
Abstract
Background
Hiccups is a known presentation of lateral medullary infarction. However, the region in the medulla associated with this finding is not clearly known. In this study, we aimed to study the neural correlates of hiccups in patients with lateral medullary infarction (LMI).
Methods
This retrospective study included all patients who presented with lateral medullary infarction between January 2008 and May 2018. Patients with hiccups following LMI were identified as cases and those with no hiccups but who had LMI were taken as controls. The magnetic resonance imaging of the brain was done viewed and individual lesions were mapped manually to the template brain. Voxel-based lesion-symptom mapping employing nonparametric permutation testing was performed using MRIcron.
Results
There were a total of 31 patients with LMI who presented to the hospital during the study period. There were 11 (35.5%) patients with hiccups. Using the voxel-based lesion-symptom mapping analysis, the dorso-lateral region of the middle medulla showed significant association with hiccups.
Conclusion
In patients with LMI, we postulate that damage to the dorsolateral aspect on the middle medulla could result in hiccups.
Keywords
Introduction
Hiccups is an involuntary inspiration against a closed glottis. Hiccups is also known as singultus, which in Latin refers to the sharp intake of breath that occurs while crying. 1 Hiccups occur because of many causes which can be broadly divided into central and peripheral causes. Among these, lateral medullary infarction (LMI) is one of the central causes for hiccups. Intractable hiccups which can occur in LMI may lead to aspiration pneumonia, oesophagitis, exhaustion, malnutrition, dehydration, and in severe cases, respiratory depression and death. 1 2 Previous lesion-based studies have shown that the dorsolateral region of the lateral medulla is associated with hiccups. 3 4 In this study, we aimed to identify the neural correlates of hiccups in patients with LMI, by using voxel-based lesion-symptom (VLSM) mapping. 5
Methods
Subjects
This retrospective study was done in the neurology department of Christian Medical College, Vellore in South India. The study was approved by the Institutional Review Board and ethics committee. All consecutive patients admitted under neurology with a diagnosis of lateral medullary infarction between January 2008 and May 2018 were identified by searching the inpatient records using a computerized database. Details of history and neurological examination findings of all patients were recorded on a standard data collection sheet. The following characteristics were extracted: demographics, clinical features, comorbidities, and duration of hospital stay. Patients with hiccups caused by an acute lateral medullary infarction were taken as cases. Exclusion criteria included (a) nonavailability of neuro-imaging and (b) poor image resolution because of which lesion boundaries could not be delineated. Controls included those patients with LMI but no hiccups.
Lesion Mapping
All patients had a brain magnetic resonance imaging (MRI) scan within seven days from the time of admission to hospital (Siemens 3T Skyra scanner, Siemens, Erlanger, Germany). MRI images were reviewed by a neurologist trained in lesion mapping and diffusion-weighted imaging and T2- weighted and fluid-attenuated inversion recovery sequences were used for lesion mapping. The individual lesions were mapped onto the Montreal Neurological Institute (MNI) space manually using MRIcron (
Data Availability
Data can be made available on request.
Results
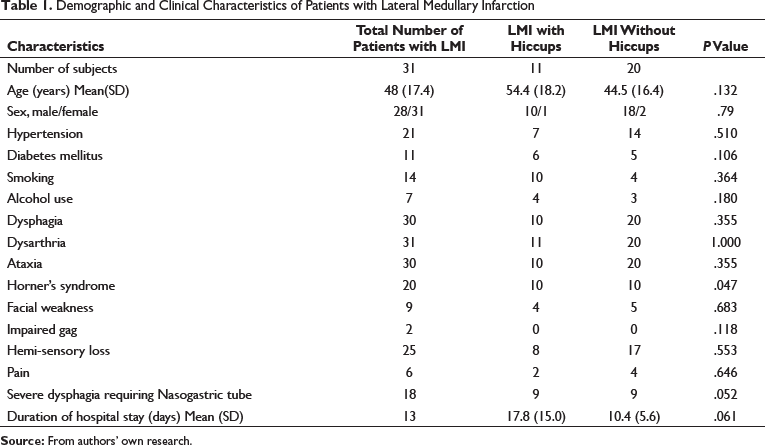
Demographic and Clinical Characteristics of Patients with Lateral Medullary Infarction
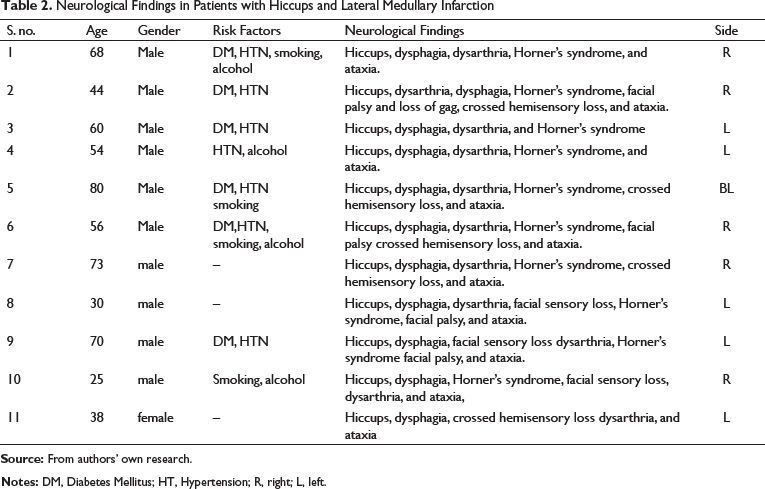
Neurological Findings in Patients with Hiccups and Lateral Medullary Infarction
Results of the Voxel-Based Lesion-Symptoms Analysis
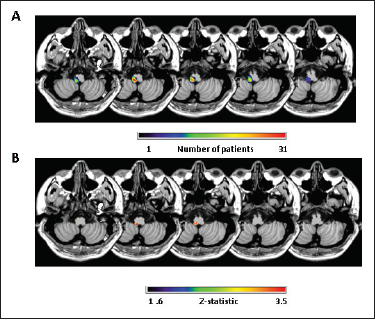
Location of the lesions in 31 patients is given as a lesion overlay map in Figure 1A. This includes 11 cases and 20 controls. The lesions were distributed across the caudal, middle, and rostral medulla. The results of the VLSM analysis are shown as a statistical map in Figure 1B. The color scale denotes the z-scores from the Liebermeister test that shows the association of a given voxel to hiccups at a false discovery rate level of 5%. The MNI coordinates for the area maximally associated with hiccups was (x = –4, y = –40, z = –58). This region was located at the dorsolateral region of the middle medulla.
Discussion
The hiccup reflex is characterized by sudden inspiration immediately followed by an active closure of the glottis. 1 The reflex arc for hiccups involves phrenic, glossopharyngeal, vagal, and sympathetic pathways as afferents, a central pattern generator in the lower brainstem, and motor neurons that supply the diaphragm and the other respiratory muscles as the efferent. 10 11 12 The neurotransmitters involved in hiccups include gamma-aminobutyric acid (GABA), dopamine, and serotonin, and hence, blocking these has proved to be useful in the treatment of hiccups. 12 13 There are central and peripheral causes for hiccups. Cerebrovascular accidents, trauma, and space occupying lesions include some of the central causes, and peripheral causes include gastro-esophageal reflux, lesions along the afferent pathway such as tumors, herpes infection or myocardial ischemia and drugs like steroids, anti-Parkinsonism and chemotherapeutic agents. 1 Medullary lesions are known to result in hiccups, and lateral medullary infarction is an important cause for intractable hiccups. 14 15
The function of hiccups continues to remain poorly understood. 1 12 Phylogenetically, hiccups are similar to the gill ventilation that occurs in fish and tadpoles. In tadpoles, gill ventilation precedes lung ventilation which is similar to that of humans where, embryologically, hiccups occur during the latter part of gestation, even before the onset of fetal respiration. 16 It is postulated that hiccups may be the expression of archaic motor patterns of gill ventilation which may persist in mammals for other useful functions of the pharynx and chest wall muscles, such as suckling or eupneic breathing. 16 17 There are numerous other theories on the pathophysiology of hiccups. One of the important theories suggests that hiccups are caused by the failure of the reciprocal inhibition of the valve control of the pharynx and larynx. 18 This dynamic valve function is achieved by alternating excitation-inhibition of two structures: The glottis closure complex and the inspiratory complex. 18 Imbalance between inspiration and expiration as because of destruction of the expiratory center and destruction of the dorsal motor nucleus of vagus and nucleus ambiguus which innervate the diaphragm are other postulated mechanisms. 17 18
Neuroanatomical correlates on the sites that produce hiccups have been studied widely in animals and in few limited human studies. 4 10 14 Studies done in cats have shown that the area associated with hiccups is in the solitary tract nucleus in the dorsal medulla and the reticular formation reticular formation lateral to the nucleus ambiguus, at the rostrocaudal level between 1.0 mm and 2.5 mm rostral to the obex. 10 13 In a lesion-based study in patients with LMI, Park et al. found that the dorsolateral region of the middle lateral medulla was involved in patients with hiccups. 3 Another study done by Moon et al. in 2014 showed that in patients with LMI, those that had hiccups often had dorsal rather than ventral lesions.
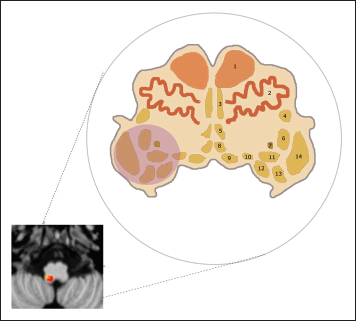
In our study on patients with LMI, using the method of VLSM, we demonstrated that the area associated with hiccups was on the dorsolateral aspect of the middle medulla. Based on this location we postulate that the involvement of nucleus of solitary tract, nucleus ambiguus, associated reticular formation, fifth cranial nerve nuclei, and their connections with the middle part of the medulla are necessary for the development of hiccups (Figure 2). The MNI coordinates for the area maximally associated with hiccups was at (x = –4, y = –40, z = –58) which is 2 mm above the obex. Our results corroborate with the findings of Park et al. and Moon et al.,3,4 who demonstrated the involvement of the dorsolateral middle medulla. Also, the medullary reticular formation lateral to the nucleus ambiguus, which was found to be the generator of hiccups in cat stimulation studies, lies within the region identified by our study. 10 The association of hiccups with clinical findings of severe dysphagia and Horner’s syndrome suggests the anatomical proximity of the pattern generator of hiccups to the location of the nucleus of solitary tract and sympathetic tract. 3 19 The major strength of our study is that it is a lesion-symptom mapping study powered with statistical testing, unlike previous lesion-based studies on LMI and hiccups. The limitations of our study were the retrospective study design and the small sample size. The major strength of our study is that it is a lesion-based study powered with statistical testing, unlike previous on hiccups and LMI.
Conclusion
In patients presenting with LMI, we postulate that damage to the dorsolateral aspect on the middle medulla could result in hiccups.
Footnotes
Statement of Ethics
The study was approved by the Ethics committee and IRB of CMC Vellore, Tamil Nadu, India.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Department of Neurological Sciences, CMC Vellore, Tamil Nadu, India.