
Abstract
The aim of this study was to evaluate leadership competencies amongst public health professionals in Nigeria. A cross-sectional survey was carried out between October and December 2019 at the International Center for Advocacy on Right to Health (ICARH, Abuja, Nigeria). The study involved health professionals who are required to provide leadership in their programmes for effective outcomes. We used a validated and robust leadership competency questionnaire, developed by the European Union (EU) Leadership in European Public Health for Improved Evidence (LEPHIE) (Smith et al., 2015).
The survey had a 60% response rate: 63.9% of respondents were male and 36.1% were female, with a mean respondent age of 33.7 years. There was a statistically significant difference (p < .001) between respondents’ reported current competence level and the level they deemed necessary for optimal performance in their job. The respondents rated their current level of competence significantly lower than their required level of competence. Respondents had the highest level of competence in the following domains: ‘ethics and professionalism’ and ‘collaborative leadership: building and leading interdisciplinary teams’. They also perceived that these competencies were the most important for their job positions, as they were evaluated highly on the required level of competencies.
Nigerian public health professionals surveyed identified that exemplary leadership in health care greatly depends on ethical professional conduct and interdisciplinary collaboration. Findings from this study show that the respondents rated their existing competencies significantly lower than the leadership competencies required for optimal performance in their roles.
Introduction
Leadership is a key determinant in the growth and success of any institution (Aarons et al., 2015). The concept of leadership is a complex and ever-changing process that has been interpreted in many ways. Situational leadership, self-directed leadership, transformational leadership and many more are some of the documented theories and models of leadership (Weiskittel, 1999). The International Journal on Leadership Studies provides an integrative definition of a leader as:
A leader is one or more people who selects, equips, trains, and influences one or more follower(s) who have diverse gifts, abilities, and skills and focuses the follower(s) to the organization’s mission and objectives causing the follower(s) to willingly and enthusiastically expend spiritual, emotional, and physical energy in a concerted coordinated effort to achieve the organizational mission and objectives. (Winston & Patterson, 2006)
Currently, discussion of the significance of leadership capacity and impact has been limited in the healthcare sector, especially in culturally diverse countries (Ghiasipour et al., 2017). The failure of leadership in the field of health care is regarded as one of the salient issues in society. Several healthcare institutions have been plagued with many challenges, and there has been action to enable improved service delivery and efficiency. The conceptual framework for improving leadership and management capacities from the WHO (2007) provides relevant organisational skills required for successful delivery of health services.
An important consideration when health professionals consider the optimal leadership style for use in organisations, teams and groups is the capacity for the leader to adapt their leadership style in the context of different settings and planned outcomes (Samarakoon, 2019). Health leaders operate in an environment that requires the capacity to manage power and change in the pursuit of quality outcomes for consumers (Kumar, 2013). Operating in the unique environment of healthcare requires a clear understanding of leaders’ capacity and requirements for change and improvement regarding their leadership competencies.
‘Competency’ is regarded as the professional skills, knowledge and attitudes needed to perform a job. Healthcare workers and managers need additional skills to complement the planning, direction, organisation and control functions of traditional management in complex healthcare systems to enable their success. These additional skills are essential for efficient patient care and continuous improvement in the quality of health (Munyewende et al., 2016). Deficiencies in competent leadership and governance in the healthcare sector have long remained a major deterrent to the growth and development of healthcare systems in most low- and middle-income countries (LMICs), including Nigeria. According to the WHO (2007), leadership and governance are directly connected to not only the role that government plays in health but also the activities of stakeholders whose impact is felt in health. The Federal Ministry of Health (FMOH) in Nigeria has recognised eight major factors that hinder the leadership role of government in the healthcare sector: (a) poor explanation of roles and responsibilities of key actors; (b) lack of essential management and mentorship tools; (c) challenges of promoting inter-sectoral collaboration with other arms of government; (d) poor communication and enforcement of health policy implementation; (e) non-existent legal support for the implementation of health policies; (f) current policies do not include conclusive roles and responsibilities of the private sector; (g) poor budget management practices and (h) inadequate funding of the healthcare sector (Mano et al., 2018). The last two decades have seen a surge in the existence of private and non-profit healthcare organisations in many LMICs, including Nigeria. This has been seen as extremely beneficial, as it has helped and supported the already heavily burdened public healthcare system in LMICs.
Inefficient leadership practices have resulted in ineffective healthcare systems in the majority of LMICs, including Nigeria, with most of the population receiving inadequate health care and having low access rates to health systems (Abubakar, 2019; Petersen et al., 2017). There are reported inefficiencies and ineffectiveness of leadership in the Nigerian healthcare sector regarding the failure to provide quality health care. This includes a massive movement of public health professionals to developed countries in search of better working conditions; a lack of funding; the battle for supremacy among healthcare professionals; conflicts over collective bargaining agreements and inadequate policy frameworks (Adinma & Adinma, 2010; Oyewunmi et al., 2015; Uneke et al., 2012). Asuzu et al. (2015) indicate that because of inefficiencies and failures in the healthcare system, Nigeria has been unable to manage epidemics and other health crises. In overcoming these challenges, and to carry out their task as leaders, there is a need for improved leadership practices in the Nigerian healthcare system, and this calls for a review of contemporary evidence about the leadership competencies of its healthcare professionals (Abubakar, 2019; Oyewunmi et al., 2015). It is important to understand the links between leadership and organisational success, competencies’ development and efficiency, as well as the gaps identified between these constructs in available research.
Leadership Competencies of Public Health Professionals in Nigeria
Leadership competencies are crucial in any organisation, and particularly in the healthcare sector, where the focus is the provision of high-quality healthcare service (Witman et al., 2010). Olu-Abiodun and Abiodun (2017) conducted a cross-sectional study focusing on the transformational leadership behaviour among 176 nurses in Ogun state, Nigeria. They concluded that nurses perceived their nurse leaders using transformational leadership, with these perceptions dependent on the work setting and the qualification levels of the nurses. This work concluded that for nurses in the general hospital setting, actions and examples of nurse leaders inspired followers towards a shared vision. These findings are consistent with the adoption of a transformational leadership style involving high levels of interpersonal engagement to inspire action (Witman et al., 2010).
This contrasts with a study conducted by Archibong (2014) that reported lower scores regarding the perception of nurses on transformational leadership style in a tertiary hospital in Enugu, South-East Nigeria. Further, Adeleye and Aduh (2014) indicate that leadership in tertiary and general hospital nursing differs due to the different status and settings of the hospitals, thus explaining the variable perceptions of the leadership styles applied. Further, Ugwa (2014) reported that transformational leadership is one of the most commonly used styles by nurse leaders in Nigeria. Onwe (2014) reported that the application of transformational leadership style, which is attributed to a high level of interpersonal skills, is linked to job satisfaction by nurses, whereby they feel engaged and included, with inspiration to meet common goals. Asuzu et al. (2015) link efficiencies in Nigerian healthcare practices, such as providing leadership in epidemics, to an effective healthcare centre. Further, Oyewunmi et al. (2015) noted that leadership that does not illustrate emotions and has little consideration for the emotions and challenges faced by employees is merely endured and has little loyalty from its followers, unlike leadership with empathy that is supportive of employees and thus has the capacity to promote commitment and loyalty to common goals. Gabriel (2016) supported these contentions and recommended inspiring and engaging employees, arguing against toxic behaviour, such as authoritarian leadership with restriction of autonomy and initiative, as well as micro-managing employees. Leadership styles display specific skills, such as empathy, which critically influence the performance and productivity of nurses, as well as positively impact the outcomes of patients. Similarly, Oyewunmi et al. (2015) linked leader’s emotional intelligence with improved employee performance in the Nigerian health sector. They argued that this enables the leaders to carry out their roles as leaders and to handle the multiple challenges within the country’s public healthcare sector. Oyewunmi et al. (2015) and Abubakar et al. (2018) highlight that poor policy frameworks that do not provide for leadership can result in inefficiencies in healthcare systems. Emotional intelligence is, thus, a critical competency for public health professionals. Leaders with high levels of emotional intelligence are linked to effective decision-making and conflict management, whereby they can adequately scan the environment of the healthcare sector, consider the consequences to their actions and use the most appropriate leadership approaches that are acceptable to their followers (Oyewunmi et al., 2015). Gabriel (2016), Mshellia et al. (2016) and Oyewunmi et al. (2015) observed that inaction due to poor leadership competency negatively impacts the performance of employees and service provision in Nigerian public hospitals. Comparing leadership competencies in public and private hospitals in Nigeria, Yakubu et al. (2019) reported that perceived competencies are low for leaders who are unable to promote effective decision-making and conflict resolution. Further, the study indicated that there was no difference regarding hospital affiliation and status but reported that some competencies were higher in private hospitals than in public hospitals.
Inadequate leadership competencies in Nigeria can be rectified using experiential training on effective decision-making approaches, effective conflict management, among others (Oyemakinde et al., 2014). Yakubu et al. (2019) indicated that neglecting leadership competencies makes it challenging to ensure efficiency in health systems and achieve universal health coverage.
Competency Development and Organisational Success
Human resources in the healthcare system in Nigeria face many challenges, with conflicts and disagreements on overpayments, inadequate leadership and management of healthcare resources and allowances and collective bargaining agreements with no focus or plans for professional development (Abubakar et al., 2018; Aturaka et al., 2018; Oleribe et al., 2016, 2018; Petersen et al., 2017). Onwe (2014) links inadequate leadership competencies with employee dissatisfaction and lack of motivation. Several writers argue that this impacts performance, thus affecting the success of facilities in providing optimal health care. Abubakar (2019) focused on professional skills and employee behaviour in the decision-making process of patients regarding which hospital to seek health care from in the North-West region of Nigeria, and concluded that employee competencies influenced the patients’ choice of hospital. The study indicated that efficient management processes within the hospital, through appropriate leadership, are linked to customer satisfaction and their choice of particular hospitals to access care. Dankyau et al. (2017) demonstrated a link between leadership competencies of nursing and non-nursing managers, and employee satisfaction and health outcomes, in an urban tertiary hospital in North–Central Nigeria. Ekenedo and Ezedum (2013) provide a rationale for competency development, arguing that it results in competencies such as teamwork and emotional intelligence, leading to improved health practices. However, Donald (2015) argues that the challenges affecting healthcare professionals are systematic, needing a comprehensive strategy to improve the healthcare system. This indicates the need for policy change within the healthcare systems, with elements such as leadership competencies being required for those in leadership and management positions.
Job satisfaction and leadership style among nurses in Nigeria are reported as being enhanced when they are led by those with democratic leadership competencies, compared to those with autocratic leadership competencies (Oyewunmi et al., 2015). Adeloye et al. (2017) also linked competencies in leadership with high performance and job satisfaction for employees. A study about Ugandan healthcare employees reported that the leadership styles used are related to motivation, teamwork and satisfaction (Musinguzi et al., 2018).
Job satisfaction has been linked with motivation, teamwork and improved performance, resulting in high-quality provision of health care (Dennis & Oluwatelure, 2016; Misener et al., 2007; Park et al., 2018). Therefore, improving the leadership competencies of healthcare professionals will improve satisfaction, motivation and teamwork for those being led, resulting in an enhanced and efficient healthcare system. Uneke et al. (2012) studied leadership and governance competencies, concluding that leadership development is linked to a more successful and efficient healthcare system, and recommended the implementation of training for healthcare professionals on different leadership competencies. Abubakar et al. (2018) link high-quality care by healthcare professionals to efficient leadership, where public health leaders provide direction for employee behaviour. However, Oyewunmi et al. (2015) indicate that competency development among public health professionals in Nigeria is limited due to inadequate funding. Adinma and Adinma (2010) support this, stating that providing funding to improve efficiency in the healthcare system is an untapped solution by which leadership competencies can be improved. In support of competency development, Uzochukwu et al. (2015) emphasise the need for healthcare financing to ensure that the operations within systems run smoothly, but also that healthcare professionals have the appropriate competencies and capacities.
Leadership and Public Health System Efficiency
Efficiency within public health systems has been linked to leadership competencies and skills. Adeloye et al. (2017) argue that employees’ perception of effective leadership is positive and valued. In contrast, Ojo and Akinwumi (2015) investigated the role of doctors in managerial and leadership positions, as well as healthcare resources in Nigeria. They reported that there is a perception of poor management and leadership skills by the general public and by some healthcare workers. Additionally, Asuquo (2019) concluded that effective leadership is yet to be actualised in research and policy in the country, despite its critical role in achieving healthcare goals. In Nigeria, most private and public hospitals are under the management of medical doctors, while other leadership positions are filled by nurses (Munyewende et al., 2016). Yakubu et al. (2019) indicate that those in a leadership position are referred to as clinical specialists, with the assumption that they have appropriate competence in providing leadership. However, most of the hospitals in Nigeria are inefficient and marked by constant industrial strikes, poor staff motivation and strained relationships among the healthcare professionals. Abubakar et al. (2018) report that the healthcare system in Nigeria is characterised by the monopoly of government facilities over private settings regarding the human resources available, technological capabilities and the cost of services. Olu-Abiodun and Abiodun (2017) explain that poverty is high in the country, with most of the population unable to afford to access private health care and instead seeking public hospital care. Leadership is an effective strategy that can be used to enhance and promote efficiency within the public health system (Govender et al., 2018; Mulenga et al., 2018). Therefore, it is crucial to achieve improved healthcare delivery through improved leadership.
Various studies in Nigeria provide evidence of the link between employees’ behaviour and efficiency in leadership. One element affecting employees’ behaviour within the healthcare sector is the role played by doctors as leaders (Witman et al., 2010). According to Adeloye et al. (2017), the Nigerian health workforce is faced with crises and characterised by distrust and recurring conflicts, with the dominance of doctors being favoured when compared to nurses, laboratory workers and pharmacists. Ojo and Akinwumi (2015) agreed and reported that doctors are mostly the managers and leaders of healthcare facilities, despite indicating low levels of leadership competencies. Adeloye et al.’s (2017) study further explains that favouring doctor appointments has resulted in disputes and conflicts over salaries, consultancy status, leadership and allowances, which negatively impacts on the efficiency of the healthcare system. It is essential for a healthcare system to have effective leadership, with teamwork, collaboration and efficiency in resource management being promoted among the healthcare professionals (Gordon & Borkan, 2014; Rowe, 2010). Gabriel (2016) agrees and recommends the training of supervisors to develop emotional intelligence, enabling them to appropriately manage their employees by illustrating positive behaviour, such as teamwork. Dankyau et al. (2017) further observed that supervisory managers—both nurse and non-nurse—should be continually assessed for leadership competency, and specific training and retraining provided, to ensure capacity and effectiveness. Oyewunmi et al. (2015) recommended that leadership should be empathic, recognising and valuing employees in order to develop more reliable and healthier working relationships within the healthcare setting. While doctors clearly can continue with their roles as managers of public health resources and other leadership positions, Ojo and Akinwumi (2015) recommend that they need to be trained in leadership competencies to handle the current challenges and evolving role of leadership in health care. Asuquo (2019) argues for the case of nurse leaders, indicating that mentoring, adequate resource provision, nurse inclusion in management and policy development, as well as overall improvement of leadership competencies, provide nurses with leadership opportunities in the Nigerian healthcare system. Lunden et al. (2019) and Welcome (2011) advocate for improvements in leadership capacity and professional development.
Research conducted on leadership competencies in the healthcare system in Nigeria reports a performance gap, despite evidence indicating the link between competencies and organisational efficiency and success. There is an identified need for healthcare organisations to ensure that leadership is a high priority and to identify measures and assessments of competency among their leaders, so that appropriate support and strategies are used to improve their competency levels. Research in Nigeria has focused on key leadership competencies, such as interpersonal skills, emotional intelligence, decision-making, conflict management and prudence in the management of resources; however, little focus has been given to critical competencies such as communication, political skills and social intelligence. The aim of this study was to evaluate current leadership competencies amongst public health professionals in Nigeria.
Methodology
A cross-sectional survey was carried out between October and December 2019 at the International Center for Advocacy on Right to Health (ICARH, Abuja, Nigeria). ICARH is a non-governmental organisation established in 1999 for the main purpose of contributing to policy issues affecting the rights of sexual minorities and people living with human immunodeficiency virus (HIV)/acquired immune deficiency syndrome (AIDS) in Nigeria, through research, analysis, training, awareness campaigns development and advocacy. ICARH works to reduce the incidence, prevalence and impact of HIV/AIDS amongst key populations in Nigeria. ICARH has played a key role in the Presidential Comprehensive Response Plan, aimed at contributing to the national HIV/AIDS response.
The study sample included ICARH staff members, who are directly involved in the creation, development and implementation of healthcare programmes in the organisation. These health system professionals are required to utilise leadership capacity to achieve successful programme development and delivery in the country. A total of 120 staff members were working in ICARH at the time of the research, and all were invited to participate in this study. Therefore, 120 questionnaires were distributed. We received 72 completed surveys (response rate: 60%).
A structured and self-administered questionnaire was applied. The questionnaire was developed to bridge gaps in leadership competency development, concerning competency-based and continuing education, as existing frameworks do not specifically highlight leadership. The main part consisted of 52 competency statements categorised into eight domains. Respondents were asked to evaluate the current level of their leadership competencies and the level required (desirable) for their position/function. Answers for items of each subscale ranged from one competency level (‘minimal’) to five competency levels (‘maximal’). The competency statements were taken from the Public Health Leadership Competency Framework, which was developed as part of the Leaders for European Public Health project, supported by the European Union (EU) Lifelong Learning Programme (Czabanowska et al., 2014). This Leadership in European Public Health for Improved Evidence (LEPHIE) framework was developed by an intensive literature review and experts’ review/assessment (Smith et al., 2015), and it was used and validated in studies conducted in different countries, including Albania (Caushaj et al., 2019; Pampuri et al., 2015) and Lithuania (Stankunas et al., 2016), as well as in learning sessions for health care professionals (Department of International Health, 2014).
Data analysis commenced by creating and labelling all necessary variables using Statistical Package for the Social Sciences (SPSS) analysis software. For the quantitative data, the eight domains (containing 52 competency statements)—for both the current and required levels of competencies—were: systems thinking; political leadership; ethics and professionalism; emotional intelligence and leadership in team-based organisations; leading change; leadership and communication; collaborative leadership—building and leading interdisciplinary teams and leadership, organisational learning and development.
Descriptive statistics were analysed for competency statements and their domains, and included mean, median, interquartile range, confidence interval, standard deviation and others. We applied the Kolmogorov–Smirnov test to check for normality of the distribution, and it was found to be significantly different (p < .001). Since the distribution was not normal, non-parametric the Mann–Whitney U test was applied to compare levels of different domains between gender, age, years of experience, job position and career groups. The Wilcoxon rank sum test was applied to assess the differences between current and required levels. Some features of competencies were categorised into two groups: participants’ ages ‘less than 35 years’ and ‘equal or more than 35 years’; years of experience in the organisation ‘1–4 years’ and ‘4–8 years’ and information on ‘biomedical’ and ‘non-biomedical’ career/background experience.
Approval for the conduct of this research was granted by the ICARH organisation and the Bioethics Centre of the Lithuanian University of Health Sciences.
Findings
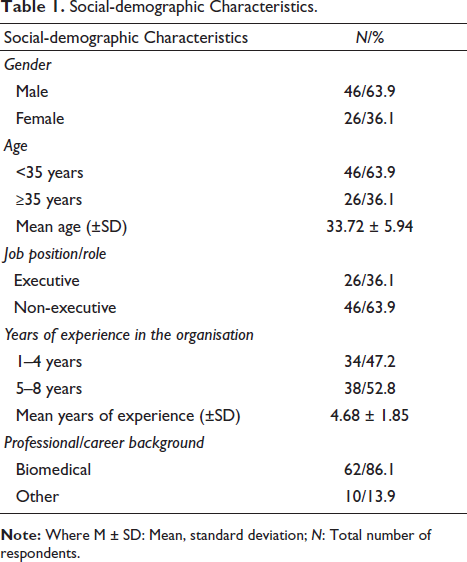
The main demographic characteristics of respondents are presented in Table 1. For this cohort, 46 (63.9%) were male, and 26 (36.1%) were female. The mean age of respondents was 33.72 years (SD = 5.94). The majority, 62 (86.1%) of respondents identified that they had a biomedical professional or experiential background.
Social-demographic Characteristics.
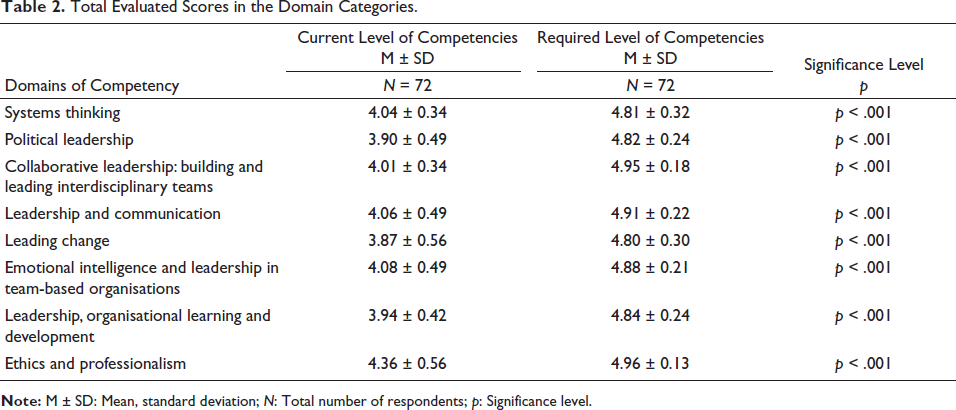
The total scores for all participants for all competency statements were included in the established eight domains (see above in Methodology section and in Table 2). A statistical significance was observed between respondents’ reported current and required levels of competency for each domain. The respondents perceived and rated their competencies in each domain positively; the highest was in ‘ethics and professionalism’ (4.36 ± 0.56), and the lowest in ‘leading change’ (3.87 ± 0.56). As for the required level of competencies for their jobs, the respondents rated all competencies in each domain highly, with ‘ethics and professionalism’ and ‘collaborative leadership: building and leading interdisciplinary teams’ being the highest. Overall, a significant gap was revealed between the current level of competence and the required competence levels of the respondents (Table 2).
Total Evaluated Scores in the Domain Categories.
The Mann–Whitney U test was conducted to determine whether significant differences existed between the socio-economic groups of respondents (Table 3). For all domains except one, there were no statistically significant differences between respondents aged <35 years and those aged ≥35 years for both current and required competency levels (p > .05). However, there was a significant difference in the required level of competency for the ‘ethics and professionalism’ domain (p = .013); this means that respondents aged <35 years old had rated competencies in ‘ethics and professionalism’ higher than respondents aged 35 years and above.
Survey Results Across Eight Study Domains.
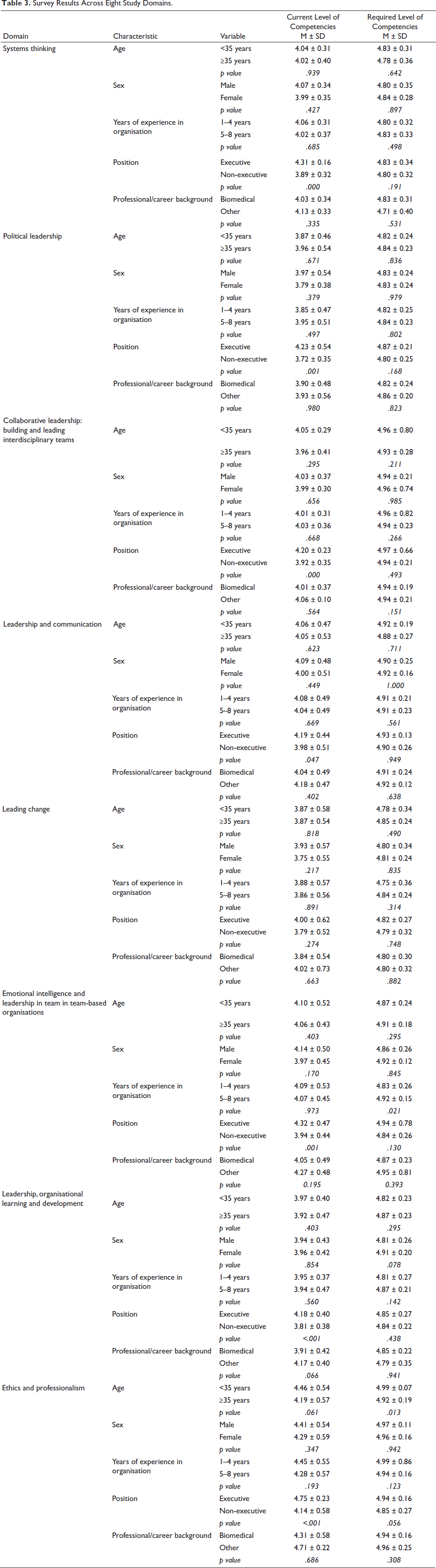
As shown in Table 3, there was a statistically significant difference in the emotional intelligence domain (p = .021). Respondents with 1–4 years of leadership experience had a significantly higher level of emotional intelligence than leaders with 5–8 years of experience. For the other domains, there were no significant differences between the two groups (p > .05).
In Table 3, for each of the domains examined, whether in the current or required competency levels, there were no statistically significant differences between males and females (p > .05). Therefore, leadership competency levels for all the domains were similar between males and females.
In Table 3, respondents who occupied executive positions rated their current competency levels for all domains significantly higher than their non-executive counterparts (p < .05). There were no statistically significant differences between executive and non-executive positions for the required competency levels (p > .05). Each of the domains examined, whether for current or required competency levels, demonstrated no statistically significant differences between respondents with and without a biomedical backgrounds/experience (p > .05). Therefore, leadership competency levels for all the domains were similar between those with and without biomedical-work experience.
Discussion
The features of our study design limited the opportunity to interview several public health professionals in their organisations, as the survey instrument used enabled the gathering of a range of information about leadership competencies and leadership professionals within the organisation were distributed across a wide geographical set of locations. Therefore, the response rate (n = 72) was not sufficient to represent a national target population. Nevertheless, the findings from our research can still be used to make projections on the leadership competency levels of public health professionals in Nigeria. It is important to note that this study involved professionals working on research, analysis, training and campaign awareness strategies, and it examines their leadership competencies in those roles. It is not necessary to hold positions of leadership to be required to engage and use leadership skills, traits, behaviours and power to affect the engagement of others in the attainment of vision and goals. Moreover, public health professionals need to be able to assess the leadership behaviour of colleagues to learn and advance their practice.
A statistically significant difference existed between the respondents’ current perceived level of competencies and what they deemed is required for their job position. According to the results, respondents had the highest level of competence in the domains of ‘ethics and professionalism’ and ‘collaborative leadership: building and leading interdisciplinary teams’. They also perceived that the competencies in these domains were the most important for their job positions, as these were evaluated highly in the required level of competencies. In addition, findings from our study show that Nigerian health professionals have evaluated their current competence levels as significantly lower than the required level for optimal performance in their jobs.
The findings in Tamulionytė’s (2016) study in Lithuanian public health institutions showed that health professionals also had a higher current competence level in ‘ethics and professionalism’. It also showed that these health professionals rated their current competence levels significantly lower than the required levels for their jobs. The trends between the Lithuanian study and ours are quite similar.
Another similar study was conducted in Albania with 297 public health professionals and the results showed significantly lower-rated scores for the current competence level and higher scores for the required level of competence among the professionals (Pampuri et al., 2015). The Albanian study results are also quite similar when compared to our study.
These comparisons between Nigeria and findings from countries previously studied as part of the EU LEPHIE are interesting and valuable, given sector changes in all three countries around sustainability, transformative plans and strategies, financing and the strong use of the public system in the delivery of health care. These comparisons also relate to requirements and their competencies in leading for change and reform. The organisation and national objectives of these comparison countries (Lithuania and Albania) in relation to objectives and strategies for their health systems may be different, but current developments, reform and change, identified capabilities and expectations of health leaders within these countries make for useful and constructive comparison and understanding of the identified competencies and learning aspirations of leaders in the Nigerian health system.
The highest evaluated leadership competency statement in this study was exercise the sensitivity needed to communicate with diverse cultures and disciplines. This is quite interesting and important because it reflects the level of cultural competence of public health professionals in Nigeria, which is an important asset for a public health leader. Nigeria is a multi-ethnic country, and public health professionals have recognised cultural competence as an important tool and strategy for successful healthcare service delivery and project implementation. Capabilities in working with people across culturally diverse backgrounds are important competencies related to the context and application of leadership with followers. Agger Gupta defined cultural competence as ‘a continuous process of seeking cultural sensitivity, knowledge and skills to work effectively with individuals and families from diverse cultural communities and with their culturally diverse providers’ (Kongnetiman & Eskow, 2009).
Participants identified usefulness and value in developing their political (power), change management skills and overall leadership in the context of organisational learning and development. These findings are consistent with other identified (Kumar, 2013) insights and studies of leaders operating in the healthcare environment. These leadership competencies would be important given the nature and context of the organisation in which respondents to the survey work. The capacity and ability to influence change and reform in complex public health policy, operations and culture require the capacity for leaders to adopt and adapt different approaches in the leadership competencies to achieve successful outcomes.
Recognition and further development of skills in sensitively communicating across diverse cultures and disciplines are a critical initiative with important translational opportunities in other healthcare settings.
Betancourt et al. (2005) showed that the purpose of cultural competence was to develop a system with the capacity to provide the best quality of health care to a patient population, irrespective of ethnicity, language or race. In 2004, Leishman (2004) conducted an interesting study on the cultural competence of nurses in Scotland. The findings revealed a lack of knowledge and understanding regarding the diverse cultural groups of the population they served and were used to develop a nursing education framework that involved the concept of cultural competence (Leishman, 2004). Singh et al. (2017) conducted a study in 2017 to assess the perception of cross-cultural training among Canadian residents in graduate medical school and found that this aspect of training was only undertaken by residents in the fields of psychiatry and family medicine. Even the residents remarked that there was no formal evaluation for this training, showing how little attention is accorded to cultural competence in healthcare education.
Cross-country migration has been on the increase, and several countries, like Canada and the United States, as examples, have continued to witness an unprecedented rise in the number of immigrants, which is affecting immigration policies and immigrant health. This invariably means a culturally diverse population requiring a proportionate response from those involved in public health leadership. This international comparison provides useful and salient understanding of how health systems require their leaders to understand and respond to cultural change in countries populations. Cultural competence is an emerging aspect of leadership that must be inculcated in competency-based education of healthcare professionals globally. This can have the greatest impact on the development of well-rounded public health leaders.
Strengths and Limitations of the Study
Few studies have been carried out in Nigeria to assess leadership competencies, and our study employed a robust and standardised leadership competency questionnaire. The competency statements used for evaluation in this study highlighted many key areas that have been silent in previous studies. The results from this study can be used to identify key areas for development of public health professionals and can even help in the formulation of a new hypothesis for further research. Leaders from the organisation studied operate across various parts and domains of the public health system in Nigeria. Those surveyed provide an effective range of information, given their background, role and function, to make the important and interesting findings from this study useful to public health professionals across the country.
Conclusive data on the number of public health professionals working in Nigeria were unavailable. Therefore, these results can only represent the research participants in the organisation included in this study, not an overall target population. However, the results can be used as a projection of the leadership competency level of a significant cohort of public health professionals in Nigeria.
Conclusion
Public health professionals from the organisation in this study highly rated their current competencies in the domains of ‘ethics and professionalism’ and ‘collaborative leadership: building and leading interdisciplinary teams’. Respondents also reported that the competencies in these domains were the most important for their job positions, as they were evaluated highly in the required level of competence. Findings from this study also showed that the respondents rated their existing leadership competencies significantly lower than those required for optimal performance in their jobs. This signals a need for expediting continuous learning and professional development. These results can be used as a projection of the leadership competence levels of public health professionals in Nigeria.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.