
Abstract
Background:
Medical residents are vulnerable to poor sleep quality due to intense work shifts and academic load. Studies objectively quantified with sleep quantity and quality among resident physicians are limited. Meditation techniques have been shown to improve sleep but are rarely studied in this population. The aim of the present study is to evaluate sleep patterns of internal medicine residents and the effect of a structured Heartfulness meditation program to improve sleep quality.
Methods:
A total of 36 residents participated in a pre–post cohort study from January 2019 through April 2019. Sleep was monitored during a one-week outpatient rotation with two validated assessment tools, namely consensus sleep diary and actigraphy. After four intervening weeks, when the residents returned to the same rotation, Heartfulness meditation was practiced and the same parameters were measured. At the end of the study period, an anonymous qualitative feedback survey was collected to assess the feasibility of the intervention.
Results:
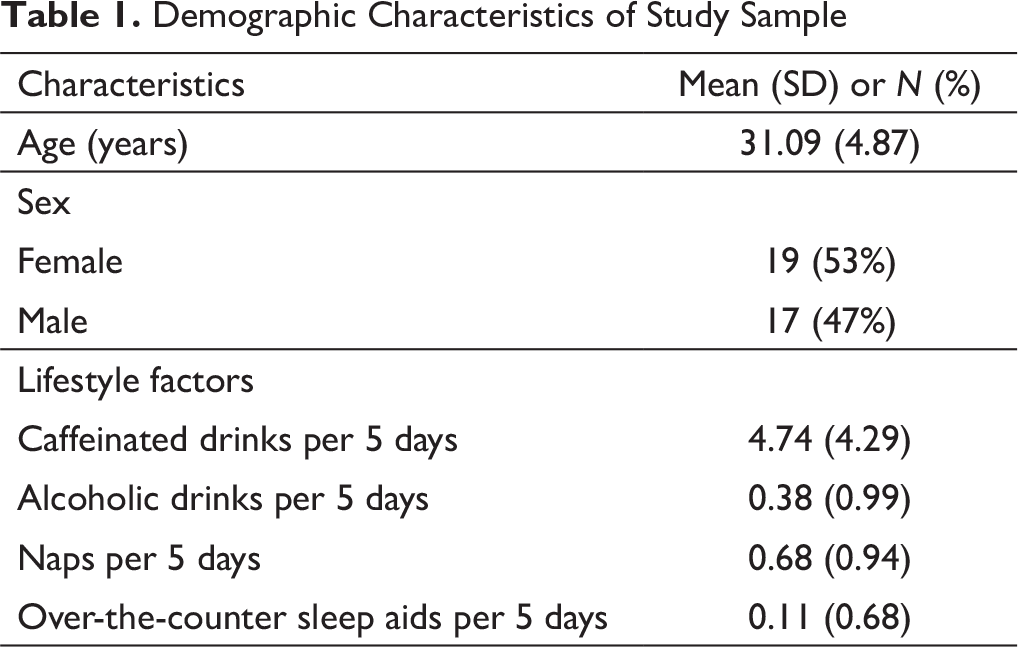
All 36 residents participated in the study (mean age 31.09 years, SD 4.87); 34 residents (94.4%) had complete pre–post data. Consensus sleep diary data showed decreased sleep onset time from 21.03 to 14.84 min (P = .01); sleep quality and restfulness scores increased from 3.32 to 3.89 and 3.08 to 3.54, respectively (P < .001 for both). Actigraphy showed a change in sleep onset time from 20.9 min to 14.5 min (P = .003). Sleep efficiency improved from 83.5% to 85.6% (P = .019). Wakefulness after initial sleep onset changed from 38.8 to 39.9 min (P = .682). Sleep fragmentation index and the number of awakenings decreased from 6.16 to 5.46 (P = .004) and 41.71 to 36.37 (P = .013), respectively.
Conclusions:
Residents obtained nearly 7 h of sleep during outpatient rotation. Findings suggest a structured Heartfulness meditation practice to be a feasible program to improve subjective sleep onset time and several objective measures among resident physicians.
Introduction
Sleep deprivation and the number of hours worked by a resident physician have been linked to significant medical errors, decreased well-being, poor cognitive performance, attention dysfunction, burnout, and decreased quality of care.1–4 There is growing consensus that inadequate sleep carries both short-term and long-term consequences. Acute sleep disturbances present dose-dependent deterioration in motor skills, mood, and cognitive abilities—equivalent to a blood alcohol concentration of 0.004% rise per hour, while chronic sleep problems generate depressed mood, attention, and cognitive impairments, which is typically seen after 6 h of sleep per night in less than two weeks. 5 Further, a clinical review provided evidence that sleep problems correlated with impeded learning, especially poorer declarative and procedural learning, neurocognitive performance, and academic success. 6 Beyond academic performance, sleep deprivation has been associated with alterations in brain functions and structure. Researchers have reported abnormalities in the hippocampus, amygdala, and insula7, 8 and have indicated convergent functional brain alterations in the inferior parietal cortex and superior parietal lobule. 9 White matter microstructure and cognitive performance may be influenced by sleep duration. 10 Healthy sleep is the foundation of wellness and is characterized by sufficient quality and duration, regularity, and the absence of sleep disturbances. 11
Duty hour regulations implemented by the Accreditation Council of Graduate Medical Education aimed to mitigate fatigue, improve sleep, and enhance wellness. However, the efficacy of these duty hour regulations is unclear.12, 13 As the quality of sleep of resident physicians plays an important role in their performance, it is imperative to explore the possible options to improve sleep. Implementing adaptive strategies to enhance sleep quality may help trainee physicians manage schedules that are often not conducive to natural sleep patterns. Early exposure to such strategies can potentially have a positive effect throughout their careers.
Heartfulness meditation involves meditation on the heart and has shown to improve burnout in physicians, advanced practice clinicians, and nurses.14, 15 The practice aims at achieving an inner state of balance within an individual. Heartfulness meditation practice was associated with a significant improvement in sleep in a study of patients with chronic insomnia. 16 However, the effect of this meditation on sleep has not been studied with actigraphy in resident physicians. In this study, we hypothesized that daily practice of Heartfulness meditation would result in improvement of sleep parameters and quality of sleep in residents.
Methods
Setting and Participants
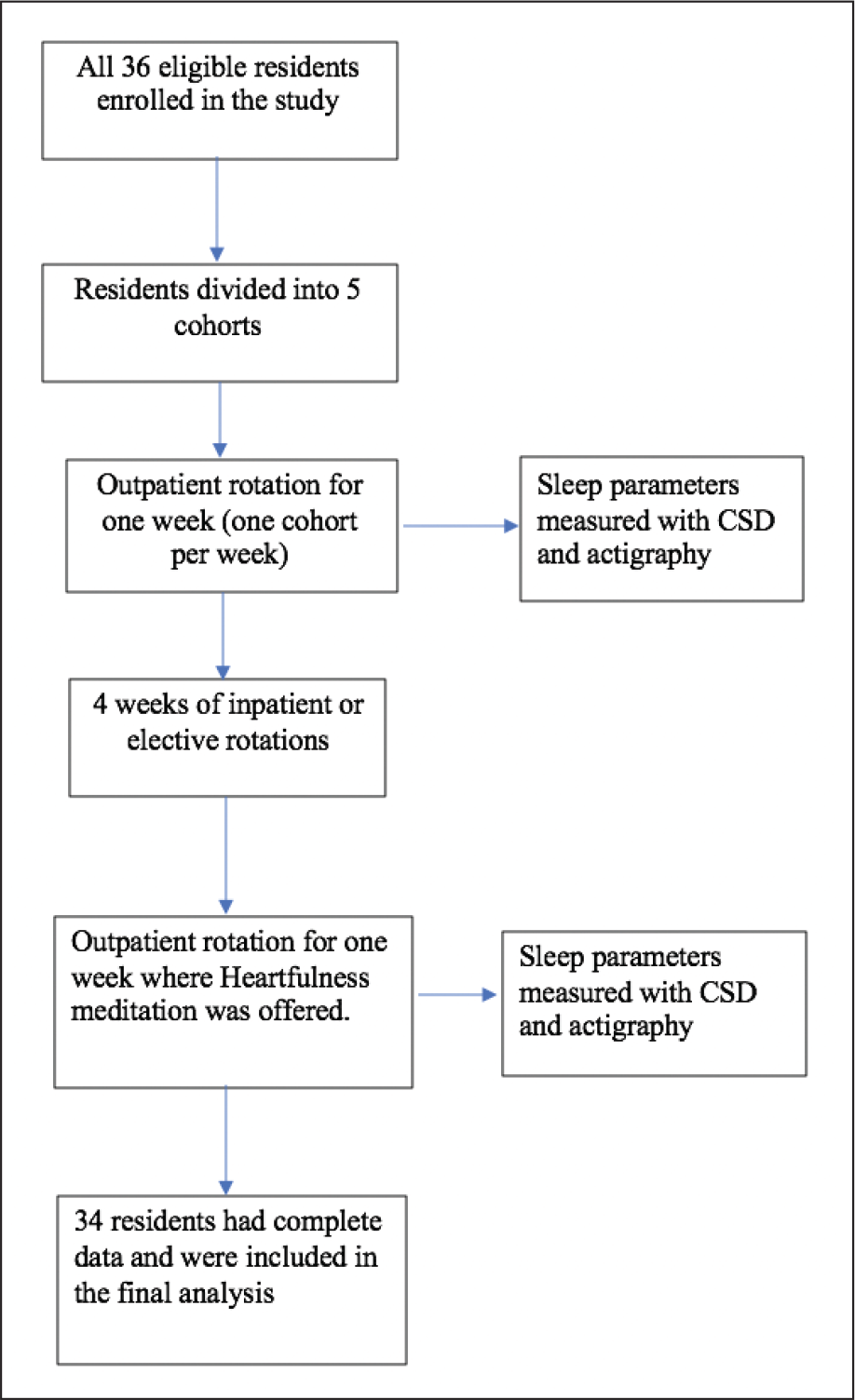
The study was a prospective cohort trial conducted from January 2019 through April 2019. The study included residents of an internal medicine residency program in a 596-bed teaching hospital in the US. Interest in participation was assessed via email along with a presentation about the study to the residents. Orientation about the protocol was offered to the participants prior to the start of the study. The baseline sleep parameters were measured during a one-week outpatient rotation. When the residents returned to their next one-week outpatient rotation after four intervening weeks, they participated in Heartfulness meditation and the sleep parameters were remeasured. All research participation was voluntary, following informed consent. A CONSORT flow chart outlines the enrollment of participants (Figure 1).
CONSORT Flow Chart.
Schedule
The residency program utilized a 4 + 1 scheduling format, which divided the program into five cohorts. Each cohort’s schedule was staggered by one week, with each cohort spending every fifth week in the ambulatory continuity clinic. The hours for this week were 8:00 AM to 5:00 PM, with no night responsibilities or calls. The four intervening weeks were spent on inpatient ward, intensive care unit (ICU), elective rotations, night float, and/or vacation. There was no 24-h call during these weeks.
Measures
Quantitative Assessment Tools
Two validated assessment tools, i.e., consensus sleep diary (CSD) and actigraphy, were used in the study. CSD is an outgrowth of the 2005 Insomnia Assessment Conference, and is a validated, self-reported measure of sleep that is tracked on a day-to-day basis. 17 CSD yields information on a number of relevant metrics including nightly sleep onset latency, wakefulness after initial sleep onset (WASO), total sleep time (TST), total time spent in bed, sleep efficiency (SE, i.e., the percent of the time asleep out of the amount of time spent in bed), and sleep quality or satisfaction, which reflects a subjective global appraisal of each night's sleep.17, 18 Actigraphy objectively measures sleep using a wristwatch-like device with a noninvasive sensor technology that records movement. Collected data are downloaded on a computer for display and analysis. These data are then processed by computer algorithms that use predetermined thresholds to label time as “sleep” or “wake.” 19 Actigraphy has been used to analyze sleep/wake patterns for more than 30 years and has been validated in multiple studies.20, 21 Thus, the two quantitative tools were deemed appropriate for the study.
Qualitative Assessment Tool
To assess the feasibility of the intervention, a single question open-ended qualitative feedback was collected through a survey at the end of study period. A physical folder was placed in the outpatient department for any anonymous, qualitative feedback on the intervention.
Intervention
On the first day of the week of the outpatient rotation, residents were provided with CSD questionnaires and actigraphy watches for baseline data. They were requested to fill out the questionnaire daily for the entire week of the study and were asked to wear the actigraphy watches on the nondominant hand for the entire week. The actigraphy watches were assessed for functionality by sleep office staff prior to the study. At the end of the week, the questionnaires and the watches were collected, and the data were subsequently downloaded. Five cohorts of residents went through the baseline assessments with seven to eight residents each week. As each cohort returned to the outpatient rotation after four intervening weeks, they were again provided with CSD questionnaires and actigraphy watches. All the participating residents in the study were given instructions on Heartfulness meditation, and daily guided relaxation and meditation sessions were conducted in the office for 20 min. In addition, participants were asked to listen to a Heartfulness relaxation audio prior to sleep. At the end of the week, CSD questionnaires and watches were collected again, and the data were downloaded. Each participant was able to provide anonymous feedback about the study and their experience. Data were collected for each resident for four nights during both the baseline and intervention weeks.
Heartfulness-Guided Practice
Participating residents were asked to sit comfortably with their eyes closed and instructions were given by the Heartfulness meditation trainer to progressively relax their body from their toes to their head. This was followed by instructions to gently focus their attention on the source of light within their heart. Participants were asked to simply tune into their hearts and be open to any experience they may have, as opposed to trying to visualize the light. If their attention drifted, the participants were advised to gently redirect their attention back to their heart. This practice was performed for 20 min in the office. The participants also listened to a Heartfulness relaxation audio of approximately 6-min duration while lying down on the bed prior to sleep.
Data Analysis
Outcomes of Interest
Primary outcomes measured included sleep parameters as assessed by the CSD and actigraphy during outpatient rotation. Specific parameters for the CSD included the mean sleep onset time, sleep fragmentation index (SFI), sleep quality, restfulness, number of awakenings per night, and total subjective sleep time. Specific parameters for the actigraphy included sleep onset time, SE, the number of awakenings, SFI, TST, and WASO. The effects of guided relaxation and meditation practices on these parameters were quantified. Secondary outcomes included assessing feasibility of the intervention through a qualitative feedback survey.
Analysis of the Outcomes
Quantitative data were summarized using frequencies and means. Changes in sleep scores and actigraphy scores were analyzed by paired t-test, and an α < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS v.24 (IBM, Armonk, NY, USA).
Qualitative data were subjected to thematic analysis. The themes were initially developed by the principal investigator based on the anonymous letters shared by participants and then checked for validity by one of the co-authors.
IRB Statement
The study was approved by the WellSpan York Hospital Institutional Review Board (IRB) prior to enrollment. The trial was registered within ISRCTN registry (ID ISRCTN16871934). Informed consent was obtained from all participants.
Results
Study Population
Demographic Characteristics of Study Sample
CSD Results
Consensus Sleep Diary Data
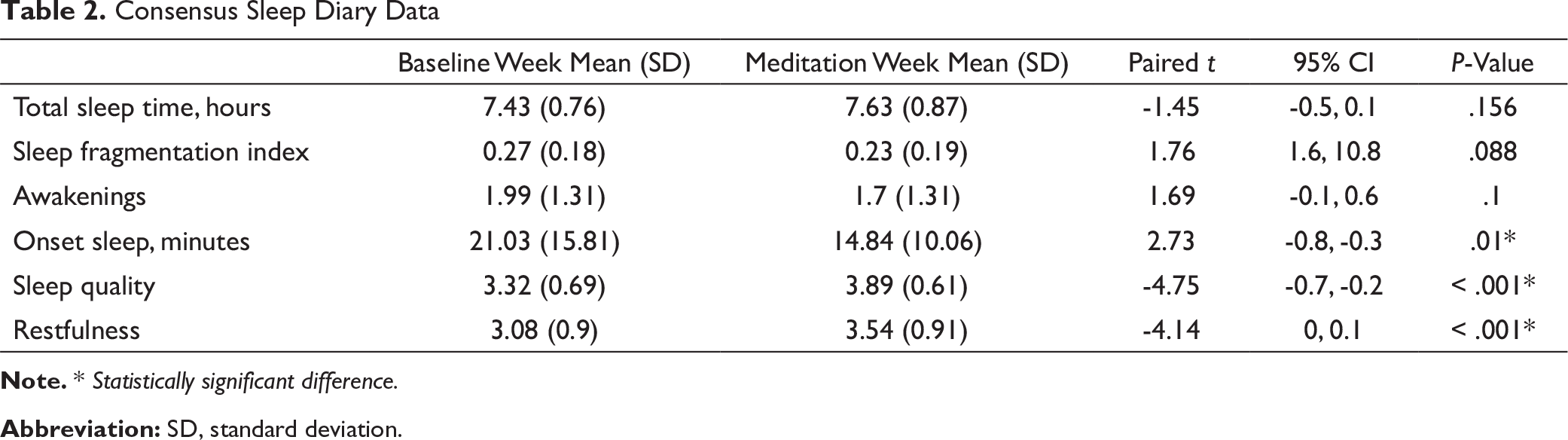
Note. * Statistically significant difference.
Abbreviation: SD, standard deviation.
Lifestyle Factors That Influence Sleep From the Consensus Sleep Diary

Note. * Statistically significant difference.
Abbreviation: SD, standard deviation.
Actigraphy Data
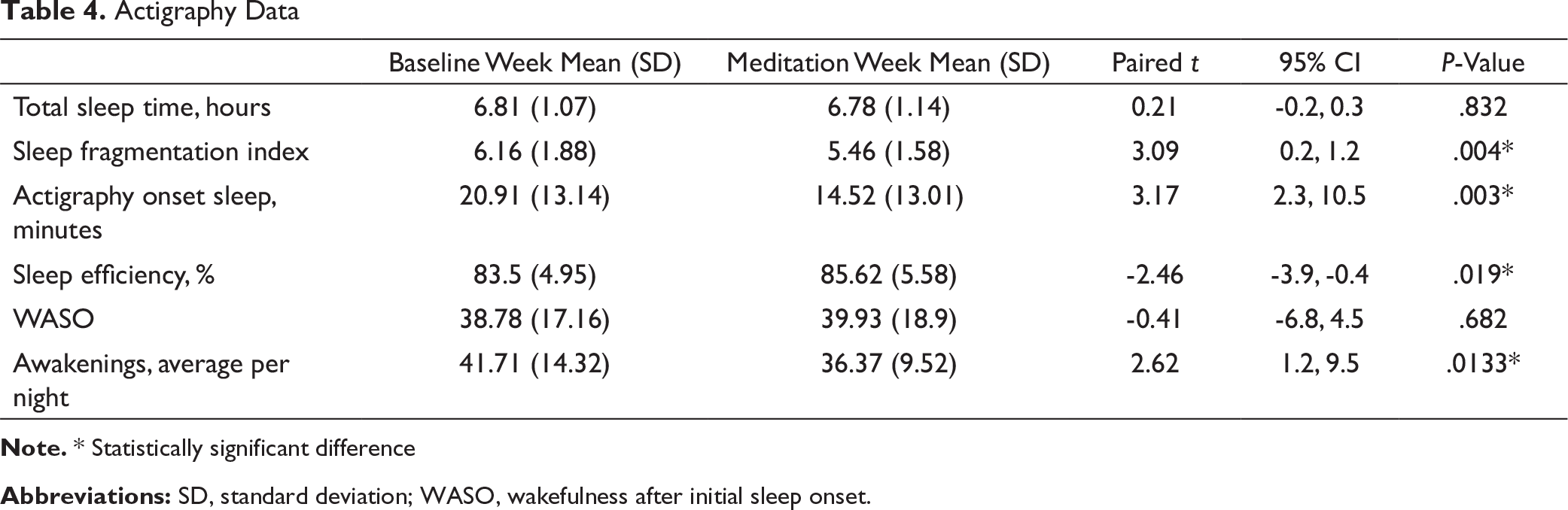
Note. * Statistically significant difference
Abbreviations: SD, standard deviation; WASO, wakefulness after initial sleep onset.
Actigraphy Results
Compared to the baseline week, the week of meditation showed a significant reduction in the sleep onset time from 20.9 to 14.5 min (95% CI [2.3, 10.5]; P = .003). SE improved from 83.5% to 85.6% (95% CI [-3.9, -0.4]; P = .019). The number of awakenings decreased from 41.71 to 36.37 (95% CI [1.2, 9.5]; P = .013). The SFI decreased from 6.16 to 5.46 (95% CI [0.2, 1.2]; P = .004). TST for the studied weeks remained at 6.8 and 6.78 h, respectively (95% CI [-0.2, 0.3]; P = .832). WASO changed from 38.8 to 39.9 min (95% CI [-6.8, 4.5]; P = .682). These results are reported in Table 4.
Compliance
The guided meditation sessions were attended by all the resident physicians (100%); 32 of the 34 residents (94%) listened to the relaxation audio daily at night. This was assessed through a subjective report at the end of the week.
Qualitative Analysis
All participants shared their experiences and future recommendations of the intervention at the end of the study period through an anonymous survey addressed to the principal investigator submitted through a physical folder in the outpatient office. Two major themes emerged from the analysis—first theme centered around experiences during meditation and second was related to the feasibility of the intervention.
The majority of participants expressed feeling light, calm, and relaxed during meditation. Meditation during afternoon and nighttime were equally favored. Notably, a number of participants also expressed interest in continuing meditation practices beyond the study period.
“I had a very positive experience with meditation and would continue to meditate during my more stressful rotations to get more benefit.”
“Dreams I had during the afternoon lecture were unique. Dreams of flying like an eagle, light and high. I have never had similar dreams in the past. Thanks a lot!”
“The meditation was really relaxing and with each session I felt refreshed. This is something to incorporate into daily activity.”
Several participants provided extensive feedback on the intervention and its outcomes. The reciprocal relationship between sleep disturbance, meditation, and daily functioning was reinforced by participants' observations of the benefits when their sleep improved. Residents reported feeling more productive during the day, improved efficiency in managing daily tasks and reducing stress, and reduced time in falling asleep. Further, there were also recommendations to include meditation especially during hospital floor rotations and ICU rotation which are typically long and intense hours for residents.
“Meditation was very helpful in calming the mind and helped me be more focused on the tasks at hand. It was good for the rejuvenation of the mind and body. The sessions were conducted very well. It might be helpful to include in our floor rotations, even ICU, if possible.”
“Really appreciated the meditation sessions as a way to take ‘a step back’ from a hectic week; this week was the most productive I have been during and outside work!”
“I think meditation should be incorporated into inpatient lectures at least three times a week. It helps relax and refresh the mind and would help reduce the stress of working in the hospital floor/ICU.”
Limitations of the intervention were identified. These included suggestions to conduct meditation in a quieter environment “Great sessions, length of time is perfect. Maybe a quieter environment or dim lights”; and clarity on study instrument “Only feedback would be understanding the need to wear the watches during the day and how it benefits the study.”
Discussion
The CSD data showed significant improvement in sleep onset time, sleep quality, and restfulness. Actigraphy data showed significant improvement in sleep onset time, SE, number of awakenings, and SFI. This study shows that during an outpatient rotation, the residents obtained close to 7 h of sleep, as recommended by the American Academy of Sleep Medicine. 11
Although the mean daily sleep time was similar to previously reported data,22–24 improvements in restfulness and sleep quality in the participating residents are the most clinically relevant findings from this study. The proposed intervention may have benefits for resident physicians in their clinical and training environments as well as for their overall health and wellness. Previous studies have demonstrated the importance of sleep in learning and memory consolidation, which are both important tasks for resident physicians. 25 Related, there were significant, cumulative dose-dependent deficits in cognitive performance and neurobehavioral functions with chronic restriction of sleep to 6 h or less per night. 26 Poor sleep has been implicated in insulin resistance and is a risk factor for the development of obesity and type II diabetes. 27 Additionally, insufficient sleep negatively affects blood pressure. 28 Motor vehicle accidents are more common with poor sleep as well. 29
Several other factors can affect sleep, such as consumption of caffeine, alcohol, number of naps, and use of sleep aids, including over-the-counter agents. For example, caffeine intake may disrupt both subjective and objective measures of sleep. 30 Alcohol use has been reported to be associated with sleep disturbances, including insomnia. 31 Likewise, frequent daytime napping has been associated with shorter nighttime sleep duration. 32 The effect of over-the-counter sleep aids is unknown. 33 Optimizing some of these factors, often included in sleep hygiene, is considered an important means of improving sleep. 34 While this has not been shown to improve sleep in a resident physician population, 23 it remains important to account for these variables. These elements are quantified in the CSD questionnaire. In this study, there was no difference in these factors during the baseline and intervention weeks, mitigating the effects of these variables on the findings. Prospective data collection, and a combination of subjective sleep diary reports and objective actigraphy data support the validity of the study. The study does show discrepancies between subjective and objective findings. For example, there is a discrepancy between the number of awakenings reported through CSD and actigraphy measurements. This is likely due to the sensitivity of movement detection by actigraphy, resulting in a substantially increased number of awakenings recorded through the watches. Further, the qualitative feedback questionnaire demonstrated favorable results in feasibility and acceptability of the intervention among resident physicians.
Prior studies have examined the benefits of offering similar meditation programs to improve resilience and general well-being during residency training. One research group conducted a 10-h mindfulness training workshop for resident physicians that focused on self-care, compassion practices, and patient relationships. They noted improvements in burnout, perceived stress, and level of mindful awareness, while having positive influences on residents’ personal lives and clinical practice. 35 Another study for family practice residents utilized the Respiratory One Method (a meditation practice combining breathing and repetition) for stress reduction, with results showing a positive effect on emotional exhaustion. 36 Similarly, in another study, pediatric residents utilized a smartphone application to complete a 10-d program in mindfulness meditation, and completed surveys at the end of the program. Results provided supportive evidence of meditation as a behavioral intervention to reduce anxiety and increase empathy among graduate healthcare students. 37 In all of these studies,35–37 burnout and stress were extensively studied with limited information on benefits of meditation to improve sleep among residents.
There are limitations to this study. The current study only assessed changes during the study period. Long-term effects have not been studied. As the study was performed on internal medicine residents during one outpatient rotation, it would be premature to generalize these results to residents on other rotations, including inpatient and night float rotations. Sleep disruptions and inconsistencies are more common during inpatient rotations with night calls than during outpatient rotations. 15 Additionally, the study was performed during the second half of the academic year; hence, it is uncertain whether similar results would be obtained during earlier portions of the year which are typically more intense than the latter half. Finally, as this study employed a pre–post cohort design, the lack of a control group limited the strength of the study.
Further research may explore whether these benefits of Heartfulness meditation can be replicated for residents on rotations that inherently pose more threats to the maintenance of normal sleep patterns (night float or ICU rotations, for example) and whether these benefits may then correlate with decrease in resident burnout.
Conclusion
Residents obtained close to 7 h of sleep during outpatient rotation as recommended by the American Academy of Sleep Medicine. Structured Heartfulness meditation practice improved subjective sleep onset time, sleep quality, and restfulness. Actigraphy data showed similar patterns of reduced sleep onset time, reduced awakenings, and improved SE. Findings suggest a structured Heartfulness meditation practice to be a feasible program to improve subjective sleep onset time and several objective measures among resident physicians.
Footnotes
Acknowledgements
The authors offer sincere gratitude to Kamlesh D Patel, PhD (Hon), President of Heartfulness Institute for guidance and advisory role on Heartfulness practices. The authors are grateful to Dr. Luminita Tudor for guidance with actigraphy data analysis, and Ms. Jennifer Gates from WellSpan Sleep office for actigraphy software support. The authors would like to thank Dr. Ronald Benenson, Ms. Kate Kelly, Dr. Sundeep Katepalli, Ms. Leah Eckert, Ms. Melissa Schlenker, and Dr. Jennifer Martin from WellSpan Health for their invaluable support for the study. The authors also thank Mr. Victor Kannan, Dr. Ranjani Iyer, and Mr. Balaji Iyer from Heartfulness Institute for their immense help for the development of the study protocol.
Ethical Statement
The study was approved by the WellSpan York Hospital Institutional Review Board (IRB) prior to enrollment. The trial was registered within ISRCTN registry (IDISRCTN16871934). Informed consent was obtained from all participants.
Declaration of Conflicting Interests
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was funded by an innovation grant from the Alliance for Academic Internal Medicine and a research support grant from Lake Erie College of Medicine.