
Abstract
Background and Objectives:
Migraine is one of the major headache disorders. Epidemiological studies have shown its high prevalence and negative impact on personal and socioeconomic aspects. It is currently ranked 19th by the “World Health Organization” amongst all diseases, leading to disability worldwide. Inflammatory mediators, which include adipokines, have been analyzed in migraine pathophysiology. Nevertheless, their role is not well recognized. This study is aimed to assess serum high molecular weight adiponectin (HMW-ADP) levels in migraineurs: during the ictal phase, prior to, and postabortive treatment.
Methods:
This was a hospital-based interventional case-controlled study, checking the peripheral blood samples from migraineurs during an acute attack and after one hour of treatment with naproxen sodium (10–15 mg/kg). Age, sex, and BMI matched controls without headache were taken, and a single blood sample was drawn in them. HMW-ADP levels were evaluated by immunoassays.
Results:
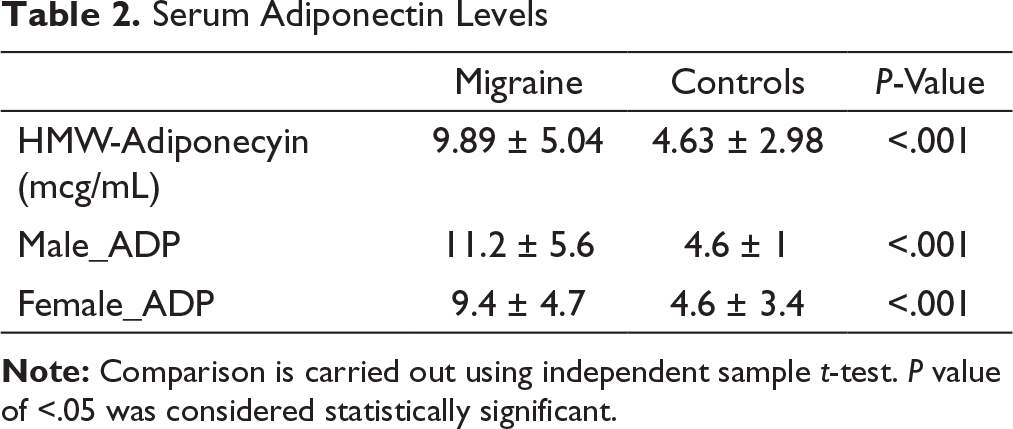
A total of 120 patients which included 60 migraine patients along with 60 controls without headache were involved in the study. HMW-ADP was higher in migraine patients (9.89 ± 5.04 mcg/mL) than in patients without headache history (4.63 ± 2.98 mcg/mL; P = < .001); along with this, serum HMW-ADP (6.4 ± 4.09 mcg/mL; P = <.001) was found to be significantly lower in responders 60 min after acute abortive treatment.
Conclusion:
HMW-ADP levels were raised in migraineurs. Additionally, among responders following abortive treatment a considerable reduction in the levels was noted. These results recommend that the HMW-ADP might be a possible “novel biomarker of acute remedy response in acute migraineurs”.
Introduction
The World Health Organization lists headache disorders among the ten most incapacitating diseases for both genders. But even after being so common, the approaches for headache disorders are not well established globally, and their burden is underestimated. Migraine ranks as one of the most common headache disorders that is not caused by a structural lesion of head and neck. Occurrence is maximum between the ages of 25 and 55 years, and more specifically between the ages of 35 and 45 years, which corresponds to the prime working years and hence adds to the economic burden.1, 2
For several years, migraine has been hypothesized to be a “vascular” disorder. The traditional view of pathophysiology of migraine has been that of arterial spasm within the internal carotid territory resulting in the aura, followed by dilatation in the distribution of the external carotid artery, resulting in the headache. Cortical spreading depression was postulated to result in a distribution of a wide array of chemicals which when released into the meninges were thought to “activate the trigeminal nociceptors,” leading to the consequent development of headache. 3 These agents consist of calcitonin gene-related peptide, potassium, excitatory amino acids, substance P, arachidonic acid, nitric oxide, and neurokinin A. 4 Obesity has also been related to a higher migraine risk, with worse migraine prognosis including frequent attacks of greater magnitude. Adipose tissue secretes numerous inflammatory cytokines such as interleukin 6, tumor necrosis factor, and adipokines [adiponectin (ADP) and leptin], which are contributory to obesity and have been incriminated in migraine pathophysiology. 5 New and emerging information shows the active involvement of adiponectin in pathological and physiological processes related to immunity, inflammation, and insulin sensitivity.6–8 Studies have shown that total and “high molecular weight adiponectin” levels are increased and “low molecular weight adiponectin” levels are decreased in migraineurs, especially during acute attacks. 9
Migraine pathophysiology is complex, and no adequate theory exists till date to encompass all of the observations and, no doubt, many further molecular candidates will be proposed. There is no specific investigation to confirm the diagnosis of migraine or to assess the outcome of treatment. Recent studies have shown that obesity has a contribution in migraine pathophysiology via the neuroinflammatory model. Adiponectins, which are secreted by the adipocytes, play a plausible role in migraine pathophysiology. Studying adiponectins may further cement the theory of obesity and migraine correlation and thus may throw light on the etiological mechanisms underlying migraine episodes, possibly serving as a potential biomarker for migraine. 10 This in turn may open doors for more therapeutic strategies in migraine.
The present study aims to analyze blood ADP levels in healthy controls as well as migraine patients, in acute migraineurs–pre and posttreatment and to compare headache severity scales with ADP levels.
Methods
This is a prospective hospital-based interventional case-controlled study, which includes patients with migraine as well as controls with no headache, recruited from 2019 August to 2019 December. The migraine patients have been registered “from the outpatient headache clinic of the Department of Neurology”, JSS hospital, Mysore. Every migraine diagnosis has been made according to the “International classification of headache disorders–beta 3 edition.” 11 Patients willing to participate in this study were recruited after informed consent.
The minimum age for the patient and control to be included was 18 years. Control subjects were recruited via active 1search between healthy volunteers accompanying patients and were age, sex, and BMI matched with the cases. Exclusively subjects with no record of headache have been involved in the control group. Patients and controls with diabetes, hypertension, neoplasms, and infectious, allergic, neurodegenerative, autoimmune, inflammatory, hepatic diseases as well as expecting women and people who are using drugs acting on the immune system had been excluded from the research. A total of 120 patients, which included 60 with migraine and 60 without headache as controls, were included in this research after they met the inclusion criteria. 12
Demographic data (sex, age, marital status), headache characteristics (frequency in a month, duration of each attack, duration of headache), and BMI (body mass index) had been recorded. “Headache impact test” (HIT-6) 12 had been recorded for every patient with migraine. Numeric pain rating scales (NPRS) 13 were calculated and recorded for patients with acute episode—pre and posttreatment with naproxen at a dosage of 10–15 mg/kg. 14 For our study, the cases who demonstrated a reduction of two points, or ≥30% on NPRS scores 60 min after treatment with naproxen sodium, were considered as responders and the rest were considered as nonresponders.
The AssayMax Human 1Adiponectin ELISA Kit used was created for adiponectin detection in saliva, milk, serum, human plasma, urine, along with cell culture supernatants. The test employed “a quantitative sandwich enzyme immunoassay” method that measures adiponectin in less than three “hours. A polyclonal antibody specific for” adiponectin was precoated on 96-well microplates with detachable strips. Adiponectins in standards and specimens were interposed “by the immobilized antibody” along with a “biotinylated polyclonal antibody specific for” adiponectin, which had been identified with the help of “streptavidin–peroxidase conjugate”. All the unbound materials were subsequently washed 1away, and a peroxidase enzyme substrate was then incorporated”. The color advancement was stopped and the color’s intensity was evaluated. From every participant, 5 mL of entire blood had to be collected. The serum was procured after centrifugation and kept at –40°C until the test. ELISA test was carried out for serum HMW-ADP level determination, based on the instructions provided by the company. The assay settings were managed, preoptimized, and standardized to guarantee reproducibility and repeatability of the analysis based on the instructions supplied by the company.
SPSS version 15.0 for windows was used for the testing of data. The confidence 1interval and significance level for this study were considered to be 95% and P < .05, respectively. The verification of” data’s normal distribution had been conducted utilizing the “Kolmogorov–Smirnov test.” The comparison of means of continuous data was done by Mann–Whitney test. Demographic aspects have been compared utilizing “chi-square tests. The correlation assessment between ADP levels and” the other continuous variables was executed with the Spearman correlation test.
Results
A total of 120 patients (60 with migraine and 60 controls) had been included in this research after they met the inclusion criteria. Out of 60 cases, 46 (76%) were females and 14 (24%) were males. Out of the 60 patients, 42 (70%) with migraine had episodic migraine and the rest had chronic migraine (30%). Migraine with aura has been diagnosed in four (6%) of the patients. There was no significant difference in gender, age, and BMI among both groups.
Clinical and Demographic Characteristics
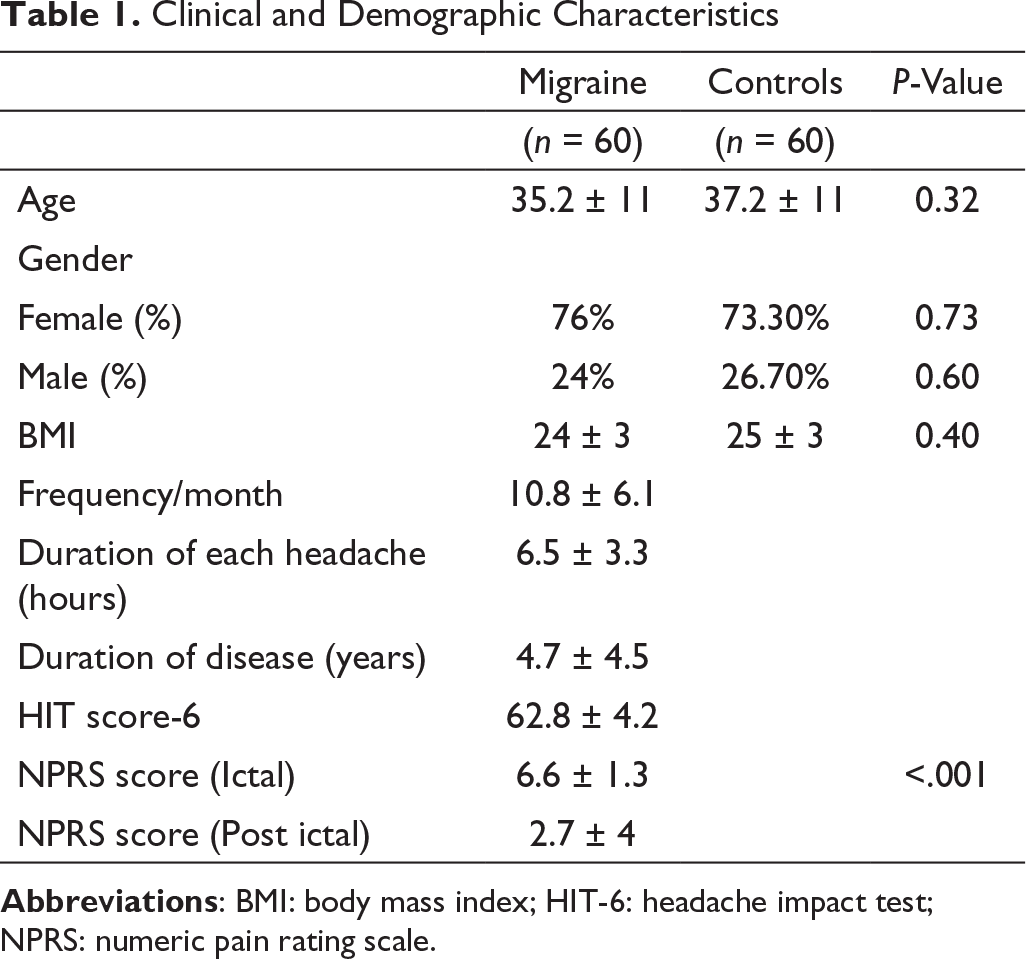
Comparison is carried out using independent sample t-test. P value of <.05 was considered statistically significant.
Serum Adiponectin Levels
HMW-ADP: Responders Vs. Nonresponders
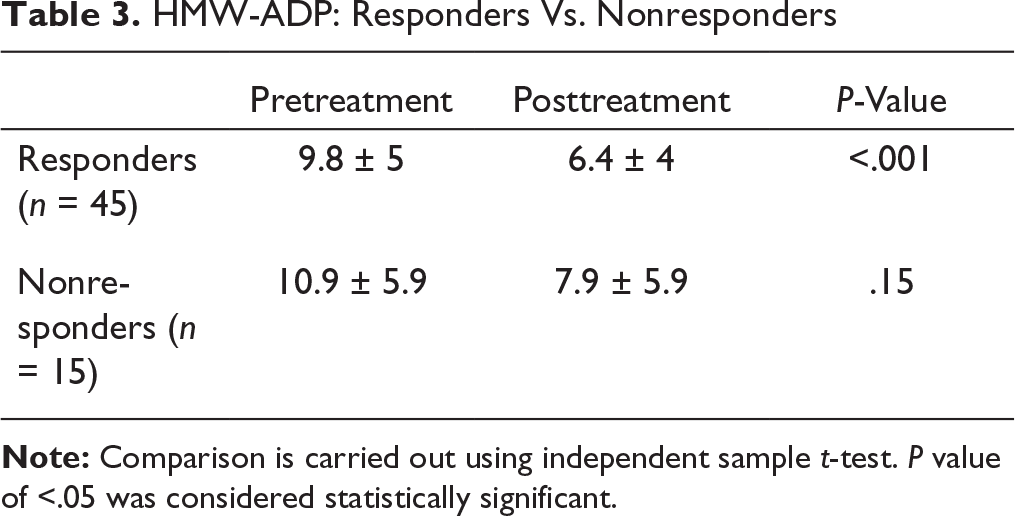
Note: Comparison is carried out using independent sample t-test. P value of <.05 was considered statistically significant.
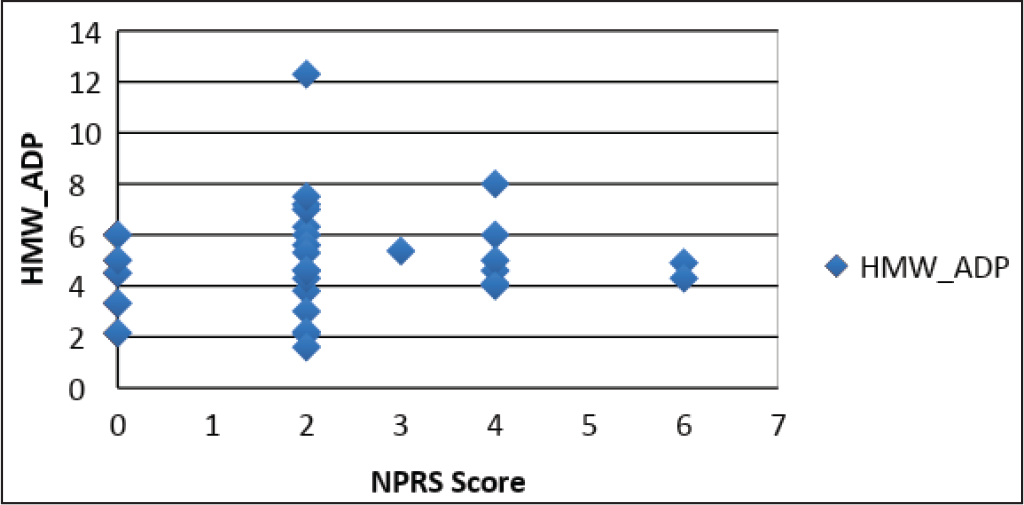
For every one-point decrease in mean NPRS, a decrease of 2.1 µg/mL of mean serum HMW-ADP was seen among responders (Figures 1 and 2).
Scattered plot : NPRS score VS HMW_ADP(Post treatment)
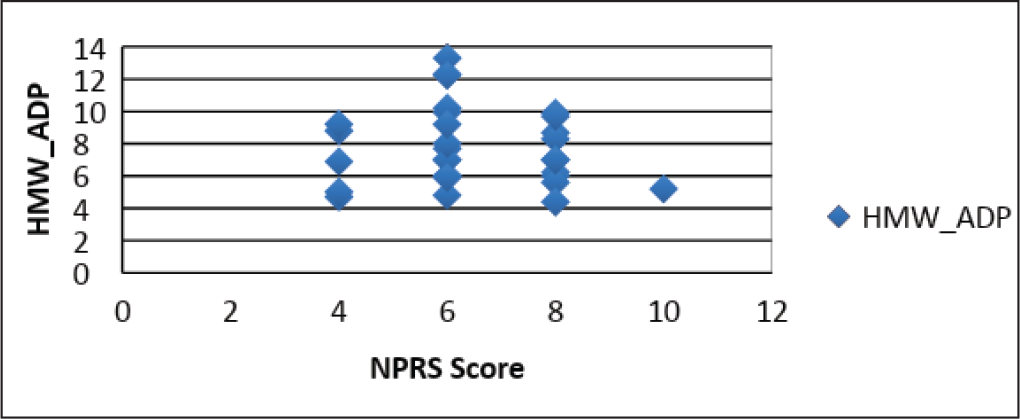
Scattered plot : NPRS score VS HMW_ADP(Post treatment)
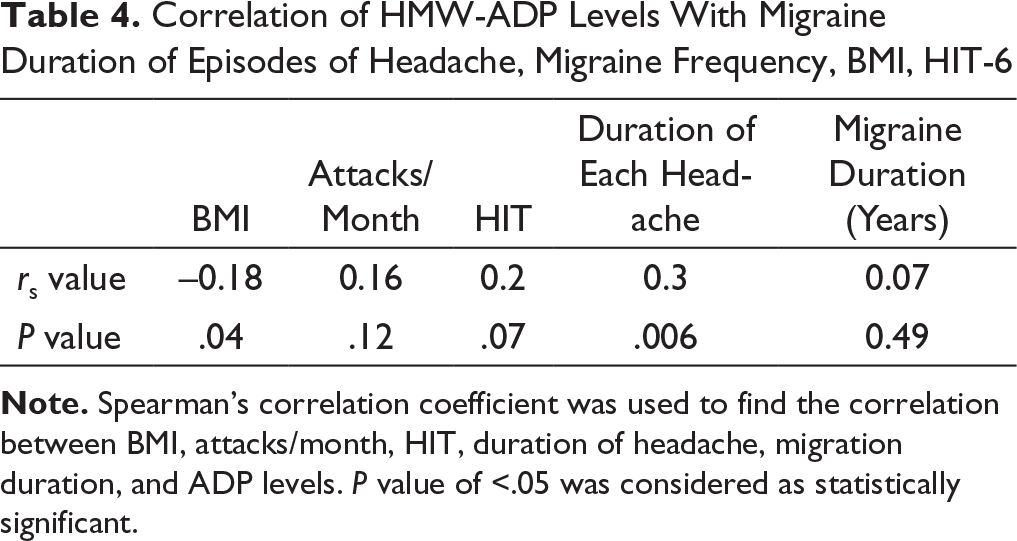
Correlation of HMW-ADP Levels With Migraine Duration of Episodes of Headache, Migraine Frequency, BMI, HIT-6
Discussion
Adiponectin is involved in the pathophysiology of migraine because of its involvement in the modulation of cytokines and nitric oxide, influence on sex hormones and prolactin, and action on the hypothalamus and shared genetic mechanisms. Adiponectin exists as LMW-ADP “low molecular weight,” MMW-ADP “middle molecular weight,” and HMW-ADP “high molecular weight” types. High molecular weight isomers are found in circulation (HMW-ADP) and also in the cerebrospinal fluid. These isomers are capable of modulating inflammation and endothelial functions in the body, which overlap with the proposed pathophysiology of migraine.15, 16 Among the isomers, HMW-ADP has a pro-inflammatory and LMW-ADP an anti-inflammatory property. These isomers bring about their function with the help of various pathways, which are also known to be implicated in migraine pathophysiology. 8
Prostaglandins such as PGE2, prostaglandin I2 (PGI2), and prostaglandin D2 (PGD2) by virtue of their action on trigeminovascular system are implicated in pathogenesis of pain in migraine. Naproxen reversibly inhibits both the COX-1 and COX-2 enzymes, resulting in the inhibition of prostaglandin synthesis and hence relieves pain associated with migraine. Numerous studies conducted to study the efficacy of naproxen sodium as an abortive therapy in acute migraine have confirmed the beneficial effect of the drug. 17 Adverse effects commonly encountered with naproxen like nausea, dizziness, dyspepsia, abdominal pain, palpitations, and edema 17 were not observed among our study participants.
In the present research, the baseline HMW-ADP levels was increased in migraineurs and HMW-ADP levels reduced significantly in responders after successful acute abortive therapy. These findings were in line with the analysis conducted by Duarte et al. In their cross-sectional study, which included migraine patients as well as controls, they detected high ADP levels in migraineurs and concluded that these elevated levels had no correlation with coexisting psychiatric dysfunction, migraine severity, or allodynia. 18 Similarly, Peterlin et al., who estimated ADP levels in various forms of headache disorders, noted higher ADP levels in patients with migraine in comparison to controls. 19 Further HMW-ADP levels reduced significantly after successful acute abortive therapy. Similar results were observed in an analysis conducted by Chai et al., where they found a significant decrease in total ADP, HMW-ADP, and an increase in LMW-ADP two hours after treatment as compared to the onset. 20
Abbasi et al. 21 in their study, using systematic reviews and meta-analyses, concluded that the blood levels of leptin and adiponectin of the migraineurs were associated with disease pathogenesis.
Elevated levels of serum adiponectin, leptin, and other inflammatory molecules were found in migraineurs as compared to healthy controls in a study by Dominguez et al., 22 thus strengthening their role in migraine pathophysiology.
Our study also shows “that ADP levels are not” dependent on the frequency of migraine attacks or duration of migraine in the patients (years), as we did not discover any association between them and the ADP levels, thereby explaining why HMW-ADP levels are not significantly different among “chronic and episodic migraineurs”. Our analysis concluded “that the ADP levels are not” associated with migraine impact (HIT-6 score), therefore signifying “that the HMW-ADP levels do not correlate with migraine severity. However, a significant association was found between BMI, duration of each headache attack (hours), and HMW-ADP levels.
Hence, we suggest that the HMW-ADP could have a role in adding newer insights “to the pathophysiology of migraine”, assessing treatment response, and being a novel therapeutic target. Not measuring various ADP oligomers, which have been implicated to have a role in migraine pathophysiology, and not accounting for sex hormones are the drawbacks of this study. Larger multicentric prospective studies are warranted in the future to strengthen the probable relation linking ADP levels and other oligomers in migraine.
Conclusion
Our study supports that HMW-ADP levels are high in migraineurs as compared to controls. Among patients who respond to medication, there is a significant drop in the levels of HMW-ADP. These results suggest that the HMW-ADP could be a possible novel biomarker in migraineurs.
Author Contributions
Siddarth S. Joshi, Nemichandra S. C. were involved in conceptualizing and designing the study, review of clinical studies and literature, acquisition of data, statistics, preparation, and editing of manuscript. Harsha S., Akhila Prasant and Shasthara P. were involved in designing the study and preparation of manuscript. Roshan Iqbal was involved in acquisition of data, preparation, and editing of manuscript. Vimala Colaco was involved in data collection, manuscript editing, and revision.
Footnotes
Declaration of Conflicting Interests
Ethical Consideration
The research has been authorized by the Institutional Ethical Committee of JSS Medical College [JSSMC/IEC/2308/12 NCT/ 2019-20, (03/09/19)].
Ethical Statement
IEC (Institutional Ethical Committee) approved this study. Written informed consent was taken from all the participants after briefing about the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.