally. 4
A documented bi-directional relationship exists between T2D and depression, wherein not only diabetes can lead to depression but also vice versa.5, 6 The prevalence of depressive disorders in individuals with diabetes is twice as high as in those without diabetes. 7 Likewise, anxiety disorders also have a negative correlation with T2D and are a leading cause of disability worldwide. 8 Based on data from a systematic review, globally, the prevalence of depression and anxiety disorders linked with hyperglycaemia accounts for 28% and 14% of patients with T2D, respectively. 9
Diabetes management relies on self-care and adhering to the prescribed treatment to avoid complications. The presence of psychological distress, mainly depression and anxiety, hinders the self-care routine and compliance with the treatment protocol. 10 This in turn may worsen the prognosis of diabetes. 7 According to recent studies, patients with diabetes who also have anxiety and depression often face increased medical expenses, disruptions to daily routines and lower quality of life, 11 as well as an increased risk of microvascular (retinopathy, nephropathy and neuropathy) and macrovascular (cerebrovascular disease, ischemic heart disease) complications.12, 13 This in turn increases the chances of mortality due to diabetes-related comorbidities in T2D patients. 3
Asian Indians are prone to developing T2D due to their ethnic differences characterised by high levels of abdominal fat. There is currently a paucity of information available on the prevalence and contributing factors of depression and anxiety in Indian individuals with T2D. Few studies have shown the burden of depression and anxiety in the Indian population, but they are limited to certain geographical regions, making it difficult to estimate the actual burden of the disease. Considering the magnitude of the psychological disorder in T2D patients and the lack of current research, the present study aimed to assess the prevalence and associated risk factors of depression and anxiety in Indian patients with T2D enrolled in a lifestyle management programme.
Methods
Study Design
This cross-sectional study was carried out from May 2021 to September 2022 on patients with T2D attending an online one-year diabetes management programme at the Freedom from Diabetes in Pune, India. The study involved patients from 334 cities across India.
Study Population and Sampling
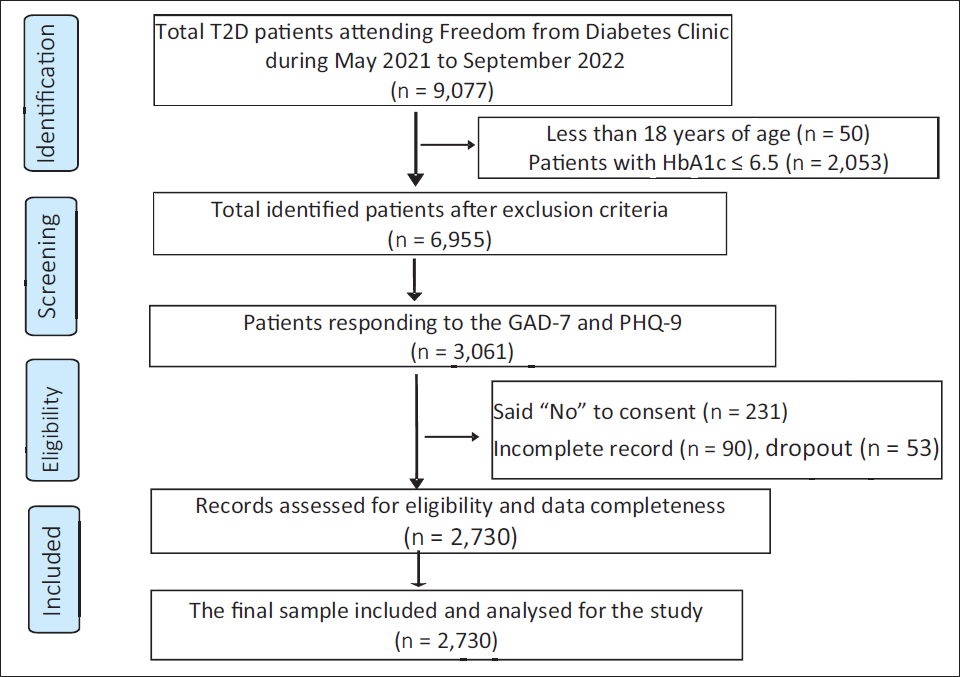
All patients attending a diabetes management clinic during the study period were screened for eligibility to participate. The inclusion criteria were adults (above 18 years of age) and a confirmed diagnosis of T2D (all patients on treatment with oral hypoglycaemic agents and/or insulin or HbA1c ≥ 48 mmol/mol (6.5%) without medication). Patients who reported a prior history of psychiatric illness that had been medically diagnosed and verified with medical records and pregnant and lactating women were excluded. Patients who met the study criteria were subsequently approached for written consent. Before obtaining consent, all potential participants were informed about the study’s purpose and the procedures that would be involved. Following this, all consenting patients were enrolled in the study. The enrolment procedure for patients in the study is illustrated in Figure 1.
Flowchart Depicting the Selection Procedure of Patients for the Study.
Tests and Scales
The data for the study was collected electronically through Google Forms using a self-administered questionnaire. The questionnaire was separated into two sections: Section I included the assessment of sociodemographic data (gender, age, marital status, education status, occupation, family history and employment status), anthropometric data (height, weight), medical history (date of detection, associated comorbidities, medication status) and clinical parameters (HbA1c); Section II assessed depression and anxiety through the Patient Health Questionnaire-9 (PHQ-9) and Generalized Anxiety Disorder (GAD-7) scales.
Anthropometric data were collected through self-reporting by the participants. Detailed instructions on measuring height and weight (in triplicates) were given to ensure accuracy. Depression was assessed using the PHQ-9 (2001), a nine-item self-report screening tool. Each item is assessed on a 4-point scale ranging from 0 to 3, with 0 representing ‘never’, 1 indicating ‘several days’, 2 signifying ‘more than half the time’ and 3 standing for ‘nearly every day’. The overall scores ranged from 0 to 27, with higher values indicating greater severity. Mild, moderate, moderately severe and severe depression are indicated by scores of 5, 10, 15 and 20, respectively, with cut-offs set accordingly. The PHQ-9 exhibits a sensitivity of 88% and a specificity of 88% in identifying depression. 14
Anxiety symptoms were assessed using the GAD-7 (2006), a seven-item self-report screening tool. Each item is assessed on a 4-point scale ranging from 0 to 3 (0 representing ‘never’, 1 indicating ‘several days’, 2 signifying ‘more than half the time’ and 3 standing for ‘nearly every day’). The overall scores ranged from 0 to 21, with higher scores indicating greater symptom severity. Cut-offs for mild, moderate and severe anxiety were indicated by scores of 5, 10 and 15, respectively. GAD-7 exhibits a sensitivity of 89% and a specificity of 82% in identifying anxiety. It has demonstrated moderate effectiveness in identifying three additional prevalent anxiety disorders: panic disorder, social anxiety disorder and post-traumatic stress disorder. 15
Statistical Analyses
All the data were checked for completeness and accuracy. The data were extracted first to Microsoft Excel and then to SPSS (Statistical Package for the Social Sciences, ver. 21.0 IBM, Armonk, New York, USA) for analysis. A descriptive analysis was done, and continuous variables are shown as the mean and standard deviation, while categorical variables are presented as frequency and percentages. During analysis, the patients were classified as either with or without depression and anxiety using a cut-off of 10.14, 15 Bivariate correlations were used to assess significant associations of sociodemographic, anthropometric and biochemical variables with depression and anxiety. Significant parameters from correlation analysis were included in a binary logistic regression model to identify the independent predictors of depression and anxiety. Findings are reported as adjusted odds ratios and 95% confidence intervals. All tests were two-tailed at a significance of p < .05.
Results
Sociodemographic, Clinical and Other Characteristics of the Study Population
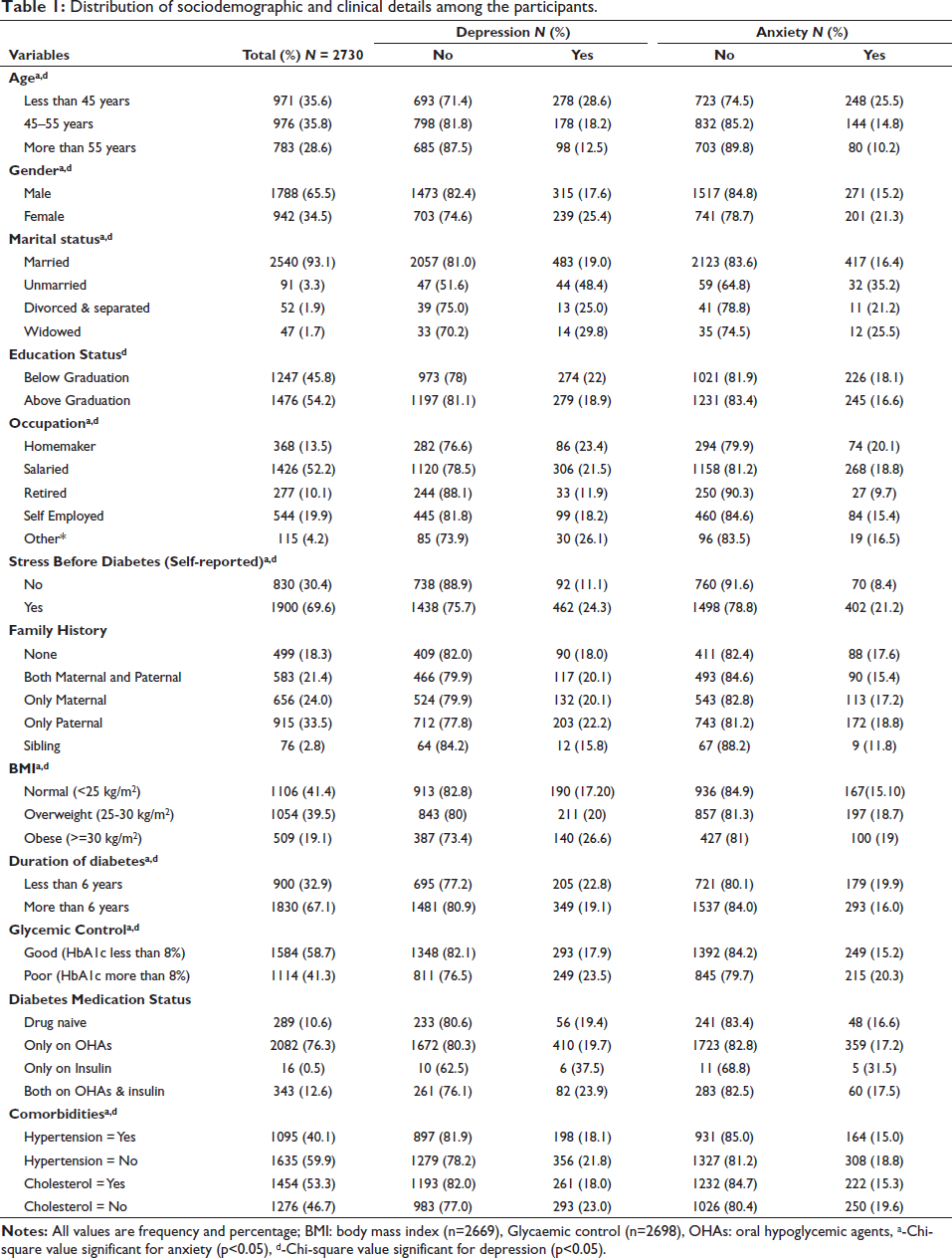
The mean age and duration of diabetes in patients were 49.7 ± 10.2 and 10 ± 7 years, respectively. The patients were mostly men (65.4%), married (93%), salaried (52.2%), had diabetes for more than six years (67%) and had a self-reported history of stress before diabetes (69.6%). Most of the patients had a family history of diabetes (81.7%). The mean baseline weight (kg), BMI (kg/m2) and HbA1c (%) levels of the patient were 74.2 ± 14.3, 26.5 ± 4 and 8 ± 1.7, respectively. The majority (88.8%) of patients were on diabetic medication, and most of them reported having one or more comorbidities (Table 1).
Distribution of sociodemographic and clinical details among the participants.
Prevalence of Depression and Anxiety
The prevalence of depression and anxiety was 20.3% and 17.3%, respectively. Patients with depression were categorised based on the severity as mild (27.3%), moderate (13.5%), moderately severe (4.5%) and severe (2.1%). Patients with anxiety were also categorised based on the severity as mild (29.6%), moderate (10.3%) and severe (6.9%).
Association of Depression and Anxiety with Sociodemographic, Anthropometric and Diabetes-related Parameters
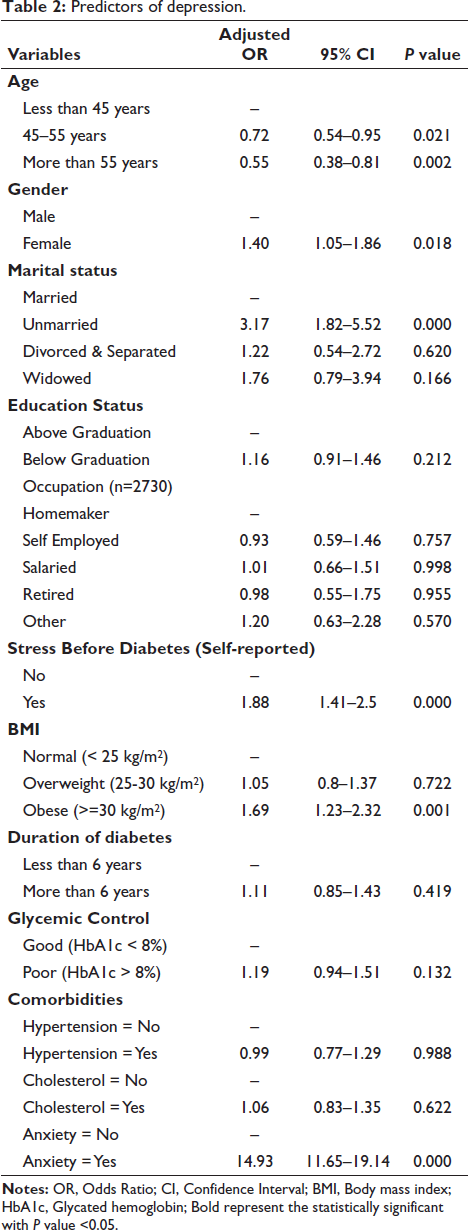
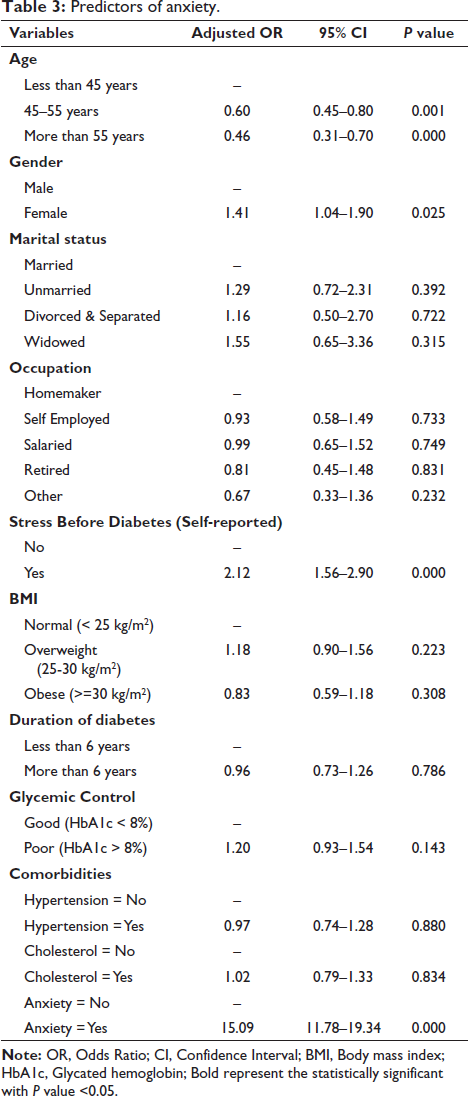
Regression analysis revealed that female gender, unmarried status, self-reported stress before diagnosis, obesity (BMI > 30 kg/m2) and the presence of comorbid anxiety were significant predictors of depression (Table 2). Similarly, for anxiety, only female gender, self-reported stress before diagnosis and the presence of comorbid depression were significant predictors observed (Table 3).
Predictors of depression
Predictors of anxiety.
Discussion
Depression and anxiety impact diabetes severity, complications and quality of life, making them crucial components to address in T2D management. 11 The current study reflects on the prevalence of and the relationship between depression, anxiety and T2D in the Indian population. In our cross-sectional study on Indian patients with T2D, we found the prevalence of depression and anxiety was 20.3% and 17.3%, respectively. It was lower than that reported by other Indian studies.16, 17 Further, our study showed that depression was more common than anxiety in the population, which aligns with previous research.18, 19
Female gender, being unmarried, those with self-reported stress before diagnosis, obesity, poor glycaemic control and the presence of co-existing anxiety were significant predictors of depression in the study population. However, female gender, self-reported stress before diagnosis and co-existing depression were the only significant predictors of anxiety. Our findings indicate that individuals below the age of 50, specifically those between 18 and 50, are more susceptible to experiencing depression and anxiety compared to those over the age of 50, which is in line with results reported by Alzahrani et al. in 2019. 20 However, this contradicts the report by Karpha et al., 16 that the risk of depression was higher in T2D patients who were older. We also found that women are at a higher risk of developing depression (AOR 1.4, p = .019) and anxiety (AOR 1.41, p < .05) compared to men. This is consistent with other studies.21, 22 The prevalence may be higher due to gender-specific issues such as maternity, menstrual cycles and hormonal disorders that may induce stress. 23 However, this contradicts the results of Karpha et al. and Balhara et al.,16, 24 which showed similar prevalence in men and women. The likelihood of experiencing depression was triple in the unmarried patients who participated in the study, which is similar to reports from previous studies16, 25 but is in contrast with the findings of Rajput et al., 26 who showed increased odds of depression in married cases. Our analysis did not reveal a statistically significant association between anxiety and marital status, which is contradictory to previous findings reporting the increased odds of anxiety in married and widowed individuals.16, 27
In our study, patients who reported stress before diagnosis of diabetes were found to have a significantly increased risk of depression (2.12 times) and anxiety (2.12 times). This suggests that stress and the way patients respond to it may trigger the development of these mental health conditions. 28 Several studies have reported a high occurrence of depression and anxiety in individuals with a higher BMI.16, 17, 29 Similar results were observed in our study, where a significantly higher risk of depression (1.69 times) was observed in patients with a greater BMI. However, we did not see a statistically significant association between BMI and anxiety, which is consistent with previous research. 29 In our study, longer diabetes duration (>6 years) did not show any association with the incidence of depression and anxiety, which aligns with the findings of Siddiqui et al. and Raval et al.30, 31 but contradicts other research that reported a link between longer duration and anxiety and depression.32–34
Depression and anxiety have been linked to poor management and adherence to treatment in patients with T2D and have been identified as predictors of poor glycaemic control. Our study found a non-significant yet 1.2-fold rise in the likelihood of depression and anxiety among patients with poor glycaemic control (HbA1c > 8%). These results are consistent with previously reported studies on the association between depression and anxiety.20, 35, 36 Several studies have reported the association of depression and anxiety with the presence of comorbid conditions.26, 37 Our study did not show an association between the presence of dyslipidemia and hypertension as comorbid conditions and depression and anxiety. However, the presence of comorbid depression (AOR = 14.93) was a stronger predictor of anxiety, while comorbid anxiety (AOR = 15.09) was a strong predictor of depression in our study patients. These findings align with previous research by Trento et al. and Sun et al. 38, 39 In the current study, occupation and education status did not show any significant association with depression and anxiety. Family history of diabetes and medication status did not appear to be associated with depression or anxiety, which contrasts with other studies that showed an association of these factors with depression and anxiety in patients with T2D.18, 19, 40 This may be because 80% of the population in the present study reported a family history of diabetes.
The primary strength of this study lies in its substantial sample size, encompassing a broader geographical area in contrast to previous studies conducted on the Indian population. However, there were a few limitations. This single-centre study design might introduce the potential for selection bias. However, the enrolment of patients from 334 cities across India mitigates this concern to a considerable extent. Another limitation pertains to the socio-economic status of the patients. The online diabetes management programme operates on a subscription-based model, potentially restricting access to those who can afford it. Consequently, the generalisability of our findings to the broader Indian context may be limited. Further, the present study is limited in its exploration of other factors within the psychological and physiological domains, as it did not assess variables such as stressful life events that could potentially impact mental health status. Nonetheless, despite these limitations, the study provides valuable insights into the prevalence and predictors of anxiety and depression within the Indian population with diabetes.
Conclusion
To summarise, this research indicates a prevalence of 20.3% for depression and 17.3% for anxiety. Recognising the substantial impact of compromised mental well-being on individuals with T2D, it is imperative to incorporate regular psychological interventions within primary care settings. This approach is vital for addressing and reducing symptoms of depression and anxiety among this particular patient population, taking into account their unique social, clinical and demographic characteristics.
Authors’ Contribution
Conceptualisation, methodology/design, investigations—PT and NK; data collection and management—BS, MDB, DT, AV and TK; original draft—BS and NK; data analysis and interpretation—BS and NK; reviewing and editing—NK, VV and MK; revising the manuscript critically for important intellectual content—NK and MK.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Ethics
Ethical clearance for the study was granted by the ethics committee of Dr D. Y. Patil Vidyapeeth, Pune, India. All methods were carried out in accordance with relevant guidelines and regulations.