
Abstract
Infertility is a serious reproductive health challenge that has a far-reaching impact on women’s lives as they, inevitably, are the ones blamed for the failure to conceive. Despite availability of Western treatments to manage infertility, women frequently consult indigenous healthcare practitioners (IHCP) for healthcare, preferring these services to Western practice due to reasons such as accessibility and affordability.
The study used a qualitative explorative, descriptive, and contextual design. Both purposive and snowballing technique were used to identify five women whom indigenous practitioners had assisted to conceive. Individual semi-structured interviews were conducted and data were analyzed using the Tesch method of data analysis.
IHCPs are known experts in managing infertility, experiences of women on indigenous management of infertility and continuous holistic management of infertility among women.
Keywords
Introduction and Background
Infertility is perceived as a public health concern worldwide that leads to economic burden on the society affecting various countries and healthcare systems (Kochhar et al., 2017). Infertility has adverse effects on women’s life where their motherly role and financial status depend on their ability to bear children in order to enhance their status in the community (Dierickx et al., 2019). Infertility is a worldwide health problem affecting about 60–168 million people globally. In general, universally the rate of infertility fluctuates intensely and corresponds to the frequency of preventable conditions leading to infertility (Emmanuel et al., 2019).
Fata et al. (2020) alluded that in Turkey there is high cultural burden to have children, and, therefore, infertile women seek help from different methods of care including indigenous practitioners. According to Nicolai (2017), it is projected that one out of six people worldwide experiences some form of infertility during their procreative age, and women seek help from various available treatments methods across the European countries. Babikir et al. (2021) concluded that the Sudanese women reverted to traditional management of infertility due to the fact that Western treatment is expensive and has low success rate. A qualitative study conducted in Pakistan on perspectives of patients, spouses, and infertility experts revealed that women will sell their asserts to accumulate funds for a repeated series of costly treatment processes from the Western practice that contributes to financial strain and increased level of stress (Naz & Batool, 2017).
Jiang and Li (2017) revealed that in the United Kingdom, fertility indicators such as ovulation rates and appropriate thickness of the endometrial lining are certainly influenced by Chinese Herbal Medicine (CHM) therapy, signifying an enrichment of physiological effect for conception and viable pregnancy. Infertility is a social problem that give rise to medical conditions such as depression and hypertension, and they first tend to seek help from indigenous practices. In rural Jordan, persistence and remorseless efforts to become pregnant are widespread, and women seek support from up-to-date technology and by reaching out to those offered by a community and traditional healers. In the same study, women were observed as failures to meet societal norms and expectations to bear children (Daibes et al., 2017). Similarly, in Palestine, infertility treatments are very costly, and several of underprivileged women or other women whose prior infertility treatments had failed opt for indigenous treatment to solve this problem (Jardat & Zaid, 2019).
A mixed method study on psychological distress and coping strategies among women conducted by Hess et al. (2018) concluded that Malian women with infertility experiences outstanding levels of psychological stress because their self-identity and societal status to be be mothers was groundless. Furthermore, women with infertility seek help from various practices to restore their fertility status. Norwegians perceive parenthood as a central goal in future. and experiencing obstacles by imagining a life without children may contribute to negative impact of infertility in women’s life and (Fernandes et al. 2020)
Despite the availability of Western medicines, women in Nigeria affirm that indigenous healthcare practitioners (IHCPs) are effective in the management of infertility, and that it has adverse effects affecting the social, physical, psychological, and economic well-being of the women (Dattijo et al., 2016). Qualitative research conducted in Ethiopia on beliefs and practices of traditional medicine towards women’s reproductive health concluded that IHCP has a pivotal role in their community’s cultural and primary healthcare service provision; therefore, women in particular consult with IHCP to curb different health problems including infertility (Murugan & Yared, 2018).
A study conducted in Ghana by Osei (2014) reports that some Ghanaian women are genuinely convinced that infertility is of supernatural origins, and so they utilize the services of indigenous and religious healers. Moreover, due to the birth rate of the African humanity and the social meanings of childlessness, infertile women use several health seeking strategies in an effort to have their own children. However, health-seeking behavior in Ghana is characterized by numerous factors including perceived cause and cost (Hiadzi & Woodward 2020).
In most rural parts of Africa, cultural and traditional health practices play a substantial role in all various issues of maternal health including infertility (Shewamene et al., 2017).
Little is known about the voices of women who used indigenous health practices to manage infertility in Ngaka Modiri Molema health district. Therefore this article intends to explore and describe narratives of women who used indigenous healthcare practices to manage infertility in Ngaka Modiri Molema health district. The aim of the article is to describe narratives of women who used indigenous healthcare practices to manage infertility in Ngaka Modiri Molema health district.
Problem Statement
Infertility is a health challenge that has a negative impact on the well-being of women. The World Health Organization’s (WHO) demographic lessons indicated that more than 30% of women in Sub-Saharan Africa suffer from infertility (Chimbatata & Malimba, 2016). Despite the availability of Western medicines, the women reported that IHCPs are effective in the management of infertility. The researcher, as a midwife specialist, realized that women with infertility claim to be pregnant after consulting indigenous practitioners. In Nigeria, most women preferred help from traditional and spiritual healers for infertility rather than consulting Western practice (Dattijo et al., 2016). Women of childbearing age have received continuous information regarding safe new technologies on Western treatment of infertility. but they still consult indigenous practices. In South Africa, a considerable number of women consult with IHCPs for a range of health challenges of the female reproductive system, including infertility (Joseph, 2018); other women use dual treatment and they assume the indigenous practitioners are the ones who assisted them. There is little information, however, about women who used indigenous practices to restore infertility.
Purpose
To explore and describe experiences of women who used indigenous healthcare practices to manage their infertility in Ngaka Modiri Molema District, North West Province, South Africa, in order to recommend the co-existence of such practitioners with the Western healthcare system with regard to infertility treatment.
Objectives
Explore and describe experiences of women who used indigenous healthcare practices to manage their infertility in Ngaka Modiri Molema District, North West Province, South Africa
lluminate the “voices” of women who used IHCPs whilst suffering from infertility
Propose recommendations for the co-existence of IHCPs and Western healthcare providers with regard to the management of infertility
Research Question
What are experiences of women who used indigenous healthcare practice to manage infertility?
Research Design and Methods
Research Design
This study utilized a qualitative, exploratory, descriptive, and contextual approach aimed at gaining an in-depth understanding of the narratives of women who used indigenous healthcare practices to manage infertility in Ngaka Modiri Molema health district. This research approach choice allows the researcher to obtain narratives from previously infertile women to understand the indigenous practices used to manage infertility.
Study Setting
The study was conducted in Ngaka Modiri Molema, North West Province—one of the most rural provinces in South Africa. Modiri Molema district, a rural area with a 24-hour community health center that caters for community health, has 28 wards consisting of 102 villages. The setting for this study was natural and a real-life situation that was not controlled.
Population and Sampling
The population for the study included women who sought the services of IHCPs to manage their infertility in Ngaka Modiri Molema district. The participants were purposefully selected based on the characteristics of having had problems conceiving prior to them consulting IHCPs (Brink et al., 2014). A snowballing technique identified five participants, with the aid of IHCPs who specialized in the management of infertility.
Data Collection
Semi-structured in-depth interviews collected data from five women who used IHCPs to manage their infertility until the reaching of data saturation. The interviews were audiotaped, with the consent of participants, at their respective homes. Between 30 April 2018 and 13 July 2018, the data collection took place, field notes were taken, and data were transcribed verbatim. Data analysis followed Tesch’s eight steps method.
Ethical Considerations
Ethical clearance was requested, and obtained from North West University’s Health and Research Committee (Reference NWU-00689-17-A9) prior to the commencement of data collection. The study maintained ethical considerations throughout, including requesting the IHCPs to ask for the participants’ consent before referring them to the researcher. All information gathered remained safe and was not shared with other parties to ensure confidentiality. The researcher used numbers to identify the participants instead of names to maintain anonymity during the study.
Trustworthiness
Trustworthiness for qualitative research was established through the following four strategies namely, credibility, confirmability, dependability, transferability, and authenticity to ensure that the study is credible and authentic.
Findings
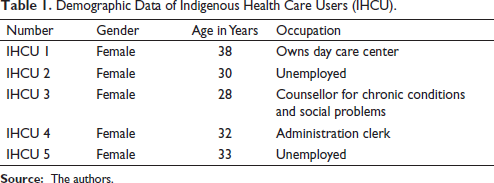
The basis for the results was the narratives of female indigenous healthcare users who had infertility issues and opted for the services of IHCPs. Presented first are the demographic characteristics of the women.
Demographic Data of Indigenous Health Care Users (IHCU).
Themes and Sub-Themes
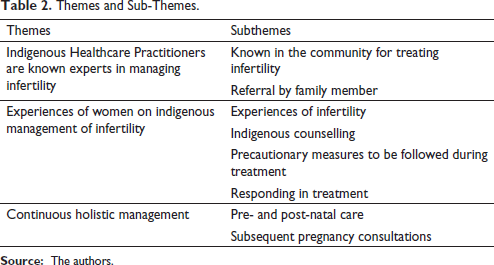
Three main themes emerged from the data analysis process in the present study: (a) IHCPs have expertise in managing infertility, (b) experiences of women on indigenous management of infertility, and (c) continuous holistic management, which describes narratives of women who used indigenous healthcare practices to manage infertility in Ngaka Modiri Molema health district (see Table 2).
Themes and Sub-Themes.
Theme 1: Indigenous Health Care Practitioners(IHCP) Have Expertise in Treating Infertility
An IHCP is highly recognized in the community in which they live as someone competent to utilize their skills and knowledge to counsel, treat, and prevent various health challenges through their experience and guidance from the spirit world (Abrams et al., 2019). It became apparent that the services rendered by IHCPs are common knowledge within the community and that information about such services travels via word of mouth. The following subthemes emerged: (a) Referral to Indigenous Healthcare Practitioner by family member and (b) Referral by other indigenous healthcare users.
Sub-Theme One: Known in the Community for Treating Infertility
The participants echoed the following statement:
The practitioner knows her work I want to tell those with problems of infertility to come and consult with her. If it was not because of her I don’t know if I could have had kids. (IHCU1)
Another participant who was satisfied with the service of a traditional health practitioner after struggling for some time with different Western practitioners in the area of women infertility, attested that
I don’t want to lie, the Indigenous Healthcare Practitioner assisted me to conceive after unsuccessful consultation with various gynaecologists for six years and on top of that I delivered twins. (IHCU4)
Another participant stated:
In our community, the traditional healer is known to assist women who are infertile to conceive. I consulted with her after one year and six months of trying and it took me four and a half months to conceive and I was so excited. (IHCU5)
Sub-Theme Two: Referral to Indigenous Healthcare Practitioner by Family Member
The recognition of IHCPs as experts is due to their ability to assist women who struggle to conceive due to various individual problems. They are trusted not only because they understand the dynamics of infertility and its management but also because people have first-hand experience of their effective methods and refer others with similar problems for assistance.
Other participants stated:
I was referred to her by my mother-in-law and she praised her based on her work. I don’t know if I deceive her but that woman she assisted me to conceive. (IHCU 4) My husband told me that we should try this granny who massage women to conceive and I agree to see her being hopeless as I have been travelling from east to west looking for help but still remains infertile. (IHCU 3)
These findings prove that women who received assistance from the IHCPs to restore their fertility status referred others; referrals were also from friends, colleagues, and significant others. Consequently, IHCPs are renowned in their vicinity due to the potential to treat infertility.
Theme Two: Experiences of Women on Indigenous Management of Infertility
This study found that women who had long-standing issues of infertility consulted IHCPs, and the narratives provided by the participants revealed that these practitioners provided effective services in the management of infertility.
Sub-Theme One: Experiences of Infertility
The participants explained how they realized they were unable to conceive, the duration of their problem and their option of consultation with an IHCP rather than Western medicines.
I started consulting with western practitioners and given treatment several times for about three years which was ineffective until I decided to stop consultations. The treatment included counselling sessions. Later that year I decided to consult with Indigenous health care practitioner and eventually after six months I conceived. (IHCU 1)
Another participant said,
I visited gynaecologists for four years and was operated twice to restore my fertility but I remained infertile and stressed. My husband took me to Indigenous Healthcare Practitioner and within three months I conceived. (IHCU 4)
Another stated,
I told her that I want to have a baby but it has been two years of trying and she gave me the medication for three months than I was pregnant. (IHCU 5)
The findings of this narrative demonstrated that infertility had a negative impact on women’s emotional and psychological status. Furthermore, women alluded to the fact that they conceived after a long period of being infertile after consulting with an IHCP.
Sub-Theme Two: Indigenous Counselling
IHCU 4 stated that the IHCPs continually counsel them during face-to-face contact, and even telephonically, and they are encouraged to pray.
Granny started by explain the causes of my problems and reassured me that is not too late I will conceive after series of appointments and she continually asked me how I feel. (IHCU 3)
Sub-Theme Three: Precautionary Measures to be Followed During Treatment
Participants expressed measures that need following when on treatment and both partners should abide by these to enhance effective treatment outcome. To confirm this, one participant said,
I was requested to boil the medication personally, let it cool off and make sure that we use enamel containers to drink not glass mugs. (IHCU2)
Another participant stated,
It was emphasised that during treatment we should avoid attending events like funerals or coming home after sunset. (IHCU 3)
Echoed by another participant,
Mmmmh … the Indigenous Healthcare Practitioner used to tell me that while on treatment we should not engage in negative arguments and to avoid disclosing duration of pregnancy to outsiders. (IHCU 5)
These statements affirm that it is expected women comply with the prescribed instructions whilst on treatment.
Sub-Theme Four: Responding in Treatment
After consultation with the IHCPs, treatment was according to guidance from supernatural powers, and users received a schedule for treatment and follow up care. The woman has to report changes or improvement in her general well-being once she is on treatment. The participants confirmed the statement by saying:
I was expected to be given enema and massaged five times, but once in two weeks and collect medication again if finished. I conceived after the third massage before fifth visit. (IHCU5)
Another participant said,
I remember that my periods were lasting for long and were irregular, after the commencement of treatment my periods become normal and on the third month menstruation disappeared and when I told her she said you requested a baby so?... (she smiled) I was very excited and I informed my husband. (IHCU1)
The participants further indicated that while on treatment, their general well-being changed as there were no minor complaints, such as headaches or dizziness, and a return to fertility was evident.
According to these narratives, all the women responded well to treatment and conceived.
Theme 3: Continuous Holistic Management
Consultation with the IHCP leads to the establishment of trust, as after delivery the woman will continuously request assistance with other health challenges. The women revealed that the IHCPs provided preventive and curative treatment for other underlying health problems. The following sub-themes were identified: (a) pregnancy and (b) subsequent consultation for other conditions.
Sub-Theme One: Pre- and Post-Natal Care
The participants mentioned that after conception, there were a series of appointments for treatment, massage and monitoring the progress of pregnancy.
The Indigenous Healthcare Practitioner requested me come for medication every week and I conceived my first child she also explained changes that will occur during pregnancy, e.g., mood swings and changes on the breast. (IHCU3)
Another participant said,
When I realised that I am pregnant I told the traditional healer and she immediately changed my medication and told me that she will stop with massage as is not safe in early pregnancy. (IHCU4)
In this study, the women affirmed that during the pregnancy, the IHCP continuously monitored the fetal growth to ensure a healthy viable pregnancy. This encourages the women to follow the same process with subsequent pregnancies.
Sub-Theme Two: Subsequent Pregnancy Consultations
The perception is that the IHCP is the main source of help for mother and child in all their daily health challenges. In this narrative, the women alluded to the fact they subsequently consulted the IHCP for post-pregnancy health challenges, and for mother and baby rituals.
One participant said:
Traditional health practitioner assisted me during post-natal period and during that time I developed an abscess on the right breast and she treated it. (IHCU1)
Another participant mentioned,
After delivery I experienced episodes of dizziness and she gave me the medication and I felt much better and she performed ritual when my baby was three months old. (IHCU3)
Another said,
My baby was crying almost all the time and she performed a ritual for both of us and the baby stopped crying and slept peacefully. (IHCU5)
The participants affirmed the IHCPs were effective in the management of all health challenges, including infertility. The findings revealed they have limited visits to the Western practice, which were for immunizations and other emergencies, such as fractures, and during disease preventive campaigns.
Discussion
According to WHO traditional medicine strategy (2014–2023), indigenous medicine is as follows:
[T]he sum total of the knowledge, skill and practices based on the theories, beliefs, and experiences that are indigenous to different cultures, whether explicable or not, and used in the maintenance of health as well as in the prevention, diagnosis, improvement or treatment of physical and mental illness.
Regardless of the modern technologies in place to manage women with infertility, women consult with IHCPs to restore their fertility. In the findings of this study, women stated that IHCPs were experts in the management of infertility, as women conceive and ultimately have viable pregnancy. The participants also added that the indigenous practitioner’s treatment process was holistic, as there were continuous counselling sessions, massage, and medications. In Nigeria, the majority of women (71.7%) had sought help from traditional and spiritual healers for infertility before presenting to the hospitals (Dattijo et al., 2017). Participants also reported that the community knew the practitioners based on their ability to restore fertility, therefore women refer others with infertility problems for assistance. In Sierra Leone, James et al. (2018) assert that women quote friends and family members as the main influencers in their decision to consult IHCPs to restore fertility. The literature reveals that 80% of the world’s population consults IHCPs for all health challenges, including infertility (Shewamene et al., 2017). In this study, women confirmed that the practitioners were accessible and affordable, and hence they are the preferred source of help. In addition, the findings revealed that the practitioners established a mutual relationship with the women, leading to continuous consultation post pregnancy and in preparation for subsequent pregnancies.
Women who suffer from infertility listen and abide by instructions regarding treatment to ensure an effective treatment outcome. The findings revealed that infertility outcomes depend on the conduct of the woman and her partner, as there were treatment restrictions to be followed that enhance the effectiveness of treatment. Furthermore, the women affirmed that the practitioner emphasized their compliance to the treatment and to report any strange feeling or illness, as that can be the sign of success or that treatment needs to be altered. James et al. (2018) concluded that infertility in African society is often concomitant with supernatural and spiritual causes, which leads to consultation with traditional healers as a first choice in health-seeking behavior. In the African culture, the marriage mainly denotes fulfilment if the couple conceives and bears children (Chimbatata & Malimba, 2016).
The participants indicated that prior to, or during consultation, they undergo couple counselling according to their identified problems. The counselling encompasses treatment process and the outcome. According to literature, IHCPs are experts, with roles that include, but are not limited to, custodians of the traditional African religion and customs, education about culture, counsellors, mediators, and social protectors (Zuma et al., 2016). In addition, findings proved that counselling was essential and an ongoing process that promoted adherence to treatment.
Findings of this study revealed that various women became aware of their infertility status, which existed at various intervals, and choose to consult with IHCPs. Most of the women in Albania indicated they went around for years using alternative advice before seeking help for their fertility (Tahiri et al., 2014). Findings of this study divulged that women with infertility suffer social isolation and are emotionally abused by husbands and relatives; hence, they are the ones who seek treatment first.
Women who consulted with IHCPs indicated that after a series of treatments, which included massages, they conceived and delivered healthy alive infants. The IHCPs provide holistic care to infertile women, and their spiritual and emotional status is attended to through prayers and counselling prior to consultation. Conception in Africa not only defines womanhood but also bestows dignity and respect to the family as well as safeguards the inheritance (James et al., 2018). In accordance with the earlier statement, women in this article strived to conceive in order to receive the honor of a mother, and they did everything in their power to consult, preferably with an IHCP, to curb infertility. As noted earlier in this article, IHCPs are major sources of help, and women and their infants continually consult them with other health challenges. The women asserted that they would continue with consultations even with subsequent pregnancies.
Recommendations
Based on the findings of this article, the recommendations were for research, policy, practice, and education. More research on infertility among black women who use indigenous practices needs to be conducted in other rural provinces in South Africa. Policy in relation to collaboration of indigenous practice and Western practice should be developed and implemented. In nursing practice, individuals require screening for reproductive health challenges as they can complicate to infertility if not properly managed. Nursing education should ensure that topics on human reproduction and related indigenous practices are included in midwifery module to equip student on diagnosis and management of infertility.
Limitations
The clearest limitation of this article was that many IHCUs found it difficult and became emotional explaining their infertility journey; therefore, the researcher had to look for those who were open and willing to participate in this article.
Conclusion
The main objective of the article was to describe and to explore the experiences of women who used indigenous health care practices to manage infertility in Ngaka Modiri Molema health district. IHCPs are custodians of cultural practices through spiritual guidance and consultation with ancestors to provide holistic care to individuals with health challenges, including infertility. Based on the findings of the article, the gift of a known expert, holistic, and continuous care, indigenous consultation and counselling were the main themes. The findings of this article further revealed there is a mutual relationship between the practitioner and the user, as affirmed by continuous consultation for physical, psychological, emotional, and spiritual problems. In addition, it is clear that the IHCPs are widely used as main sources of help in terms of restoring fertility, and are accessible and affordable. The article revealed that even though infertility is a couple’s problem, women are the ones who bear the blame and first seek help in order for recognition as mothers. It is further evident that the IHCPs have ability to manage infertility based on the findings of the article.
The women who participated in this research experienced healing by IHCPs, and they advocate their services for the reasons mentioned and holism of care. As Western-trained health providers, we cannot continue to ignore the genuine voices of healthcare users where evidence is glaring. Hence, the researchers support the women and advocate for the co-existence of the use of IHCPs and Western healthcare providers in the management of infertility, as it is a complex phenomenon.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.