
Abstract
Background:
Diabetes is a metabolic disorder characterized by chronic hyperglycemia. Its prevention and regulation depends on dietary pattern and lifestyle. There are numerous studies which have been conducted to elucidate the relationship between type of diet consumption and sugar levels. The objective of this study was to enumerate the distribution of the staple food consumed in seven zones across India and their association with sugar levels.
Methods:
A pan-India multicentered screening, covering the 63 districts, 29 states, and 4 union territories per populations, was undertaken. A specially designed questionnaire was administered for data collection, which comprised specific questions for diet 17,280 sample was analyzed across seven zones of India. Statistical Package for the Social Sciences (SPSS; 21.0) software was used to analyze the data.
Results:
The survey suggested that rice and wheat are the major staple food consumed across different regions of India. In Jammu, North, East, South, and central zones, consumption of rice was more than wheat. However, in North and West zones, consumption of wheat was observed to be more than rice. Mean values of fasting blood sugar (FBS), postprandial blood sugar (PPBS) were high in the group consuming Bajra (128.3 & 160.5). Similarly, FBS mean was less in group consuming rice (114.6), and PPBS was low in group consuming ragi (149.2).
Conclusion:
Staple food has significant effect on FBS, PPBS and glycated haemoglobin cholesterol levels and anthropometric measurements.
Introduction
Diabetes is a metabolic and a lifestyle associated disease mainly characterized by the presence of high glucose levels detected in the blood stream. It is progressive in nature with serious consequences if not controlled and is essentially a life-style disease. Ayurveda proclaims that sedentary lifestyle and a sub-optimal dietary pattern are the most important preventable risk factors for the development of diabetes. Furthermore, the nature of staple food which diabetic subjects consume plays a key role in maintaining sugar levels. Worldwide, the prevalence of diabetes has been estimated to reach 150 million and is expected to be doubled by 2025. The rising prevalence in developing countries is closely connected with population structure, age structure and urbanization-change in lifestyle. 1 Its preponderance is high in India as well with largest number of subjects reported in 2003 (approximately 33 million) and is expected to cross 57.2 million by the year 2025. 2
Chronic hyperglycaemia (i.e., elevated levels of plasma glucose) is the result of perturbation occurring in carbohydrate, fat, and protein metabolism. 3 The primary driver of the epidemic of diabetes is the rapid changes in dietary patterns and decreased physical activity. 4
Furthermore, accumulating evidence indicates that there is an imbalance caused in gut microbiome which may enhance progression of Type 2 diabetes that occurs in about 90% of all diabetic cases worldwide. The imbalance caused in gut microbiome results in the release of toxic metabolites which subsequently affects the metabolic and signaling pathways of the host organism, and also influences the functions of the intestinal barrier. This is linked to insulin resistance directly or indirectly in diabetic subjects. 5
Ayurveda principles are based on the assumption that a living being is constituted by five elements of nature including water, earth, air, fire, and space, and there are three types of energy present in all living things known as pitta, vata, and kapha. According to ayurvedic principles, there is a disturbance in the balance of kapha energy in diabetic subjects. Kapha energy which is made up of elements earth and water gets imbalanced in diabetic people. Ayurveda texts emphasize more on association between lifestyle and manifestation of the disease. It explains daily and seasonal regime as a part of life-style management for prevention from the diseases. Furthermore, it gives importance to diet as a major cause for the vitiations of doshas and thus for manifestation of a disease. It accentuates following ways for prevention from the disease: hitabhuk (eating food which gives comfort), mitabhuk (eating less) and in treatment modality. Ayurveda explains nidana parivarjana (abstaining from the causative factor) is a crucial factor in the management of disease.
Ayurveda classics broadly categorize diabetes under the heading of prameha into 20 types. It falls under three major types under three doshas. Kaphaja varieties—10, Pittaga varieties—6, Vataja varieties—4. But main dosha involved in the manifestation of Prameha (diabetes) is Kapha dosha.
Diabetes mellitus can be considered as ikshubalika rasa meha of kaphaja type. Chronic stage of Type 2 diabetes can be correlated to madhumeha, a vataja type. Charaka et al. emphasized that improper dietary habits, disturbed metabolism, and reduced physical activity may attribute to the development of diabetes mellitus. Ayurveda suggests consumption of green leafy vegetables, wheat, barley, corn and oats for people suffering with diabetes which helps to balance Kapha dosha. Diabetic people must abstain themselves from consuming excessive sweets, sugars, seafood, and dairy products which are all considered to provoke the kapha energy.
Sushruta et al. suggested day time sleeping, lack of exercise, and laziness, along with consumption of sweet, oily, alcoholic foods, and beverages as the causative factors for development of diabetes later in life. Furthermore, Charaka et al. argued that excess of newly harvested food grains, jaggery preparations and factors responsible for elevation of kapha, may contribute to the development of diabetes.6, 7
Ayurveda also explains many varieties of staple foods and their relationship with tridosha. For instance, it is explained that rice increases vata and pitta; and wheat increases kapha, as it exhibits the quality of cold and oiliness. Ragi is considered as a trina dhanya, and it is explained that it reduces the kapha and pitta as it tastes like astringent. Jowar helps in reducing pitta and kapha, as it manifests the quality of coldness and astringent.6–9
Study on dietary habits and diabetes had been conducted and it was found that white rice consumption is associated with increased risk of Type 2 diabetes. 10 Comparative studies of white rice and brown rice have revealed that pregerminated brown rice is useful to control blood glucose level. 11 Consistent with this, a prospective study performed on Japanese women have established white rice consumption increases the risk of diabetes. 12 Furthermore, a meta-analysis of risk of diabetes in vegetarian and nonvegetarian diet had been conducted and its results revealed that the vegetarian people have reduced risk of diabetes as compared to nonvegetarian people. 13 Furthermore, there is no relation observed between fructose and sugar levels. 14
Another interesting study demonstrated that glycemic response of consuming rice with chopstick was lower than with spoon. The glycemic index (GI) of rice using chopsticks (GI: 68) was lower compared to using spoon (GI: 81). The present study suggests that eating rice with different feeding tools has different chewing times and amount of food taken per mouthful alters the GI of the rice. 15 Moreover, food with high GI (rice) may increase the risk of diabetes. 16 Another study has discussed the principal component analysis for nutrition factor with diabetes. 17
Relationship between dietary pattern and risk of diabetes has also been discussed. 18 Contrary to these reports, an investigation conducted on the Chinese population revealed that high rice consumption was not associated with diabetes risk. 19 Reduced effect of germination and amylose content of rice on the development of obesity and insulin resistance have been implicated. 20
Methods
Study Design
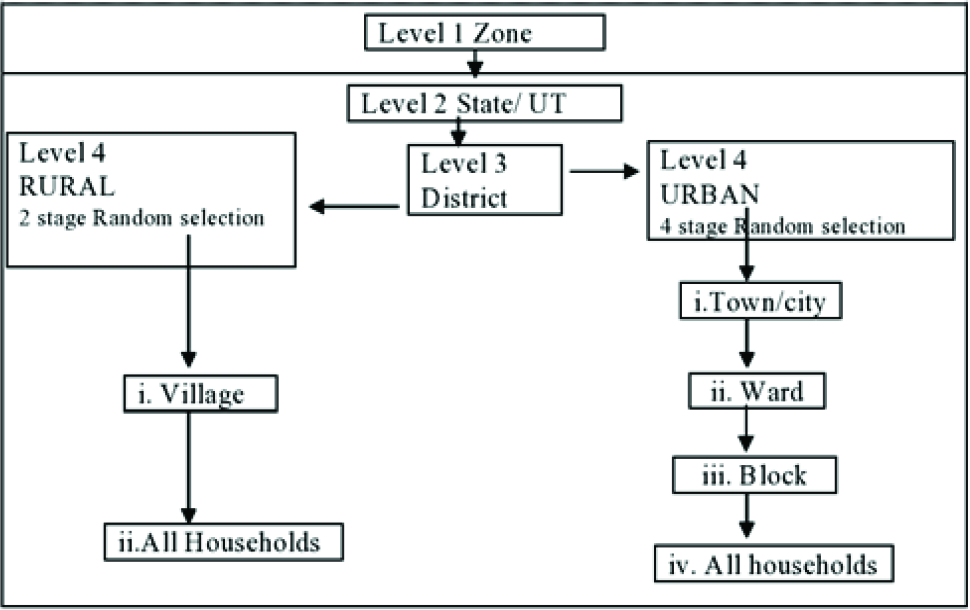
We confirm that all methods were carried out in accordance with relevant guidelines and regulations. Furthermore, we confirm that informed consent was obtained from all subjects and all experimental protocols were approved by the Institutional ethical committee (RES/IEC-IYA-001). Study included two phases. Phase I: rapid national sampling survey for estimating the present prevalence of known diabetics and new diabetics from unknown diabetics. Phase 2: fasting blood sugar (FBS), postprandial blood sugar (PPBS), and glycated haemoglobin (HbA1c) blood tests were conducted for people who had attained high risk Indian diabetes risk score (IDRS) tab. The number of people from whom data was available after curation was 17,280. Goal of the study was to check the association between diabetes and staple diet. In phase I, samples from seven geographical zones—Jammu & Kashmir, North-East, North, West, Central, East, and South were included. A stratified, multistage cluster sampling design was adopted: In rural areas, a two-stage village household design; and, in urban areas, a four-stage town/city-ward-block household design was adopted. Both rural and urban areas were stratified at three levels based on geographical distribution and population size (Figure 1).21
Stratification of Rural and Urban Areas at Three Levels Based on Geographical Distribution and Population Size
Individuals of both sex of age group range 20–80 and having IDRS score > 60 were included in the study, Individuals with severe complications and having IDRS score < 60 were excluded from the study.
Amongst 17,280 who were included for the present study, 3,626 people were self-reported Diabetes patients and 20% people were under medication.
Screening assessments for all participants included sociodemographic variables (education of the head, occupation of the head, family income) and clinical measures.
Clinical measures included: Height, weight, and waist circumference. Blood pressure, diabetes level (if previously diagnosed), and yoga awareness. All completed IDRS questionnaires. Further assessments for known diabetics and high and moderate risk according to IDRS HbA1c, fasting blood glucose; 2-hour post prandial glucose; and lipid profile (in venous blood).
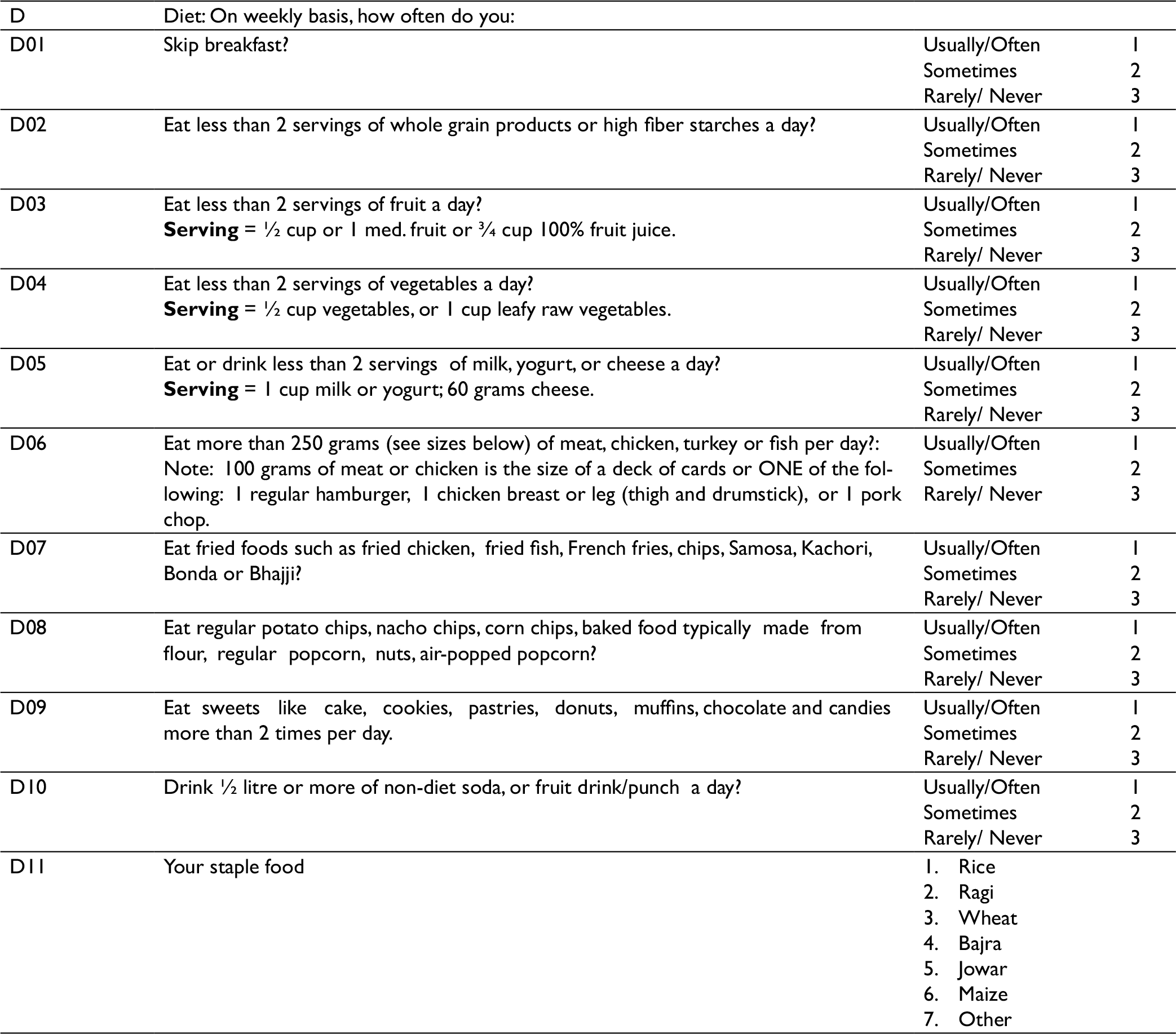
Factors of Questionnaire
The questionnaire contained detailed question about their food habits and major staple (cereal) food (Appendix).
Statistical Analysis
Data was uploaded via mobile apps by trained YVDMs (Yoga Volunteers for Diabetes Mellitus) under supervision of senior research fellows. Uploaded data from screening forms (about 4 < 0.001/district), registration forms, and laboratory data (about 50, < 0.001) were checked for perfect matching of coding. After cleaning on Excel, the data set was analyzed using R software for bio-statistical analyses. Cross tables was done to check the distribution of staple food. Linear regression was applied to check the association between sugar levels and staple food.
Results
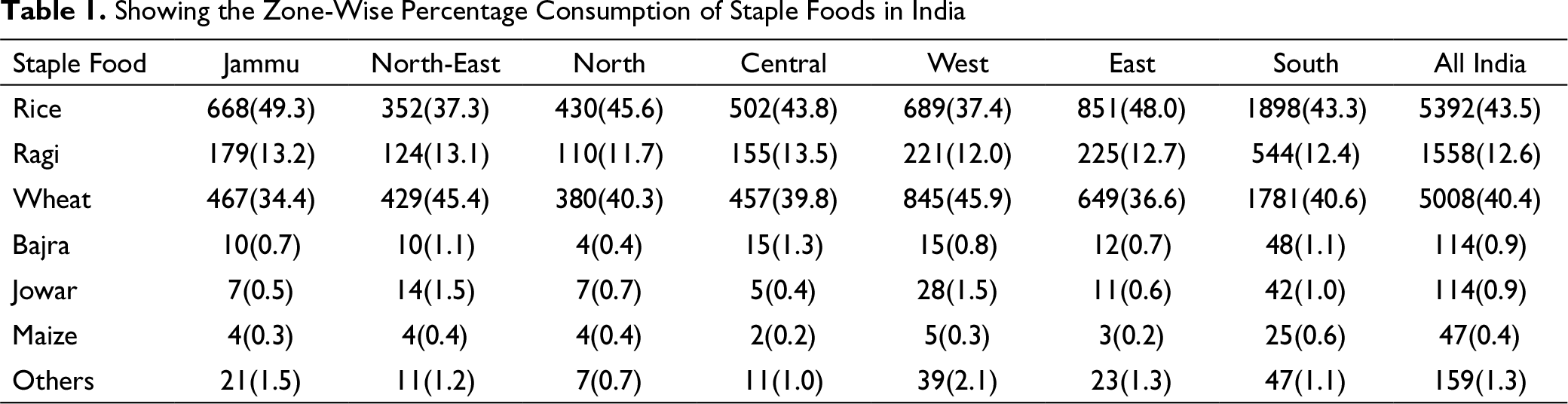
Table 1 shows the percentage consumption of various staple foods in various selected zones of India. As seen in the table, rice, wheat, and ragi are the major staple foods across India and are consumed by 95% of the population in all the selected seven zones; whereas bajra, jowar, maize, and other staple foods are consumed by negligible population in all the seven selected zones of India.
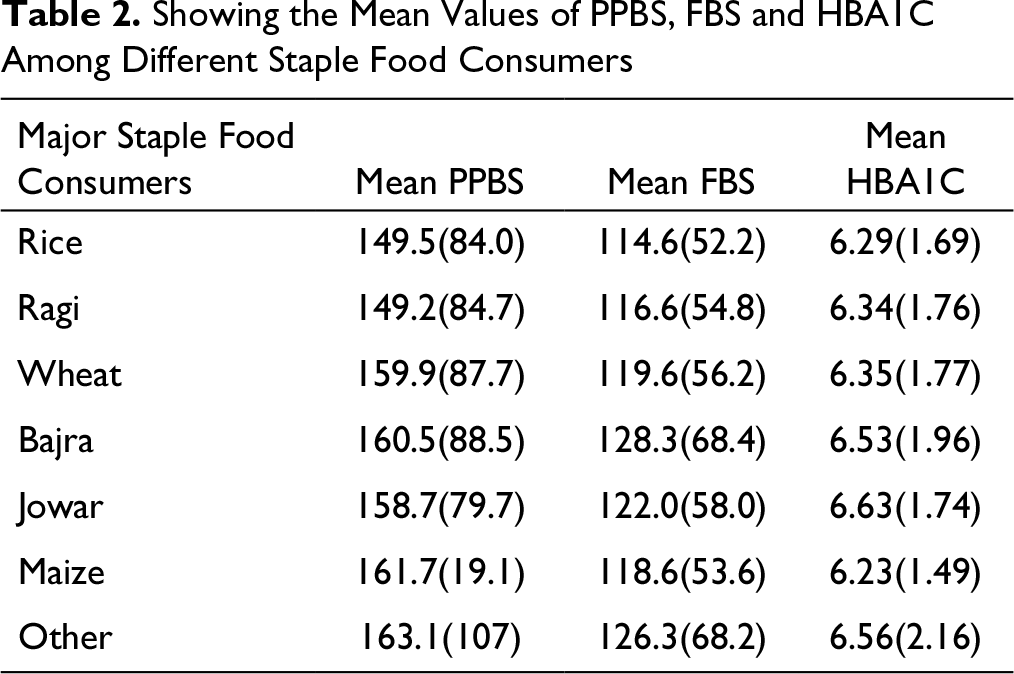
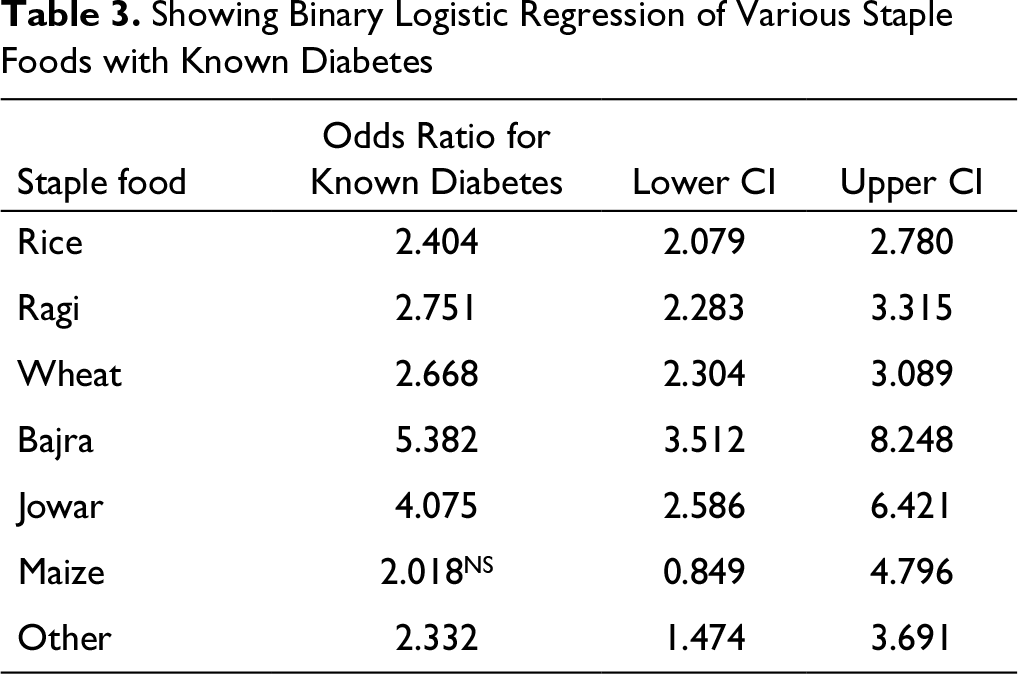
Table 2 shows the mean values of FBS, PPBS and HbA1c among selected sample (High IDRS > 60) with respective staple food consumption. The table shows that an increase of mean PPBS from mean FBS was highest among maize consumers, whereas the increase was lowest among bajra consumers. Moreover, this rise in value of mean PPBS from mean FBS was higher among wheat consumers as compared to rice consumers. Table 3 reveals the binary logistic regression of various staple foods with known diabetes. As seen in the table, the odds ratios were significant for all staple foods, except in case of staple food maize. The people consuming rice, ragi, and wheat were less prone to the status of known diabetes. The people consuming bajra and jowar were more prone to the status of known diabetes.
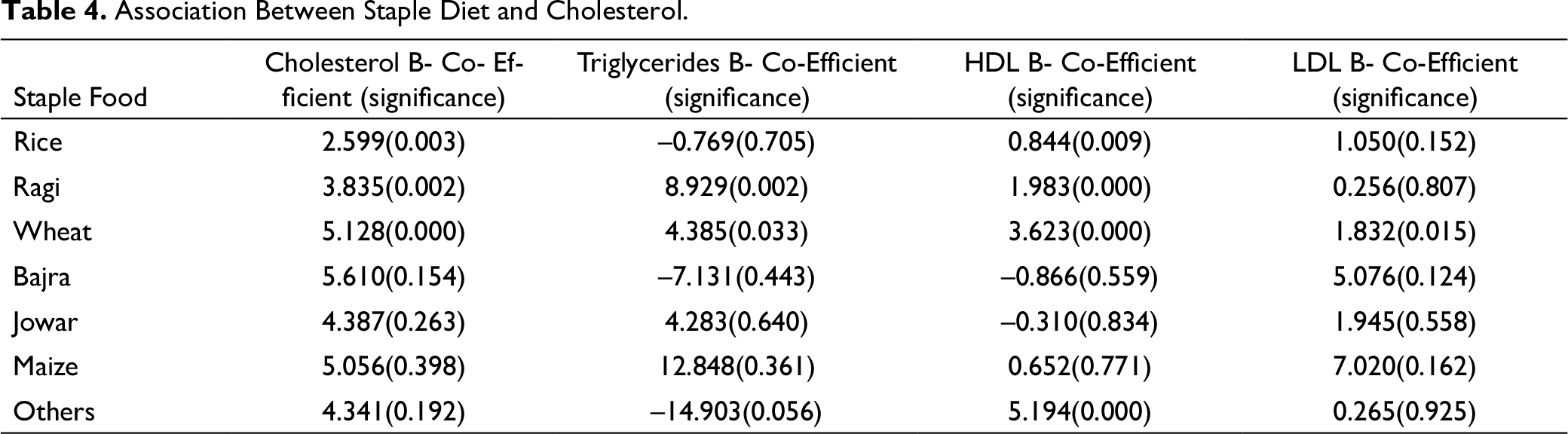
Table 4 gives the B values of the association of each staple food with cholesterol levels of an individual with significance values. Wheat is highly significantly associated with cholesterol, LDL (Low Density Lipoprotein) and HDL (High Density Lipoprotein) when compared to rice and ragi. Ragi is highly, positively and significantly associated with triglycerides when compared to rice and wheat. Bajra is positively associated with cholesterol and LDL, negatively associated with triglycerides and HDL but not significant. Jowar is positively associated with cholesterol, triglycerides, and LDL and negatively associated with HDL, but not significant; maize was highly positively associated with total cholesterol, triglycerides, LDL but not significant.
Showing the Zone-Wise Percentage Consumption of Staple Foods in India
Showing the Mean Values of PPBS, FBS and HBA1C Among Different Staple Food Consumers
Showing Binary Logistic Regression of Various Staple Foods with Known Diabetes
Association Between Staple Diet and Cholesterol.
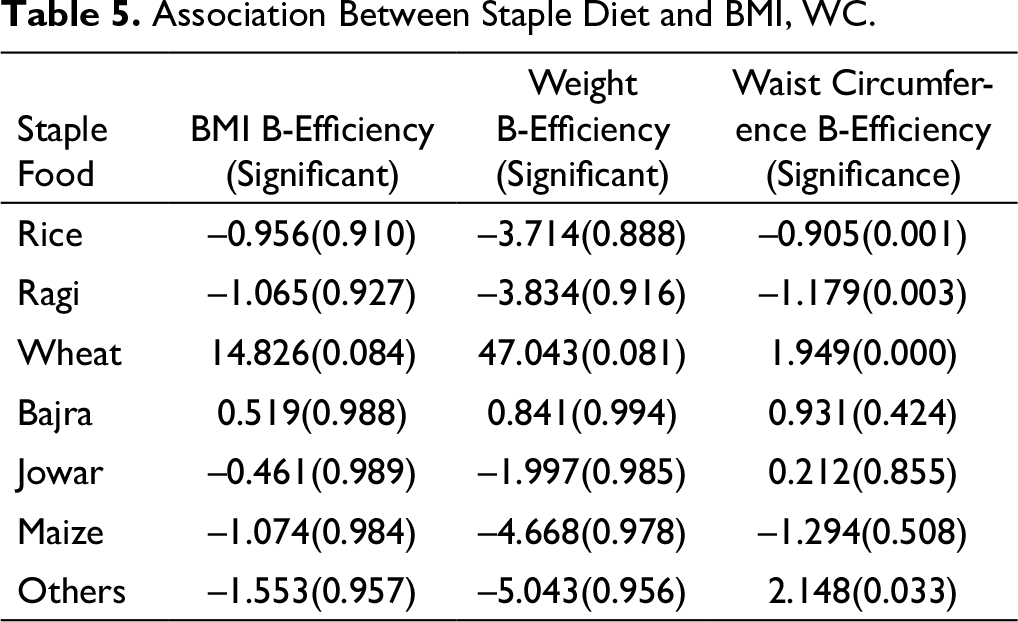
Association Between Staple Diet and BMI, WC.
Discussion
This was a study across rural urban areas of different zones of India to study the association between the major cereals in the diet with the glycemic status in diabetes.
The findings of the present study revealed that the consumption of rice, wheat, and ragi is more across India as compared to bajra, maize, jowar (coarse cereals), and other staple foods. It has been reported that consumption of these coarse cereals has intensely declined in both rural and urban population of India. This abrupt change in the food habit of Indians has led to deficiency of iron among them as these cereals are comparatively rich in iron content. Similarly, intake of ragi is more in rural area relatively, whereas consumption of wheat is more in urban area (Table 1).
Another finding of this study revealed that the rise in value of mean PPBS from mean FBS was higher among wheat consumers as compared to rice consumers, and the mean HbA1c was higher than the normal value among all consumers, indicating them to be prediabetic or diabetic (Table 2). This suggests that wheat which possesses high GI increases HbAc1 levels and should not be consumed much. Ziaee et al. studied the effect of a high fat low-glycemic load diet on HbA1c of poorly controlled diabetic patients. 22 In that study, the investigators recruited hundred diabetic patients, and administered them with a low-glycemic load diet for a period of two and a half months. Their data showed a positive correlation with HbA1c concentration and FBS after intake of high fat low-glycemic load diet. 23 The results of present study are contradictory to this study which indicates that diets with low GI are not good to control HbA1c levels and sugar levels of diabetic patients. It is noteworthy to mention that whole processed wheat bearing low GI as compared to unprocessed refined wheat are reported to keep sugar levels in control (Table 3).
In order to maintain regulated blood sugar and HbA1c levels in diabetic subjects, there are certain recommended diets that are to be followed. Various health organizations advise diets rich in 50%–60% carbohydrate, 15%–20% proteins and 20%–30% fats are good enough to keep diabetes under control. Diabetic people and people suffering with other related metabolic complications must consume diets with this composition to maintain a healthy lifestyle.24, 25 Additionally, intake of fiber is reported to produce a marked influence on glycemic control, 26 and large amounts of fiber should be consumed to control glycemic index. Previous literature suggests that 25 g of fiber intake per meal reduces PPBS level by 10%. 27
Su-Que et al. assessed the effect of nutrient-rich wheat bread Jizi439 and buckwheat on postprandial plasma levels in Type 2 diabetic subjects. Their findings revealed that intake of Jizi439 steamed bread resulted in reduced plasma glucose in both diabetic subjects and healthy people, compared with other types of test foods, suggesting that Jizi439 steamed bread is helpful in lowering the glycemic index. 28 In addition, people are less likely to develop Type 2 diabetes and/or other major diseases like cardiovascular diseases (CVDs) and cancer who consume whole grains compared to refined grains as whole grains contains all the vital nutrients which are lost during refining process.29, 30
Moreover, several studies have shown that increased intake of whole wheat grain changes the gut microbiota which assists in ameliorating the health of the individual. However, the association between the two is poorly understood.31-34 Findings of Borneo et al. demonstrated that total cholesterol and LDL cholesterol at fasting reduced when whole grain was consumed, whereas no significant changes were found in the refined grain group. Furthermore, there are overall health benefits and an amelioration of lipid profile observed when whole grains are consumed as compared to refined grains. 35 Whole wheat are thought to contain more fiber than refined grains hence they are able to decrease the blood cholesterol levels.36, 37 But our study showed that it is positively associated with cholesterol, tends to increase the cholesterol.
Cano et al. revealed maize-based diets have amazing health benefits and are helpful in reducing LDL levels in rats. 38 Studies have revealed that when whole wheat is consumed at a dosage of 48 g per day, then it has the potential to curtail total cholesterol in humans.39, 40 However, there are few contradictory reports which suggest that consumption of whole wheat does not influence blood cholesterol levels in some cases. 30 Similar findings were obtained by Odes et al., whose group found that intake of supplement with 12.5 g of fiber daily for two or four weeks had negligible effect on blood cholesterol levels in humans. 41 However, their findings also demonstrated that the lipid levels reduced when a combination of whole wheat, corn and rice was consumed for a period of six weeks. But our study showed that wheat and maize are positively associated with cholesterol and tend to increase the cholesterol.
These results demonstrate the role of kind of diet an individual consumes in health and disease. Ayurveda explains mainly two types of food: laghu and guru. Laghu means one which gets digested within three hours of consumption (example—rice, ragi) and Guru means the food which takes longer duration to get digested (example—wheat, black gram). Laghu type of food increases vata and decreases kapha. Guru type of food increases kapha and decreases vata. According to ayurveda, diabetes, cholesterol levels and obesity are caused by the vitiation of kapha dosha. Therefore, refined wheat is contraindicated in diabetes and obesity, whereas rice, ragi, and jowar are recommended for diabetes and obesity.
Ayurveda also suggests that newly cultivated rice is not good for diabetes, as it increases kapha. Instead, one should consume stocked old rice in diabetes and obesity. Usually, glycaemic index is considered for prescribing diet module for diabetes. GI of rice and ragi are 81 and 71, respectively, while of wheat is 100. Jowar GI is 61 (clinical dietetics and nutrition). 18 This also shows that wheat has high glycaemic index and rice, ragi, and jowar can be advised in diabetes. The theory of GI confirms ayurvedic perspective of diet.
The strength of the study is that it is the first study to analyze the association between different staple food categories and sugar levels. Sample size was also good. A limitation of the study is that sample was not distributed normally in all zones. Moreover, the data about other diets was not obtained and that it is difficult to rule out the effects of physical activity. Furthermore, data about diet information was retrospectively obtained and this is not prospective information.
Conclusion
The results of this article indicate that wheat is more positively associated with sugar levels, weight, and waist score of an individual. This suggests that intake of wheat which bears a high GI value may prove detrimental to diabetic subjects and hence should not be consumed more than recommended levels. On the contrary rice and ragi, which comparatively carry a lower GI value, are negatively associated with HbA1c levels, sugar levels and waist circumference. This indicates that their consumption can reduce HbA1c, total cholesterol, and LDL levels and put diabetes in control.
Footnotes
Authors’ Contributions
RN(PI) conceptualized and edited the manuscript. AA gave concept of the paper. DM and SN were involved in writing. SP was involved in raw data and analysis. AS provided National Coordination.
Statement of Ethics
Following a detailed presentation by the PI, the IYA’s IEC cleared the proposal after scrutinizing the complete project proposal including informed consent forms. The study was registered on CTRI (Registration Number- Trial REF/2018/02/017724).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.