
Abstract
Our study sought to examine how and why political leadership and institutional memory affected the implementation of Health 2015, a public health programme prepared following the principles of the Health in All Policies (HiAP) strategy, between 2001 and 2015 in Finland. We analysed the data using a realist explanatory case study method. We found that the HiAP strategy did not have a strong leader who was able to generate interest in HiAP among other policymakers. This contrasted with the Finnish success story in previous decades when several interested elected politicians and high-ranking civil servants promoted the implementation of healthy public policies. Our results also pointed to institutional amnesia. During the implementation of Health 2015, a transition to project-based implementation, the retirement of many long-term policymakers and a change from the financial steering of local authorities to steering by information took place. The subsequent institutional amnesia was followed by discontinuity of previous institutionalised HiAP implementation structures and practices, such as intersectoral working groups.
Introduction
Health in All Policies (HiAP) is a strategy that seeks to take health considerations into account in all societal decision making (Sihto et al., 2006). In addition to the health sector, other policy sectors also make decisions and take actions that affect health and its distribution in the population. For a health policy to be successful, there needs to be multisectoral cooperation to protect and promote health, as well as an adequate understanding of the health implications of decisions that are being made in different policy sectors (e.g., environment, education, housing, transport, employment, economy) (Ollila et al., 2013; WHO, 2014).
Initiatives based on the HiAP strategy are typically coordinated by official bodies of national governments, although they may also involve actors outside governments, such as research institutes, private sector actors and nongovernmental organisations (Freiler et al., 2013). In addition, initiatives in line with the HiAP strategy aim at macro-level health determinants and are specifically related to structural or long-term policies or agendas rather than being ad hoc in nature. These features make HiAP initiatives stand out from other intersectoral initiatives.
World Health Organization (WHO) in particular has produced tools and guides to support and highlight the prerequisites for the successful implementation of HiAP (WHO, 2014, 2015). However, the implementation of HiAP is challenging and varies depending on the context in which it is being implemented (Shankardass, Muntaner, et al., 2018; Shankardass, O’Campo, et al., 2018). Successful practices and ways of doing things in one context may not be suitable elsewhere, in which case the previous successful practices do not provide sufficient solutions (Ståhl & Koivusalo, 2020; Van den Broucke, 2013). Therefore, there is a need to increase the understanding of the complex operational environment in which HiAP is to be implemented. In addition, HiAP is also very political, so the focus should not only be on technical implementation but also on politics and political leaders (Cairney et al., 2021; Kokkinen et al., 2017).
The Effects of Political Leadership and Institutional Memory on the Implementation of HiAP
By political leadership in the context of the HiAP strategy, we mean the direct actions of high-level decision makers, such as making detailed plans and objectives, advocating to change the political agenda and creating or redirecting networks (Greer & Lillviss, 2014). Recent findings of Delany et al. (2016) and Guglielmin et al. (2022) suggest that high-level political leadership may influence the chances of implementing the HiAP strategy. However, it is unclear exactly how political leadership improves or hinders the chances of implementing HiAP. A study by Guldbrandsson and Bremberg (2020) in Finland, Norway and Sweden showed that half of the high-ranking civil servants in the 26 different ministries did not recognise the HiAP strategy at all. Thus, we assume that the key influencing mechanism of political leadership is to raise awareness and generate interest in HiAP among other decision makers.
It has been argued that changes in governments can weaken the HiAP approach, even in countries where it has been a long-standing practice (Ståhl & Koivusalo, 2020). Such a situation can be examined through institutional amnesia and institutional memory. Stark and Head (2019) defined the concept of institutional amnesia as those unintentional or intentional ways in which government organisations forget politically relevant experiences of the past. In terms of institutional memory and amnesia, for example, researchers, citizens and other nongovernmental actors have an important role to play in ensuring that decision makers and the organisations that they lead do not forget the failures or successes of the past. Such an active refreshing of the institutional memory might seem to be a problematic slowdown from the point of view of a change-driven decision maker. However, at the same time, it helps to set the boundaries and preconditions for future decision makers so that they would not dismiss, for example, the previous achievements in multisectoral cooperation from the past (Greer & Lillvis, 2014).
The Finnish Context
In Finland, the leading body of health policy is the Ministry of Social Affairs and Health (MSAH), which promotes and guides the HiAP strategy. Interaction and cooperation with international actors, especially with WHO, has been active for several decades, as multisectoral health policies have been promoted through legislation, cooperation structures and different tools (Melkas, 2013). In addition to the MSAH and WHO, the third key body in the implementation of HiAP has been the Advisory Board for Public Health (ABPH). The ABPH consists of separate divisions for multisectoral cooperation at the national level, with 10 ministries out of 13 represented, and local cooperation, representing several municipal and regional actors. In particular, it coordinates and monitors HiAP. Based on this, the Finnish HiAP context can be described from an international perspective as mature (Storm et al., 2014) and well institutionalised (Aaltonen et al., 2018; Kokkinen, Muntaner, et al., 2019).
The Health 2015 public health programme has been the latest public health programme implemented in Finland. It has also been the latest programme to implement the HiAP approach, and thus it is a good example of national strategies and a good opportunity for empirical research on the subject. Health 2015 was a continuation of Finland’s Health for All by the Year 2000 programme, which was fundamentally based on WHO’s Health for All programme. The Health 2015 public health programme was a government resolution managed by the direction of MSAH and prepared by the ABPH at the time. It was formulated as a national cooperation programme from 2001 to 2015 to define Finnish health policy.
Purpose of the Study
This study investigates how and why political leadership and institutional memory affected the implementation of the Health 2015 public health programme in Finland. As the study seeks to explain how and why, it is purposeful to form guiding hypotheses based on previous research. The hypotheses of this study are as follows:
High-level political leadership for HiAP will help raise the interest of other decision makers and prioritise HiAP high enough on the political agenda. Institutional memory enables the continuity of the implementation of the HiAP strategy, and, on the other hand, institutional amnesia can undermine previous success, even in a mature HiAP context.
Data Sources and Methods
Study Design
This study is a realist explanatory case study. The explanation takes place through the causal mechanisms underlying the HiAP implementation, and through the outcomes in the implementation of HiAP under certain circumstances and contexts (Pawson & Tilley, 1997). The context–mechanism–outcome (CMO) configuration is the main heuristic model in the realist approach. The causal mechanisms that produce outcomes in each context are often latent and perhaps difficult to notice, but they are no less real than things that are more easily noticeable. Mechanisms operate at different levels and at different time periods than the outcomes they produce and, in addition, are dependent on the interactions between many different components. Thus, mechanisms have the causal power to influence some outcome, but the ability of mechanisms to produce these outcomes is affected by the context in which they occur (Westhorp, 2018).
Data
This study used the readily available data of key informant interviews, which were part of a larger multiple-case study project of HARMONICS (Kokkinen, Muntaner, et al., 2019). Ethical approval for the HARMONICS project was obtained from the St. Michael’s Hospital Research Ethics Board.
The main data of this study consist of 10 key informant interviews. The interviews were conducted at the end of 2014, and they covered the implementation of the Health 2015 public health programme. Potential key informants were identified on the basis of the literature and by using a snowball sampling strategy. The participants were selected based on their knowledge of the issue and as broadly and comprehensively from different policy sectors as possible. The participants self-assessed their eligibility and familiarity with the topic using a Likert scale. Kokkinen, Muntaner, et al. (2019) described the steps of data collection in more detail.
Five of the key informants represented the health sector and the remaining five represented non-health sectors. Five key informants were high-level civil servants representing different ministries. Three key informants represented research institutes (two directors, one researcher), one key informant was a university professor and one was a politician (a minister at the time of Health 2015). The organisations of the interviewed key informants are in alphabetical order as follows: Finnish Institute for Health and Welfare, HAUS Finnish Institute of Public Management Ltd, Ministry of Economic Affairs and Employment, Ministry of the Environment, Ministry of Finance, Ministry of Social Affairs and Health, Prime Minister’s Office, Tampere University, University of Helsinki and the WHO. Some of the informants represented more than one organisation in their duties.
The interviews were conducted in Finnish using a semi-structured interview framework. The questions were open-ended and based on previously formulated hypotheses. The interviews were led by the following themes: (a) The implementation of HiAP, governance structures and tools; (b) funding allocation; (c) motivation for HiAP; (d) previous expertise and institutional experience with intersectoral cooperation; (e) resistance to cooperation or lack of cooperation and the factors involved with it and (f) influential leadership. The interviews were transcribed word for word, but the tones of voice or other linguistic features were not transcribed.
In addition to the interviews, documentary data were collected. Kokkinen, Muntaner, et al.’s (2019) research report guided the selection of the documents. The documentary data cover the main documents related to the Health 2015 public health programme and, more broadly, to the implementation of HiAP during the implementation period of the Health 2015 public health programme from 2001 to 2015. Based on these criteria, five main documents were selected: (a) Melkas, T. (2013). Health in all policies as a priority in Finnish health policy: A case study on national health policy development; (b) The Ministry of Social Affairs and Health. (2012). Evaluation of Health 2015 public health program [in Finnish]; (c) Ståhl, T., & Rimpelä, A. (Eds.) (2010). Health promotion as a challenge for research and decision-making [in Finnish]; (d) Rotko, T., & Kauppinen, T. (2016). Final evaluation of the Health 2015 public health program [in Finnish]; (e) Vilén, J. (2012). “The patient survived despite the treatment” A study of Finnish health policy and New Public Management. Case: The government resolution on the Health 2015 public health program.
The Process of Data Analysis
The coding and analysis of the data followed the previously developed method of a realistic evaluative case study (Shankardass et al., 2015). The CMO configurations that were found were recorded using the Microsoft Word Comments feature. Line numbers were also recorded so that it would be easier to return to a particular finding later. In the written paragraph of the comment field, the parts where context (C), mechanism (M) and outcome (O) were identified in the transcribed interview were explained in detail to make the conclusions as clear and traceable as possible. Based on the CMO configurations, the relevance or validity of the hypotheses was considered; that is, the hypothesis related to the CMO configuration was either confirmed or questioned.
In addition, CMO configurations were recorded in the Microsoft Excel spreadsheet using line numbers from the transcribed interviews and page numbers from the documents. These line and page numbers were recorded in a table, making it easier to keep track of them. Thus, as the analysis proceeded, it was easier and faster to notice how common a particular hypothesis was, and at what part, and from which key informant, a CMO configuration that either supported or did not support the hypotheses could be found.
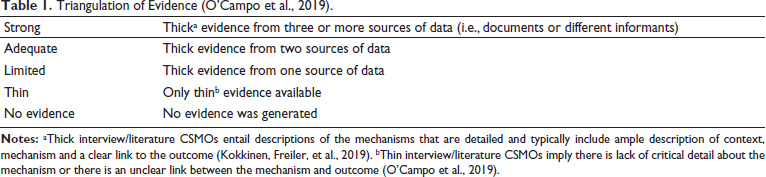
In the final stage of the analysis process, the interview and documentary data were examined together. The purpose of the documents was to apply data triangulation to validate and verify the findings of the interviews. Subsequently, CMO pattern configurations were grouped according to the domains and patterns of similar mechanisms (Shankardass et al., 2015). Tables were created for each domain so that triangulation could be assessed to determine the level of support from multiple sources. Evidence was evaluated for quality based on the triangulation of sources and the strength of the evidence (O’Campo et al., 2019) (Table 1).
Triangulation of Evidence (O’Campo et al., 2019).
Results
Political Leadership
We found strong support for our hypothesis regarding the need for high-level political leadership for the successful implementation of the HiAP strategy (thick evidence from six different sources), and no opposing evidence was found. High-level political leadership, in particular, helps generate interest in the HiAP strategy among other decision makers and prioritises it high enough on the political agenda. As for generating interest, it was considered important for these leaders to show personal interest in the HiAP strategy. The director of a research institute representing the non-health sector described the importance of political leadership for Finland’s prior HiAP success and described how the Health 2015 programme did not have influential advocates who would have created the political will to resource and implement it.
I don’t think that anyone opposed at least, but maybe there haven’t been any clear supporters either. I think that the political side was involved in this to a very small extent in every way. This has been rather civil servant led…—The prior success was a lot about these enthusiastic individuals and strong social democratic/leftist support. Currently the role of Parliament in health policy making is very weak and same applies to political parties.
According to the literature, the civil servant-led promotion of the HiAP strategy has been important in Finland, but not sufficient, as the support of high-level political leaders particularly increases the understanding of different administrative sectors about the importance of health implications and health-oriented actions for other sectors and enables a widely recognised implementation of the HiAP strategy across sectors (Vilén, 2012).
Our hypothesis was further refined so that high-level political leadership in the successful implementation of HiAP is particularly important because of competing priorities within the health sector. We found strong evidence to refine the hypothesis (thick evidence from four sources). The university professor representing the health sector highlighted in this regard the meaning of political leadership in prioritising the reform of the health care system over the Health 2015 programme that implemented the HiAP strategy:
Every time that the government has to discuss health policy, for example in the parliament, with the exception of these few taxation-related issues, the discussion is always related to the healthcare reform and the flaws in health care.—So HiAP simply isn’t the main priority. It may be the second or third priority, but by no means the first priority. In practice, it means that, for example, within the Ministry, and in the National Institute for Health and Welfare, the allotment of priorities and resources doesn’t happen according to this programme, but they have to find a balance with the other priorities.
According to the literature, the prioritisation of curative health care services over health promotion measures in line with the HiAP strategy has been further facilitated not only by political leadership but also by legislation that is less binding to health promotion than to health care services (Melkas, 2013).
Institutional Memory
We found strong support for our hypothesis on the role of institutional memory in the successful implementation of the HiAP strategy (thick evidence from 10 different sources) and only weak evidence opposing it (thin evidence from one source). According to our analysis, in the twenty-first century, there has been an institutional amnesia in Finland that came along with the transition to project-based HiAP implementation. Contrary to previous good experiences, the Health 2015 programme, like many other government programmes and development projects in the twenty-first century, has been project based not only in terms of its actions but also in terms of its resources. We found that well-established and good practices would have been needed alongside such project-based work. This could dispel concerns and doubts about the continuity of actions and resources beyond the end of the project, and thus lead to sustainable and longer-term implementation. A researcher representing the health sector described how the institutional implementation structure of the Finnish HiAP strategy simply disintegrated with the transition to a project-based world.
To summarise, the most significant change has been that the implementation structure disintegrated and has been increasingly replaced by project-based activities. What has been typical for these activities is short-term funding. We sort of still have a system of working groups and national action plans, there’s been programmes on alcohol policy and tobacco policy, but their implementation, there’s no implementation structure.
In addition to the transition to project-based implementation, the reform of the state subsidy system in 1993 in Finland drove institutional amnesia by dismantling the state’s financial control over the municipalities, on which Finland’s previous success in implementing national strategies at the municipal level was largely based. After the state subsidy reform, the government began to learn how to guide municipalities with information instead of financial steering. A researcher representing the health sector accurately pointed out the trigger for institutional amnesia in this regard: ‘And the decisive decision was made in 1993, with the dismantling of the regulatory system’. The third factor alongside project-based implementation and the state subsidy reform that drove institutional amnesia in Finland was the generational change in MSAH in the 2000s and 2010s. Although new talented and pro-development-oriented civil servants were found in senior positions in the ministry, they did not have the long experience of their predecessors or the long-term personal relationships with other ministries to implement the HiAP strategy.
Discussion
This study examined how political leadership and institutional memory affected the implementation of the HiAP strategy. Based on the results, high-level political leadership for the HiAP strategy can help generate interest among other decision makers and prioritise the strategy high enough on the political agenda. This is particularly important for competing priorities. Institutional memory, on the other hand, enables continuity in the implementation of HiAP, and the results of this study suggest that institutional amnesia might undermine prior success, even in a mature HiAP context.
In terms of political leadership, we found shortcomings in the Finnish context. Shortcomings were also identified in the health sector’s own policies and actions. The HiAP strategy did not have a strong leader during the Health 2015 programme in 2001–2015, who could have generated interest in HiAP among other decision makers. The high-level political and civil servant leaders who had previously promoted the implementation of HiAP in Finland left a gap when they left office, which has made the implementation more difficult and partly fully hindered. According to this study, there have previously been strong leaders in Finland, and the difference between the current state of the HiAP strategy and the past is evident in the absence of such strong leaders.
In terms of institutional memory, we found institutional amnesia in Finland. During the implementation of Health 2015, the state administration shifted to project-based implementation, many long-term and high-level civil servants retired from MSAH, and steering the municipalities shifted from financial steering to steering by information. This was followed by discontinuity in the Finnish HiAP implementation and in the prior rather institutionalised implementation structure. Several well-established practices that helped in everyday work, such as intersectoral working groups, procedures and the distribution of work and assignments, disappeared.
In Finland, the government resolution on the ‘Promotion of wellbeing, health and safety 2030’ (Finnish Government, 2021a) and the related implementation plan prepared by the Advisory Board for Public Health (Finnish Government, 2021b) continues the work towards the long-term goals set in the Health 2015 public health programme. The government resolution and the implementation plan strongly emphasise the role of the HiAP strategy. Understanding and explaining previous implementation experiences during the Health 2015 public health programme provides better opportunities to consider the preconditions for successful implementation in the future.
The results of this study also provide lessons on the impacts of political leadership and institutional memory on the implementation of the HiAP strategy beyond the Finnish context. Our research deepens the understanding of why the mere rhetoric or principled support of political leaders is not enough and does not lead to success in implementing the HiAP strategy; instead, successful implementation requires concrete actions, as has been called for in previous research (Melkas, 2013; Rotko & Kauppinen, 2016; Vilén, 2012). In addition, although Finland has often been described as a forerunner in the HiAP strategy (Guglielmin et al., 2022; 2023; Melkas, 2013), based on this study, there is no reason to rely on this old success. Considering this study, the implementation of HiAP after the institutional amnesia appears to be project based, largely dependent on single individuals within the government system, and is only recently getting used to the era of steering by information.
Based on their recent literature review, Cairney et al. (2021) called for an increased realistic and comprehensive understanding of politics, power and political processes in the implementation of HiAP. They state that utilising the perspectives and theories of political science could help broaden the understanding of the implementation of HiAP, although it should not be used as a technical tool or manual to solve problems, but instead should provide critical reflection tools for understanding and adapting to different contexts. In this study, we examined two theoretically strong factors that explain the implementation of HiAP—political leadership and institutional memory—in the Finnish context. For this part, we have increased the understanding of why there is a gap between the HiAP principle and its practical implementation, and why this gap also varies in a mature HiAP context.
Strengths and Weaknesses of the Study
The strength of our study, based on the realist explanatory case study method, is the ability to analyse how different factors affect the implementation of HiAP strategy in a certain context (Shankardass et al., 2015). To explain how political leadership and institutional memory affected HiAP implementation in the Finnish context, we used the CMO configurations based on our hypotheses. The reliability of the results in this study is increased by the fact that we used two types of research data: interviews and documents. Through data triangulation, it was possible to confirm the evidence and accuracy of the findings from the interviews and the literature.
On the other hand, however, context dependence can also be considered the biggest weakness of this study. The data and methods used enabled the analysis of the effects of political leadership and institutional memory precisely in the Finnish context, and the results of this study may not be directly generalisable to other countries.
We employed several strategies to prevent and acknowledge confirmation bias in our study. We sought out evidence from diverse sources (i.e., documents and different informants) and systematically employed data triangulation to ensure that all relevant evidence was considered. In addition, according to the methods and processes of realist explanatory case studies, we observed and sought evidence that both supported and refuted our hypotheses. This systematised methodology and the training for realistic methods both authors had undergone, increased our awareness of confirmation bias in general, in addition to the objectivity provided through seeking out alternative explanations for our findings. The findings of our study were reviewed and reflected accordingly with a separate, experienced external researcher, to reduce the influence of preconceptions on the evaluation of the data. However, to some extent, there is a possibility for confirmation bias despite our efforts to address and avoid it.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.