
Abstract
Background:
There is a lack of clarity about the cognitive dysfunction in young patients with subclinical hypothyroidism (SCH). This study was done to explore the neuropsychological impairments in young patients with SCH and compare them with euthyroid controls.
Methods:
Patients between 18 and 45 years of age and diagnosed with SCH were recruited. Controls were euthyroid age, gender, and education matched. All the cases and controls underwent a detailed neuropsychological assessment with a battery of tests validated for use in the age groups of 18 to 65 years.
Results:
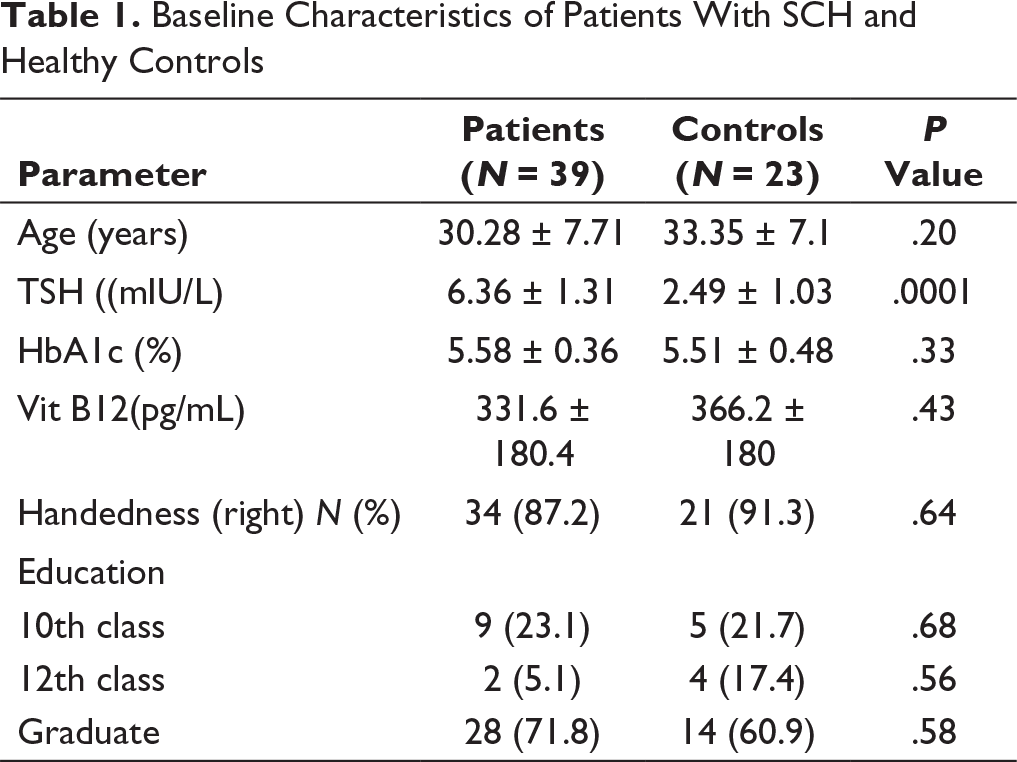
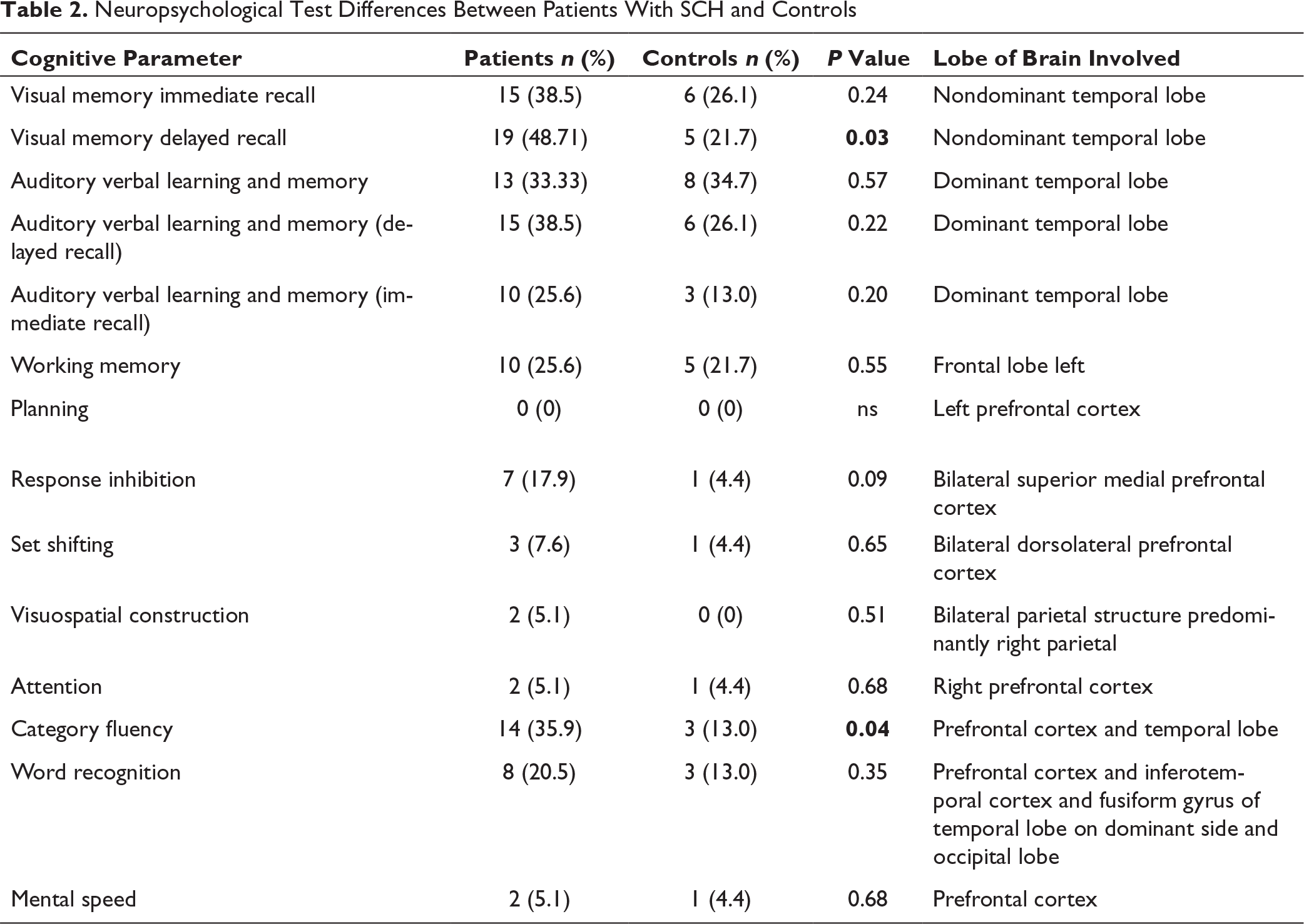
Thirty-nine patients with a mean age of 30.3 ± 7.7 years (female:male ratio 12:1) and 23 controls (female:male ratio 21:2) with a mean age of 33.4 ± 7.1 years (P = .24) were included in the study. The mean TSH value was 6.36 ± 1.3 mIU/L and 2.49 ± 1.03 mIU/L in cases and controls, respectively (P < .001). The visual memory delayed recall was impaired, in 48.71% (n = 19) and 21.7% (n = 5) cases and controls, respectively (P = .03). The category fluency test showed impairment in a greater number of cases (35.9%, n = 14) as compared to controls (13%, n = 3; P = .04).
Conclusion:
This study shows that younger patients with SCH have delayed visual memory recall and category fluency deficits, which are suggestive of dysfunction of the prefrontal cortex and temporal lobe in young SCH patients. These impairments may justify the treatment of young SCH patients with replacement therapy.
Introduction
Thyroid hormones are critical for the normal functions of the brain. They are very crucial for the areas of the hippocampus, especially the dentate gyrus and CA1 and CA3 regions. These regions are vital in learning and for memory and contain abundant thyroid hormone receptors. Consequently, there are implications on synaptic plasticity and neurogenesis in the hippocampus if any changes occur in the level of thyroid hormones. 1 Subclinical hypothyroidism (SCH) is a condition characterized by TSH levels between 4.5 and 10 mIU/L, with normal T4 levels. 2 The studies done in patients with SCH have revealed a heightened incidence of coronary heart disease, dyslipidemia, cardiac autonomic dysfunction, and endothelial dysfunction. 3
Studies have also shown that in situations of experimentally produced thyroid inefficiency, many important alterations occurred in the meninges, particularly in pia mater and in brain cells. A notable finding was the alterations in the vessels of the microcirculation that lead to the impaired metabolism of mucopolysaccharides. These perturbations may account for the abnormalities in the function of the brain. 4
Newer imaging techniques like functional and quantitative MRI of the brain have shown significant differences in patients with hypothyroidism before and after levothyroxine replacement.5, 6
In mature adults, the thyroid hormones have an essential role in cognition, mood, and behavior, but the basic cellular and molecular mechanisms underlying this are not understood clearly. 7
Patients with SCH have shown conflicting results with regard to differences in the neuropsychological memory scores in comparison to healthy controls.8, 9 However, in patients with frank hypothyroidism, it has been shown that white matter fiber dysfunction may be a reason for the basic memory dysfunction. 10
The main objective of the study was to study the neuropsychological deficits in young adult patients with SCH and to compare them with euthyroid age, gender, and educational level matched healthy controls.
Methods
It was a prospective, case-controlled, hospital-based study involving the Departments of Endocrinology, Neuropsychology, and Neurology in two tertiary care centers in Bangalore, India. All procedures performed in this study were in accordance with the ethical standards of the institution and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The Institutional Ethical Committee approved the study.
Inclusion Criteria
The patients between the ages of 18 and 45 years and diagnosed as SCH as per the American Thyroid Association guidelines with a cutoff between 4.5 and 10 mIU/L on two different occasions two weeks apart were recruited. 2 Patients did not have diabetes and vitamin B12 deficiency and had a normal clinical neurological examination. Healthy controls were age, gender, and education matched with normal TSH values and normal neurological examination.
Exclusion Criteria
Patients with type 2 diabetes mellitus and prediabetes, patients on antiplatelet drugs, any neurological, neurodegenerative disorder, psychiatric disorder, history of stroke, history of transient ischemic attack at the time of presentation, any history of significant head injury, any history of intracranial surgery, patients with vitamin B12 deficiency, and known immunocompromised states (HIV) were excluded from the study. The controls were euthyroid (TSH between 0.45 and 4.5 mIU/L), thyroid peroxidase antibody negative, with no goiter, and no family history of thyroid disorder in first-degree relatives.
Study Assessments
The patients and controls underwent the following evaluation. Detailed anthropometry was recorded for all the patients. The patients and controls underwent TSH testing and also a baseline HbA1c to rule out diabetes. Neurological assessment was done by clinical history, examination and detailed neuropsychological tests, including depression and anxiety scales.
Neuropsychological Tests
The following neuropsychological tests were carried out in this study: (a) MMSE (Mini-mental status examination), (b) digit symbol substitution test (mental speed), (c) digit vigilance test (focused attention), (d) animal naming test (category fluency), (e) N-back test (verbal working memory), (f) planning test (tower of London), (g) Stroop test, (h) Wisconsin card sorting test (WCST), (i) auditory verbal learning test (AVLT), and (j) complex figure test (CFT). These tests have been validated for neuropsychological testing in patients with hypothyroidism in previous studies. 11
Statistical Analysis
For the comparison of means among the two groups (cases and matched controls) in terms of the neurocognitive test performance, the optimal sample size was estimated using the standard principles and methods for a t-test with Wilcoxon signed-rank test (matched pairs), a moderate effect size of 0.50, α error probability 0.05, and 80% power. The total sample size calculated was 35. The sample size was calculated using G-power software (
The mean and standard deviation were calculated for parametric variables. The parametric variables were compared by Student’s t-test and nonparametric by Mann–Whitney test. The comparison for categorical variables was made by chi-square test. The P-value of less than .05 was taken as significant. Holm–Bonferroni method was applied for multiple variables.
Results
Thirty-nine patients with a mean age of 30.28 ± 7.7 years (female:male ratio 12:1) and 23 controls (female:male ratio 21:2) with a mean age of 33.4 ± 7.1 years (P = .20) were enrolled. The mean TSH value in cases was 6.36 ± 1.3 mIU/L and in controls was 2.49 ± 1.03 mIU/L (P < .001). Vitamin B12 deficiency was ruled out biochemically in all patients. HbA1c was done in all cases and controls to rule out diabetes mellitus (values less than 5.7%). There was no difference in the education status of the two groups (P = .61). The category fluency test was impaired in 35.9% (n = 14) patients as compared to 13% (n = 3) in controls (P = .04). The visual memory delayed recall, which is a function of the nondominant temporal lobe, showed an abnormality in more number of cases as compared to controls 48.71% (n = 19) and 21.7% (n = 5; P = .03). The demographic profile and baseline characteristics of the patients and controls are given in Table 1. The cognitive test comparisons are given in Table 2.
Baseline Characteristics of Patients With SCH and Healthy Controls
Neuropsychological Test Differences Between Patients With SCH and Controls
Discussion
The results in our study show important neuropsychological deficits in patients with SCH. The salient observations of statistically significant deficits in category fluency and visual memory delayed recall are the hallmarks of this study. These point out the presence of executive dysfunction and nondominant temporal lobe dysfunction.
The cognitive deficits in SCH have been studied in some of the previous reports in heterogeneous age groups of patients, including the children and elderly.12–19
Studies performed by Sangun et al. in children suffering from mild SCH have shown that there is an improvement in verbal memory and verbal recall in these patients after treatment with levothyroxine. 20 The patients in this study had a TSH value between 5 and 10 mIU/mL, and the free T4 value was normal. These patients were assessed clinically and cognitively before and after levothyroxine treatments at six months follow-up. The battery of neuropsychological tests included those for attention, perception, close and remote memory in both cases and controls. Also, at baseline, the patients had statistically lower verbal memory and lower verbal recall scores as compared to healthy controls. Our study also shows a deficit in visual memory delayed recall in our subjects with SCH, but our population was of young adults. Although we have only done a cross-sectional study, our subjects underwent detailed tests using a validated battery of neuropsychological testing.
A study on 2,557 individuals from Germany combined data from two separate studies. The cutoffs of 0.40 and 3.29 mIU/L were defined for low and high TSH, respectively. People with high TSH had substantially lower total brain volume than those within normal range TSH, but low TSH was not significantly associated with brain volumes. Voxel-based morphometry analyses showed that serum FT4 levels were positively associated with the left middle frontal gyrus. 21
Our study results are also in concordance with the study done by Correia et al., who demonstrated the impairments of the hippocampal complex and prefrontal cortex in patients with SCH. 22 This area is responsible for declarative memory. In their study, 17 patients of SCH and 21 patients with hypothyroidism were assessed by tests of verbal, spatial, working, and associative memory, attention, and response inhibition anxiety and depression scales. After the replacement of levothyroxine, the patients were assessed again. It was found that spatial memory had become normal in the SCH group but did not improve in the hypothyroid group. Also, associative memory deficits persisted in the overt hypothyroid group. This study (mean age 50 ± 9.2 years) had a predominantly higher age group of patients, though with a mostly female population (16:1) like our study. The mean age of the patients in our study was much younger (30.28 ± 7.71 years), and they showed mainly executive dysfunction and delayed recall impairments.
These studies show that the cognitive deficits in patients with SCH can be detected by detailed neuropsychological tests. These impairments may not lead to overt intellectual decline but can reduce the optimal cognitive functioning of the individual with SCH. These changes may assume significance during a younger age where the cognitive challenges are overwhelming, both at work and personal level. There is also a pattern or continuity in the development of subtle cognitive abnormalities that begin during the phase of SCH and in patients with overt hypothyroidism. These involve more extensive cognitive domains, like executive dysfunction and spatial memory. 22
In the prospective study of pravastatin in the elderly at risk, 5154 participants aged 70 to 82 years were enrolled to evaluate the result in terms of vascular outcomes. They found that SCH was present in 161 patients. The authors did not find any consistent association of SCH with cognitive decline in the elderly. 23 This study was different from our study as they have taken older population and have not used an extensive battery of neuropsychological testing. The treatment of SCH in older subjects beyond 65 years has not shown any benefit in the vascular outcome or in neuropsychological parameters. The beneficial effects in the improvement of neuropsychological abnormalities have been seen in the younger population.
SCH has also been associated with atherosclerosis and a higher risk of ischemic stroke in various studies. In a study by Zhang et al., a risk of small vessel disease was evaluated in patients with SCH. Their results showed that these patients had a higher risk of development of white matter lesions and microbleeds in brain MRI even after the adjustment with the confounding factors. These changes can contribute to the cognitive status of a patient with SCH 24 . The patients included in this study were older, in the age range 66.6 ± 10.7 years, unlike our study, where the patients were much younger. The TSH cutoff was between 4.5 and 10 mIU/mL in this study, similar to our study.
A Japanese study evaluated 229 subjects who were 75 years or older and were free of dementia. SCH was diagnosed by the level of TSH level and FT4. Detailed geriatric assessments were performed at baseline and at one year follow-up. The results showed no difference between the cognitive decline in patients with SCH and healthy controls. 12 This study again had patients in the higher age group than our study, so it is difficult to compare it with our study.
The advanced imaging studies were done in patients with SCH by Kumar et al., who studied 28 patients of SCH and an equal number of controls with intrinsic and extrinsic functional connectivity of the resting-state networks. This unique study showed the level of impairment of motor, working memory, attention, and executive cognitive functions in SCH as well as the disruption of functional connectivity in these patients using functional MRI techniques. 25 The patients in this study had a mean age of 32 years, which is similar to our study.
The study done by Jorde et al. did not show any difference in cognitive tests after treatment with levothyroxine as compared to untreated patients of SCH. The subjects in the study had higher proportion of males as compared to our study. 9 This study also had subjects in the age group above 60 years, and TSH ranged from 5 to 10 mIU/mL.
Monzani et al. showed that after treatment with levothyroxine in patients with SCH, there was an improvement in memory skills, as evaluated by the Wechsler Memory Scale; somatic complaints, obsessionality ratings, and the Crown-Crisp Experiential Index total score (P = .04) significantly decreased with respect to untreated patients. 26 These results are in concordance with our study where we have seen abnormalities in category fluency and visual memory delayed recall.
Our study thus supports the presence of sub/clinical neuropsychological deficits in young Indian patients with SCH. These patients would show up as normal on the routine outpatient evaluation by cognitive screening tools like Mini-mental status examination or Montreal cognitive assessment battery. These patients have subtle cognitive deficits that would prevent them from being in an optimal level of cognition in their day-to-day living. The people who would be responsible for making critical decisions may falter because of these impairments in the executive functions and temporal lobe functions. The financial and personal implications of these impairments should be quantified by further studies.
Limitations of the Study
The limitations of the study are its cross-sectional design. The change in cognition after replacement with levothyroxine would provide critical data to assess the outcomes. The strength of the study is the age-, education-, and gender-matched controls, with detailed neuropsychological testing using a validated neuropsychological battery in young patients with SCH. The other factors that can impact neuropsychological assessment were ruled out.
The cutoff TSH value used in some previous studies was higher, but we have taken TSH above 4.5 mIU/mL as cutoff for diagnosis of hypothyroidism, and the mean TSH in our study was 6.36 ± 1.61 mIU/mL, and even then, impairments in the neuropsychological profile were shown in the young patients with SCH as compared to controls.
These changes in the neuropsychological profile have an impact on the productivity of a person as they are in the peak of their career, and these so-called minor deficits may have a bearing and thus may be taken care by replacement with levothyroxine if needed.
To conclude, our study shows that patients with SCH have neuropsychological deficits in executive functions and temporal lobe functions that would go undetected by conventional screening tests. These deficits may impair the optimal performance of individuals with SCH.
Footnotes
Declaration of Conflicting Interests
Ethical Statement
This study was approved by IEC (Institutional Ethical Committee). All the participants were briefed about the study and were involved after taking the written informed consent.
Funding
The authors received funding for research from the Endocrine Society of India grant number R2015001.