
Abstract
Background
Hyperdense middle cerebral artery sign (HMCAS) on a non-enhanced multidetector computed tomography (MDCT) scan is considered an important radiological marker in detecting acute arterial thrombotic occlusion, and it is one of the earliest signs of ischemic cerebrovascular accident (CVA). This finding has been observed within 90 min of symptom onset. Modern approaches to patients with cerebral infarction emphasize early diagnosis and management.
Purpose
To determine the diagnostic accuracy of hyperdense artery signs in early detection of middle cerebral artery (MCA) infarction on non-contrast-enhanced MDCT scan using Magnetic Resonance Angiography (MRA) within 24 h as the gold standard for definitive diagnosis.
Method
A total of 140 patients aged 35–70 years, referred to the radiology department of Aga Khan University Hospital with clinical suspicion of acute cerebral infarction, were included. After clinical suspicion of acute infarction, the patient underwent an initial complete MDCT scan of the brain, which was performed using Aquilion ONE 640 slice MDCT (Toshiba Medical Systems, Japan). Consultant radiologists, with a minimum of 5 years of experience in MDCT brain imaging, interpreted the images. Follow-up examination with MRA within 24 h was performed to confirm the diagnosis of MCA infarction.
Results
Overall sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy of HMCAS in the early detection of MCA infarction on non-contrast-enhanced MDCT scan using MRA as the gold standard for definitive diagnosis was 96.20%, 93.44%, 95.0%, 95.0%, and 95.0%, respectively.
Conclusion
This study concluded that the diagnostic accuracy of hyperdense artery signs in the early detection of MCA infarction on non-contrast-enhanced MDCT scans is very high.
Keywords
Introduction
Magnetic resonance imaging (MRI) and multidetector computed tomography (MDCT) are significant diagnostic tests in the management of acute stroke. 1 The ideal method in the initial stroke diagnosis is a MDCT scan due to its ease of operation, readable availability, and short examination time. 2 MDCT can visualize acute thromboembolism in the intracranial arteries. On a non contrast MDCT scan, an artery visualized as diffuse high density and higher density compared to other visualized vessels should raise suspicion for acute occlusion by a clot in an acute stroke setting. 3
Following the initial hours of acute stroke, even when a large territory is involved, MDCT findings may be unremarkable. However, there are various markers of early acute stroke on MDCT: (1) hypodensity in basal ganglia, (2) hypoattenuation of the insular ribbon, (3) convexity sulci effacement, and (4) the hyperdense middle cerebral artery sign (HMCAS). 4 In acute stroke, visualization of these minor signs of ischemia and infarction on MDCT is significant as these signs have diagnostic and prognostic importance. 5
The hyperdense middle cerebral artery sign (HMCAS) is the presence of high attenuation of the proximal segment of the middle cerebral artery (MCA) that is frequently accompanied by the M1 segment thrombosis of MCA. After a stroke of ischemic nature, it might be an initial diagnostic sign on MDCT. 6 M2-segment is known as the appearance of the hyperdense area within the Sylvian fissure of branches of MCA. It is recognized as a dot sign, which designates an occlusion due to an embolus in distal MCA overall; in comparison to M1-segment hyperdensity, this has a much better prognosis. 7
The HMCAS in a non-enhanced MDCT scan is considered an early sign of an ischemic cerebrovascular accident (CVA). It is usually observed within 90 min of symptom appearance. 8 It is also considered as a significant radiological marker in indicating acute arterial thrombotic occlusion. 9 Latest approaches to patients with cerebral infarction accentuate early diagnosis and management. 10 The HMCAS on MDCT indicates the development of a large cerebral infarction. Emergency MDCT of the brain is the standard first-step diagnostic method in patients with acute, focal neurologic deficits. 10 HMCAS is a subjective outcome, but previous research has indicated objective features of HMCAS. 11
A study reported that HMCAS is present in 5% of their patients; however, a much higher incidence has been reported by other studies.12, 13 MR angiography, on the other hand, is effective for detecting intravascular occlusion caused by a thrombus and accessing carotid bifurcation in acute stroke patients.14–16 This modality is considered the gold standard because of its safety (compared to formal cerebral angiography), with avoidance of radiation and contrast bolus as with computed tomography angiography (CTA), with an equally good evaluation of acute stroke and depiction of the penumbra.14, 17 Moreover, the MRI findings are simple to interpret when compared to CTA. 14 Nevertheless, the CT scan hardly takes 5 min in comparison to the MRI examination, which takes at least 15 min to complete. Fifteen studies have previously stated that HMCAS’s specificity in detecting MCA occlusion is close to 93.4% with a relatively lower sensitivity of 78.5%. 10
Recent studies11, 18–20 observed the importance of thin slice NECCT reconstructed on MDCT. Approximately 80% rise in sensitivity was reported in these studies. Due to a local increase of hematocrit during the clotting process, the clotted blood has a hyperdense appearance. 21 False positive results have been noticed in individuals with atherosclerosis and increased hematocrit. Therefore, correctly identifying this sign is essential in detecting and managing acute infarction early.
In this study, our objective was to assess the diagnostic accuracy of the hyperdense artery sign in the early detection of MCA infarction on non-contrast enhanced MDCT scan. We utilized Magnetic Resonance Angiography (MRA) performed within 24 h as the gold standard for definitive diagnosis. The rationale behind our research stems from the potential benefits of MDCT in facilitating the early detection of acute infarction. In comparison to MRI, MDCT offers significant advantages in time due to its faster imaging acquisition. This speed can be critical in time-sensitive scenarios, enabling prompt evaluation and timely decision-making for patients suspected of having an acute infarction.
Objectives
The objective of the study was:
“To determine the diagnostic accuracy of hyperdense artery sign in early detection of MCA infarction on non-contrast enhanced MDCT scan using MRA within 24 h as Gold standard for definitive diagnosis.”
Operational Definitions
Methods
Study Design
A cross-sectional validation study.
Setting
Department of Radiology, Aga Khan University Hospital Karachi.
Duration of Study
21st January 2020 to 20th January 2021.
Sample Size
Sensitivity: 78.5% 10
Specificity: 93.4% 10
The margin of error for sensitivity is 13%, and for specificity, 7%
Prevalence of HMCAS in Stoke: 12–28% 10
Confidence level: 95%
The sample size required: 140.
Sample Technique
Non-probability, consecutive sampling.
Sample Selection
All patients aged 35–70 years are referred to the radiology department of Aga Khan University Hospital with clinical suspicion of acute cerebral infarction, as stated above in the operational definition.
Already diagnosed cases of acute cerebral infarction turned up for follow-up examination. No evident hyperdense artery sign on the initial MDCT.
Data Collection Procedure
The study was started after the approval of the synopsis from the Ethical Review Committee of Aga Khan Hospital on 9th September 2019 (2019-2420-502n). Informed consent was also taken from all patients before enrolling in the study. The patients had undergone an initial Complete MDCT scan of the brain, which was performed using Aquilion ONE 640 slice MDCT (Toshiba Medical Systems, Japan) after clinical suspicion of acute infarction. Images were interpreted by consultant radiologists with minimum 5 years of experience in MDCT brain imaging. Follow-up examination with MRA within 24 h was performed to confirm the diagnosis of MCA infarction.
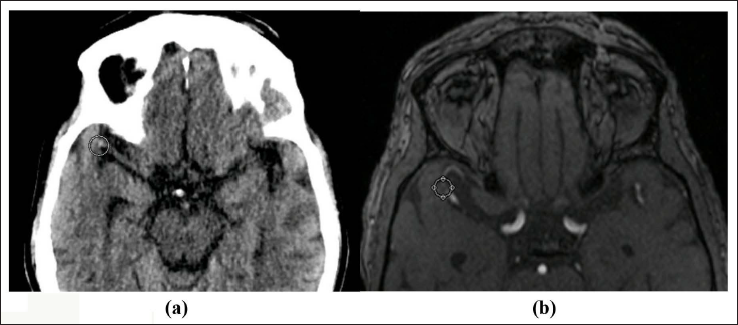
(a) MDCT Axial Images of a 58-Year-old Woman Showing Dense Right MCA Bifurcation. (b) Corresponding TOF MRA Shows No Signal in the Corresponding Artery.
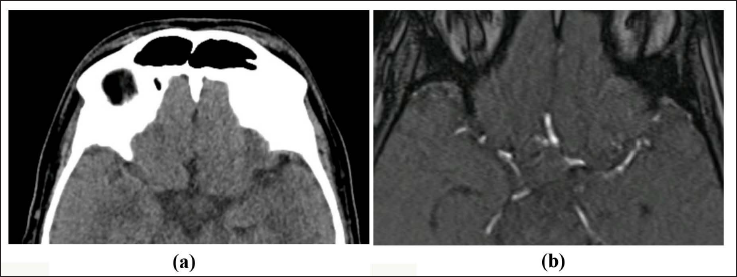
(a) MDCT Axial Images of a 58-Years-old Woman Showing Dense Right MCA Bifurcation. (b) Corresponding TOF MRA Shows No Signal in the Corresponding Artery.
Data Analysis Procedure
Collected data was analyzed through computer software SPSS 22.0. Age was presented as mean and standard deviation. Gender and findings on MDCT and MRA were presented as frequency and percentage. A contingency table (2×2) was used to calculate sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy of hyperdense artery sign in early detection of MCA infarction on the non-contrast-enhanced MDCT scan using MRA as the gold standard for definitive diagnosis. Stratification was done for age and gender. Post-stratification diagnostic accuracy was calculated.
Results
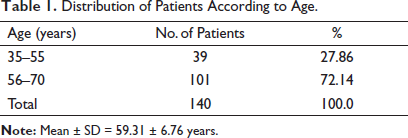
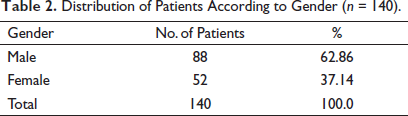
We stratified diagnostic accuracy according to age groups and gender. The age range in this study was from 35 to 70 years, with a mean age of 59.31 ± 6.76 years. The majority of the patients, 101 (72.14%), were between 56 and 70 years of age, as shown in Table 1. Out of these 140 patients, 88 (62.86%) were males, and 52 (37.14%) were females, with a ratio of 1.7:1 (Table 2).
Distribution of Patients According to Age.
Distribution of Patients According to Gender (n = 140).
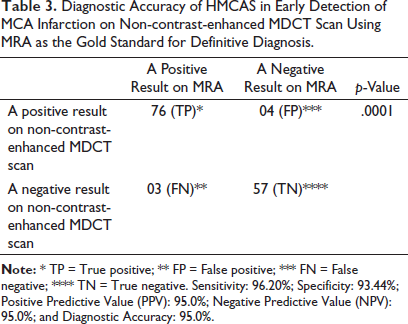
All the patients were subjected to MDCT, and it was found that 76 were True Positive and 04 were False Positive. Among 60 MDCT-negative patients, 03 (False Negative) had a stroke on MRA, whereas 57 (True Negative) had no stroke on MRA (p = .0001), as shown in Table 3. Overall sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy of hyperdense artery sign in early detection of MCA infarction on non-contrast-enhanced MDCT scan using MRA as the gold standard for definitive diagnosis was 96.20%, 93.44%, 95.0%, 95.0%, and 95.0%, respectively.
Diagnostic Accuracy of HMCAS in Early Detection of MCA Infarction on Non-contrast-enhanced MDCT Scan Using MRA as the Gold Standard for Definitive Diagnosis.
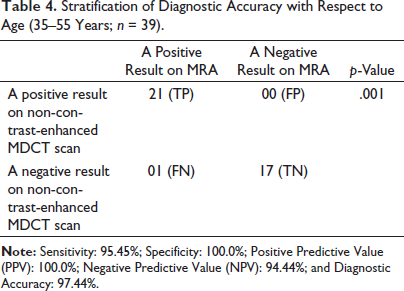
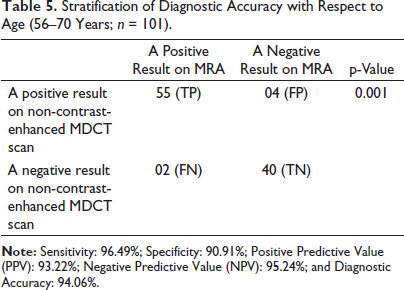
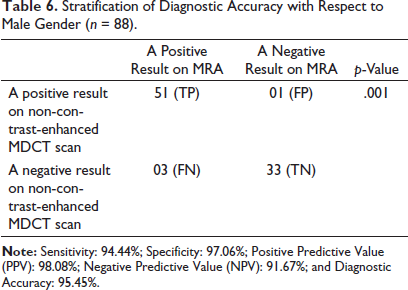
Stratification of diagnostic accuracy with respect to age groups is shown in Tables 4 and 5. Gender stratification is shown in Tables 6 and 7.
Stratification of Diagnostic Accuracy with Respect to Age (35–55 Years; n = 39).
Stratification of Diagnostic Accuracy with Respect to Age (56–70 Years; n = 101).
Stratification of Diagnostic Accuracy with Respect to Male Gender (n = 88).
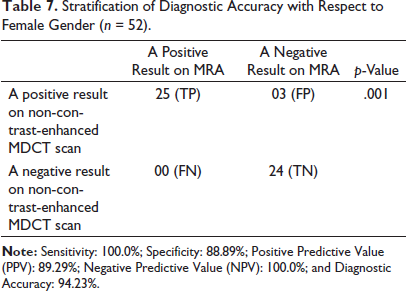
Stratification of Diagnostic Accuracy with Respect to Female Gender (n = 52).
Discussion
MDCT without contrast is the primary imaging method for the initial investigation of stroke in various settings. 24 Therefore, MDCT remains significant for routine evaluation of ischemic stroke. Hyper-attenuation in the cerebral artery on non-contrast MDCT may indicate an embolus or acute thrombus in acute ischemic stroke; therefore, HMCAS indicates arterial obstruction and may deliver valuable information for acute ischemic stroke diagnosis. HMCAS is described as an artery that subjectively looks temporarily denser when compared to neighboring or equivalent contralateral vessels3, 25 even after administering impartial measures. 26 In comparison to HMCAS with angiography, it has been revealed that HMCAS is a specific (however, false positives are described) 27 but less sensitive marker of arterial obstruction.28, 29 There is no published meta-analysis regarding HMCAS sensitivity and specificity according to the recent literature.
A randomized multicenter trial, Third International Stroke Trial (IST-3), assessed intravenous thrombolysis (Alteplase) administered less than 6 h after the onset of ischemic stroke. All 3035 participants of this trial had baseline (pre-randomization) and follow-up (within 48 h) brain imaging (predominantly non-contrast MDCT) performed. Pre-randomization MR angiography (MRA) or MDCT angiography (CTA) were routinely performed for stroke imaging protocol.30, 31
This study was conducted to estimate the diagnostic precision of HMCAS in early diagnosis of infarction in MCA on enhanced MDCT scan without contrast using Magnetic MRA as the gold standard for definitive diagnosis. Negative and positive predictive value, overall sensitivity, specificity, and diagnostic accuracy of HMCAS in early detection of infarction in MCA on enhanced MDCT scan without contrast using MRA as the gold standard for definitive diagnosis was 95.0%, 95.0%, 96.20%, 93.44%, and 95.0%, respectively. Previously, studies have shown the specificity of HMCAS in identifying occlusion in MCA as close to 93.4% with a relatively lower sensitivity of 78.5%. 10
American Heart Association recommends NCCT as the initial investigation in stroke 32 due to its swiftness, convenience, and patient tolerance, and therefore, quickly allowing the rapid administration of stroke patients. Various types of research demonstrated a relationship between the size of baseline and the final infarct volume, clinical event, and risk of hemorrhage formation during intravenous thrombolysis with tissue plasminogen activator and intra-arterial stroke interventions.33, 34 Furthermore, research indicates that hypoattenuation shown on MDCT is precisely specific in irreversible ischemic damage of the brain if it is diagnosed in the initial 6 h. Brain tissue of patients with an absence of hypoattenuation suggests a favorable outcome. 35 The lack of infarction in imaging should not delay stroke treatment in the suspected patients. However, visualization of infarct on imaging signifies the diagnosis. It allows a more subtle management plan for thrombolysis and endovascular intervention made by the magnitude and severity of infarction on appearance.35, 36
In 30% of patients undergoing a vascular event in the MCA territory, the HMCAS is usually observed.28, 37 In various types of research, this sign is reported qualitatively with HU values not being specified. However, a value greater than 43 HU in attenuation of the affected MCA was found to be positive by Koo et al. 26 On the other hand, Schuknecht et al., conducting the same research, found no relation between both MCAs. 38 Another study found that the value of MCA attenuation greater than 50 HU and the ratio of MCA (affected MCA/healthy MCA) greater than 1.4 as the absolute limit amongst the presence and absence of HMCAS. 13 Concerning the attenuation changes in various parts of the MCA territory, there is controversy regarding the clinical significance, reliability, and prognostic value of EICs on MDCT.39, 40 However, HMCAS is a distinct and easily identifiable radiological finding. The sensitivity of HMCAS is quite low for MCA thromboembolic occlusion even though its specificity may be almost 100%. 41 Increased hematocrit and MCA wall calcification are common sources for false positive HMCAS. 11 The incidence of HMCAS varies greatly based on the population studied and it occurred in 30% of cases with the MCA territory infarction. 11 According to a recent meta-analysis, The HMCAS is prevalent in 17%–50% of acute MCA occlusions, with 95% specificity and 52% low sensitivity. 19 A study evaluated the sensitivity and specificity of the HMCAS on thin-slice (1.5 mm) NCCT along with NIHSS score and clinical history and discovered a sensitivity of 79% in patients with LVO with an NIHSS > 10. 42 A recent study reported similar findings and it showed that combination of NIHSS score and the absolute attenuation value of the MCA on NCCT demonstrated a sensitivity of 85% for LVO. 43
Limitations
One of the primary limitations of our study was the restriction to a single center, which may introduce potential biases and limit the generalizability of our findings to a broader population. The absence of data from multiple centers reduces the diversity and may not adequately represent the variability seen in different healthcare settings.
Another notable limitation was the relatively small sample size used in our study. A smaller sample size increases the risk of random variations and reduces the statistical power to detect significant differences. Consequently, the probability of errors, such as Type I or Type II, was higher, which could impact the reliability and precision of our results.
To mitigate these limitations in future research, it is recommended to conduct multicenter studies that involve a larger and more diverse sample size. This would enhance the external validity of the findings and provide a more comprehensive understanding of the diagnostic accuracy of the hyperdense artery sign. A larger sample size would also improve the statistical power, leading to more robust and reliable conclusions.
Furthermore, it would be valuable to explore the potential impact of these limitations on the interpretation and implications of our findings. Addressing these limitations and conducting further research in a multicenter setting with an increased sample size would strengthen the validity and reliability of the study, providing a more accurate representation of the diagnostic accuracy of the hyperdense artery sign in the early detection of MCA infarction on non-contrast-enhanced MDCT scan.
Conclusion
This study concluded that the diagnostic accuracy of hyperdense artery signs in the early detection of MCA infarction on non-contrast-enhanced CT scans is very high. Therefore, we recommend that hyperdense artery sign on CT scans should be used routinely as a primary modality for accurate detection of MCA infarction, which will result in proper management of patients.
Footnotes
Authors’ Contribution
The conceptualization was done by YW and FM. The literature and drafting of the manuscript were conducted by YW, HSR, HF, and FR. The editing and supervision were performed by FM. All authors have read and agreed to the final version of the manuscript.
Statement of Ethics
Approval of the study was provided from the Ethical Review Committee of Aga Khan Hospital on 9th September 2019 (2019-2420-502n). Informed consent was also taken from all patients before enrolling in the study.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patients for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.