
Abstract
Background
Conduction velocity of the short segment of the median motor nerve, across wrist (transcarpal motor conduction velocity (TCMCV)), has been used to increase diagnostic yield in carpal tunnel syndrome (CTS). However, repeatability of this parameter has not been studied till date. It has not been used as an indicator of response to treatment. Using surface stimulation techniques, it is difficult to localize the sites of stimulation of transcarpal segment of median nerve in palm. As a result, small errors in measurements of TCMCV can be magnified and variability of TCMCV may occur on successive measurements. Despite this possible variation, TCMCV can be a useful tool for assessing response to therapy, if its repeatability is assessed and a cut-off value determined for a significant change in nerve conduction velocity.
Purpose
In this study, it was determined whether TCMCV is repeatable. If found to be repeatable, we show a method to determine the cut-off value of the change in this parameter for it to be considered significant.
Methods
Difference between values of TCMCV on successive measurements was obtained in hands of 26 controls. Repeatability of this parameter was determined in this control population following criteria of British Standards Institution. In 19 patients of CTS, treated with intracarpal steroid injection, pre-treatment and post-treatment values of TCMCV, and of symptom severity scale (SSS) and functional status scale (FSS), were obtained at 1, 2, and 3 months after treatment.
Results
Repeat measurements of TCMCV were made in each hand of all controls. After applying criteria of British Standards Institution, to such recordings, TCMCV was found to be repeatable and the cut-off value for significant change determined. According to this cut-off value, 4 patients of CTS showed improvement in TCMCV, with consistent improvement in SSS and FSS. Change in TCMCV corroborated qualitatively with changes in SSS and FSS.
Conclusion
Repeatability of TCMCV can be assessed by criteria of British Standards Institution and a cut-off value determined to use it as an indicator of response to treatment in CTS.
Keywords
Introduction
Nerve conduction velocity (NCV) is a commonly used parameter to assess problems in conduction along compressed segments of nerves. Carpal tunnel syndrome (CTS), a common compressive neuropathy of the median nerve at the wrist, is commonly diagnosed by assessing conduction velocity of the forearm motor segment of the median nerve and less often by study of the affected transcarpal motor segment. Review of literature available till date shows that transcarpal motor conduction velocity (TCMCV) has been used to increase diagnostic yield in CTS.1–6 A previous study has reported the variability of forearm ulnar nerve motor conduction velocity upon repeated trials. 7 As far as we know, till date, no interventional study on CTS has taken into account the repeatability of TCMCV. It is known that using surface stimulation techniques, it is difficult to accurately localize the sites of stimulation of transcarpal segment of median nerve. This is due to peculiar course of this segment of the nerve in the palm, and thickness of the transcarpal ligament. 8 Short distance between successive points of stimulation causes small errors in measurement of TCMCV to be magnified. In spite of this variability, TCMCV can prove to be a useful indicator of response to treatment in CTS, if its repeatability is assessed and a cut-off value determined to identify significant change in the velocity. In a cohort of subjects, if difference (∇V) of TCMCV between successive measurements in each subject is determined, mean of the differences is zero and 95% of such differences (between two successive measurements) fall within two standard deviations of ∇V, then the method of measuring TCMCV can be said to be repeatable as per criteria of British Standards Institution. 12 To assess repeatability of the short segment nerve conduction velocity (of median nerve), the distribution of ∇V should fit a Gaussian distribution, with mean of ∇V equal to zero. The standard deviation of this distribution and the 95% confidence interval of this distribution of ∇V is to be applied to study the difference of the same short segment motor conduction velocity, between final and initial recordings (say ∇Vp) in patients, being done by the same investigator using the same instrument. Then change in ∇Vp beyond two standard deviations (95% Confidence Interval) will indicate a true change in nerve conduction velocity. This study was undertaken to find out if TCMCV is repeatable and how to obtain a cut-off value of ∇V to be significant.
Method
This study commenced after approval from the Institutional Ethics Committee, IPGME&R (Institute of Post Graduate Medical Education & Research) and Seth Sukhlal Karnani Memorial (SSKM) Hospital, Kolkata, with approval letter Inst./IEC/1062. Written, informed consent was obtained from both cases and controls.
Patients
This longitudinal study included 25 patients, who attended the outpatient clinic of the Department of Rheumatology and Clinical Immunology, IPGME&R and SSKM Hospital, having symptoms of pain and paresthesia in the hand, with nocturnal and activity-induced aggravation, for at least 3 months. Phalen’s and Tinel’s signs were considered supportive diagnostic criteria. Patients with polyneuropathy, pregnancy, prior treatment of CTS, and cervical radiculopathy were excluded from the study.
There were 13 unilateral and 12 bilateral cases, of whom 19 patients completed the entire duration of study.
Controls
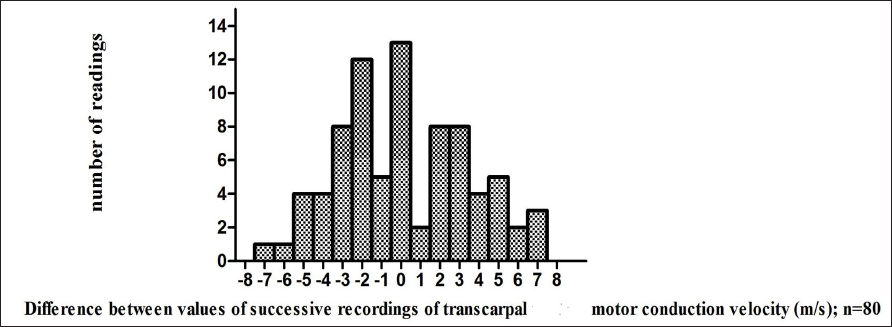
Twenty-six age-matched healthy volunteers were selected for study of the transcarpal segment of the median nerve. Both hands of each subject were studied and TCMCV was determined separately for each sitting. Two separate recordings of TCMCV were obtained in each hand in all subjects, 3 such recordings in 7 subjects, and 4 recordings in another 7 subjects. Difference between successive values of TCMCV in the same hand (∇V) was recorded and the resulting distribution of (∇V) in control subjects was plotted on a histogram . Thus, altogether 80 recordings of difference (∇V) in TCMCV were obtained from the hands of 26 controls.
Electrophysiology
Nerve conduction study (NCS) was performed in the Electrophysiology laboratory, Department of Physiology, IPGME&R using RMS NCV EMG EPII Electromyograph with RMS stimulator (Recorder and Medicare Systems Ltd., Haryana, India).
All subjects were examined in supine posture. Motor and sensory studies of median and ulnar nerves were undertaken using supramaximal surface stimulation, by the same investigator,
(Pinaki Das (P.D.)) on controls and on patients, initially and at the end of first, second, and third months after treatment. Stainless steel disc electrodes and ring electrodes were used for motor and sensory studies, respectively, with ground electrode placed over dorsum of hand. Skin temperature was kept above 32°C. Identical sites of stimulating, recording, and reference electrodes were used at each visit. The sites of stimulation and application of respective electrodes was noted and the distance between them measured with a tape. This distance was kept constant at every examination.
Motor Nerve Conduction (MNC) Study
Motor studies of median and ulnar nerves were performed by eliciting compound muscle action potentials (CMAPs) from abductor pollicis brevis (APB) and abductor digiti minimi (ADM), respectively. Recording (G1) and reference (G2) electrodes were used following the belly tendon montage. Median and ulnar nerves were stimulated 3 cm proximal to distal wrist crease (DWC), at equal distance from G1 and at the elbow, respectively. For the median nerve, this distance from the site of stimulation at wrist to G1 was equal to the sum of the distance from APB to mid-point of DWC and then from the latter to the most proximal site of stimulation at wrist (3 cm from DWC). 9 In case of the ulnar nerve, this distance was measured as a straight line from stimulating to recording site over ADM. All distances were measured, with a tape, and graduated in centimeters. Stimulus duration of 0.1 ms, filter band pass of 10 Hz–10 kHz, sweep speed and gain of 5 ms and 5 mV per division, respectively, were used. Distal motor latency (DML) of CMAP measured from stimulus artifact to point of sharp inflection from baseline and amplitude (peak to peak) were recorded in each waveform.
Transcarpal Motor Conduction Study
Keeping other factors unchanged, stimulus was delivered 3 cm proximal to DWC. Subsequent stimuli were delivered at 1-cm intervals up to DWC with cathode directed distally. For stimulation of recurrent thenar branch of median nerve in palm, stimuli were given at 1-cm intervals, along a straight line, connecting stimulation site at wrist crease, to second web space. Anode was directed distally towards the base of the little finger.1, 2 Care was taken to avoid direct muscle stimulation. During palmar stimulation, attention was paid to both twitch of thenar muscles and the recorded waveform. Stimulus intensity was increased gradually. In the palm, latency of the pure median CMAP was noted. While stimulating the thenar branch of median nerve, it was observed that the most distal site in palm, where a pure median CMAP was consistently obtained, was 3 cm from DWC. Hence, the latency of the median CMAP at this site was used while calculating TCMCV (calculated as distance between sites of median nerve stimulation, 3 cm proximal to DWC and 3 cm distal to it divided by difference in latencies between these sites). The same distance was used to calculate TCMCV in cases and controls.
Sensory NCS
Median and ulnar sensory nerve action potentials (SNAPs) were recorded by antidromic stimulation at wrist, 3 cm from DWC. Recording electrode (G1) was at metacarpophalangeal joint, reference electrode (G2) 3 cm distal to it with ground electrode over dorsum. Filter settings were 20 Hz to 3 kHz; sweep speed and gain were set at 2 ms and 5 mV per division, respectively. SNAPs were obtained from index, (D2) ring (D4), and little (D5) fingers. Distal sensory latencies (DSL) from stimulus artifact to onset of SNAP were used to calculate sensory nerve conduction velocities. Difference between onset latencies of SNAP of median and ulnar nerves (M-U) to D4, measured at identical distances (12 cm each) from active electrode was noted.
For diagnosis of CTS, the electrophysiological criteria adopted were: M-U > 0.4 ms, DSL (median) > 3.5 ms, and DML (median) > 4.4 ms. 10
Clinical Assessment
The Boston Carpal Tunnel Questionnaire (BCTQ), 11 comprising of scales to assess symptom severity (SSS) and functional status (FSS) was used for each patient included in the study before treatment and at each follow-up visit. It was applied before electrophysiology studies.
In order to reduce investigator bias, nerve conduction data of both patients and controls were in the possession of one investigator (Subhankar Kumar (S.K.)), who did not participate in examination of cases and controls. Records of BCTQ were kept by Subhankar Halder (S.H.), who had no access to electrophysiological records or clinical findings of subjects. The investigator, performing electrophysiology studies, was unaware of NCS data and scores of BCTQ.
Therapy
Patients fulfilling both clinical and electrophysiological criteria of CTS were treated with a single dose (40 mg) of intracarpal methylprednisolone, by one rheumatologist (Parasar Ghosh (P.G.)).
Statistical Analysis
Data obtained were analyzed using GraphPad Prism ver. 5.01 for Windows 7 (GraphPad software, San Diego, California).
Results
Repeatability Study
Difference (∇V) between repeat measurements of TCMCV was calculated for each subject. A scatter plot of ∇V against mean value of the TCMCV of each control subject was drawn to check for the presence of any association between them. Mean and standard deviation (S.D.) of values of (∇V) pooled across all subjects were obtained. Frequency distribution of ∇V was obtained by drawing a histogram (operator selected class intervals) to ascertain whether 95% values of ∇V fell within two S.D. of the mean (Figure 1). These measures were in accordance with those necessary to prove repeatability of a measurement. 12 The cut-off value of (∇V) obtained in this study was ±8m/s (95% Confidence Interval of the distribution of random values of ∇V).
Histogram of Difference Between Successive Readings of Transcarpal Motor Conduction Velocity.
Figures 2(a) and 2(b) show tracings of TCMCV in one hand of a control.
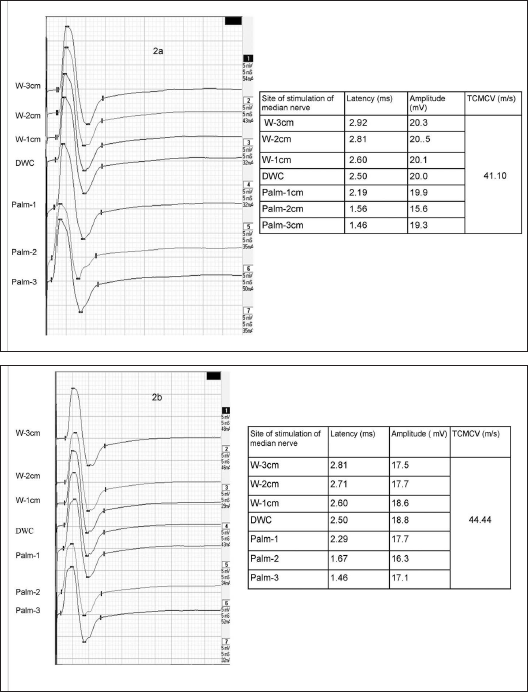
(a) Recording 1. (b) Recording 2.
Patients
TCMCV was recorded initially and at each follow-up visit at 1 month, 2 months, and 3 months after treatment. Difference between post-treatment (at 3 months) and pre-treatment TCMCV values was noted to calculate change in TCMCV with treatment. Similarly, difference between values of SSS and FSS, 3 months after treatment and their pre-treatment values, was used to evaluate changes in scores of symptoms and function status. In four patients (three unilateral cases and one hand of a bilateral case), there was improvement in TCMCV (increase in TCMCV greater than two standard deviations of distribution of (∇V), with consistent improvement in SSS and FSS. In one hand of a patient there was decrease in TCMCV, with improvement in SSS and FSS. In the remaining cases, changes in TCMCV and scores were inconsistent.
Thus, in four affected hands of four patients, there was improvement in both TCMCV and symptom and function status scores. This change in TCMCV corroborated qualitatively with change in SSS and FSS, suggesting true change in disease with treatment. Correlation between change in SSS and change in TCMCV at 3 months after treatment is shown in Figure 3.
Correlation Between Change in Symptom Severity Scale and Change in TCMCV at 3rd Month After Treatment.
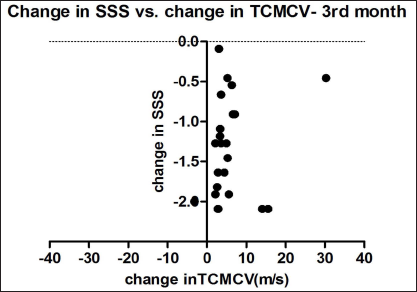
Table 1 shows data of patients with change in TCMCV (∇TCMCV) at each visit after treatment.
Electrophysiological and Clinical Data of 19 Patients Before and After Treatment with Change in Transcarpal Motor Conduction Velocity at Different Time Points.
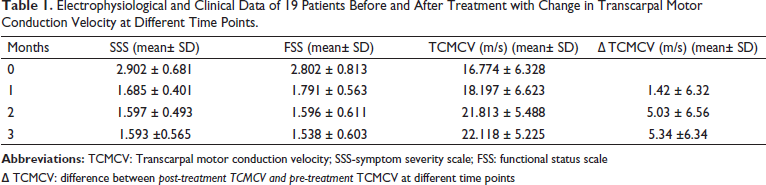
∇ TCMCV: difference between post-treatment TCMCV and pre-treatment TCMCV at different time points
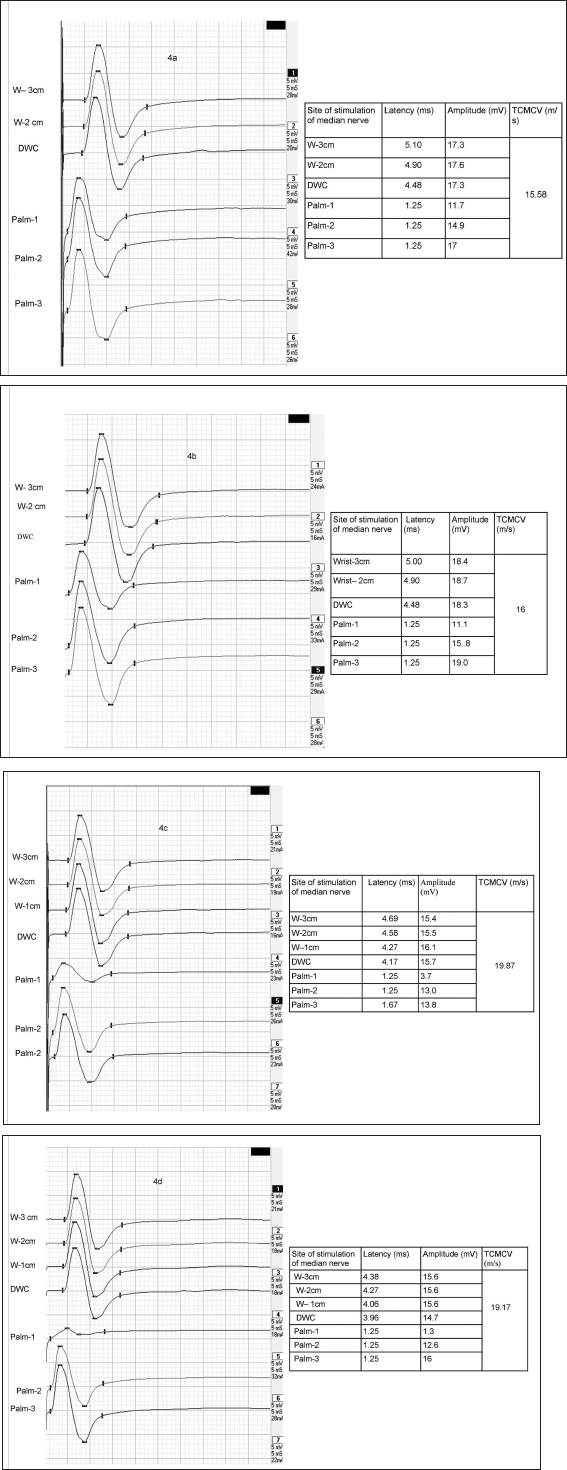
Figures 4 (a–d) show recordings of TCMCV before and at each follow-up visit in one hand of a patient.
CMAPs Recorded from Abductor Pollicis Brevis in a patient, Before and After Treatment, Stimulating Median Nerve 3 cm Above DWC (W-3 cm) to 3 cm Below DWC in Palm (Palm-3). TCMCV Are Shown Alongside. TCMCV Was Calculated Between W-3 cm and Palm-3. (a) Before Treatment. (b) 1 Month After Treatment. (c) 2 Months After Treatment. (d) 3 Months After Treatment.
Discussion
The primary goal of this study was determination of repeatability of conduction velocity of the transcarpal motor segment of the median nerve in normal subjects, so that it may be applied in cases of carpal tunnel syndrome treated with intracarpal steroid injection. We first probed this aspect of variability, between repeat measurements, of short-segment (transcarpal) motor conduction velocity. The mean coefficients of variation of TCMCV for left and right hands were 4.96% and 5.28%, respectively (data not shown). This was similar to the findings of forearm ulnar nerve motor conduction velocity reported in an earlier study. 7 In the above study, it has been suggested that primarily demyelinating conditions with reduced conduction velocity, upon treatment may show considerable improvement. The demonstration of the statistical significance of such improvement will require fewer subjects. In a subsequent study performed in rodents, with implanted epineural electrodes on lower limb nerves, the intra-day variability of NCV was less than 2%, suggesting that, study of effectiveness of therapy on nerve conduction velocity is possible with fewer samples. 13 We incorporated these suggestions while planning this study. To the best of our knowledge, till date no other interventional study of CTS has been carried out using repeatability of TCMCV for assessment of response to treatment.
In this study, TCMCV was measured over 6 cm in cases and controls, similar to the distance (approximately 5 cm) used to calculate TCMCV in an earlier study. 4 The mean TCMCV in our controls (26 subjects TCMCV 35.5± 6.4m/s) was less than that reported in the study mentioned above (69 controls, TCMCV 46.7± 5.8m/s). Mean value of TCMCV in cases in our study (26 hands, TCMCV= 16.77± 6.32 m/s) was less than the same parameter in cases reported in studies conducted by Walters and Murray (70 hands, TCMCV= 32.3 ± 9.7 m/s) and Digueglielmo (148 hands, TCMCV = 22 ± 8.1m/s).3–4 It was observed that in most controls and cases, stimulation of the recurrent thenar branch of median nerve in palm, at more than 3 cm from DWC, resulted in a CMAP with features consistent with ulnar nerve co-stimulation, proving spread of the stimulus to the deep branch of the ulnar nerve in palm. This finding was similar to that reported in two earlier studies.4, 14
The insignificant correlation between change of symptom status and change in TCMCV proves the independence of these parameters, in assessing outcome of treatment, similar to observations of other studies.15–16
This study was limited to a short follow-up period of 3 months after treatment, during which maximum change in median motor conduction velocity has been reported by most studies.15–16
On the basis of our observations, the following suggestions may be made:
For any “before-after comparison” made by observing change in a parameter, repeatability (precision) of the measurement of the parameter must be assessed. So, it is important to assess the repeatability of TCMCV when using it as an indicator of response to treatment.
In measuring NCV of the transcarpal segment of median nerve, the distance between the proximal and distal sites of stimulation was 6 cm, same distance as used by other authors in their study. 4 The stimulator knobs were 1 mm in radius, which introduced a millimeter uncertainty in location of a stimulation site. A millimeter uncertainty in measuring a 6 cm distance leads to 1.7% uncertainty in velocity calculation. This uncertainty is inherent in all short segment measurements.
Due to this finite uncertainty in measurement of short segment NCV, the difference between successive measurements ∇V is a random variable expected to have a Gaussian frequency distribution with zero mean. Then 95% of such random differences ∇V will be within two SD of this distribution of ∇V, on either side of zero. A difference ∇V greater than two SD of this distribution of ∇V will signify a true change in NCV with p < .05, given that the same instrument is used by the same operator for all measurements.
Each operator must obtain the distribution of random ∇V for the particular instrument to be used for all measurements, check whether it fits the Gaussian distribution, and calculate SD of the distribution.
This is just the prescription of British Standards Institution for all “before-after comparison,” applied here in this article to the issue of short segment NCV exemplified by transcarpal segment of the median nerve.
We also observed that in some cases, locating the site of stimulation in palm, was difficult. This is due to the course of this part of median nerve in palm and thickness of transverse carpal ligament. 8 Kimura has also observed the same difficulty in locating the site of stimulation in palm in his work (Kimura, 1979). 14 Due to this technical difficulty, transcarpal NCV may not be measurable at all in a few cases of CTS. But this difficulty does not affect precision of measurement, where the transcarpal NCV can be measured at all.
Conclusion
Short segment NCV such as TCMCV can be used to detect response to therapy in local compressive neuropathy such as CTS, provided the following criteria of British Standards Institution are met:
The random variations of measurement are found to have a Gaussian distribution with zero mean;
The 95% confidence interval of random variation is determined from this distribution;
The corresponding p-value (< .05) is indicated in the interpretation of changes in short segment NCV as a random difference or a true response to therapy.
Footnotes
Acknowledgements
The authors would like to thank Dr. Gitabali Sircar, Department of Rheumatology and Clinical Immunology, IPGME&R and SSKM Hospital, for her logistic support during this project and Dr. Sangita Sen, Department of Physiology, IPGME&R for her guidance during preparation of the manuscript. The data supporting findings of research are available on request from corresponding author. Data are not available publicly due to privacy and ethical restrictions.
Authors’ Contribution
P.D. Design of study, performing electrophysiological study of subjects, and writing manuscript.
P.G.: Selection of patients for study, their treatment and follow-up.
S.K.: Concept of study, statistical analysis of data, reviewing, and editing manuscript.
S.H.: Selection of cases, administering questionnaire and maintaining all clinical data till conclusion of study.
Statement of Ethics
Prior to start of the study, approval was obtained from the Institute Ethics Committee (approval letter Inst./IEC/1062). The study was carried out following the guidelines for human research, in accordance with the World Medical Association Helsinki Declaration. Written informed consent was obtained from all cases and controls.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.