
Abstract
The ongoing pandemic of the novel coronavirus (COVID-19) has exploded and raised important questions on the efficiency and effectiveness of healthcare systems around the world to provide guidance for appropriate policy responses. While it is important to look at the current (and future) situation, it is also needed to look back into the past, especially at the first few months of the pandemic. This study re-examines the efficiency of healthcare systems around the world against the outbreak of COVID-19 in its first 62 days (23 January 2020–25 March 2020) to see if the examined countries were well prepared and well reacted to the pandemic. Results from a data envelopment analysis evaluation indicated that the global healthcare systems experienced a very low efficiency on average. Besides the absence of a coronavirus vaccine at that time, this low efficiency is typically linked to the operational scale of the healthcare systems, suggesting that countries could tightly rationalise their healthcare resources/inputs to improve the technical efficiency of their healthcare systems.
Introduction
The ongoing pandemic of COVID-19 has exploded and raised important questions on the efficiency and effectiveness of healthcare systems around the world. Public health, politics and medical communities are struggling with the strain of medical staff, equipment and supplies (Fauci et al., 2020; McCloskey & Heymann, 2020). The importance of the healthcare systems, especially during such pandemic, was emphasised by researchers, practitioners and philanthropists (Gates, 2020; Gilbert et al., 2020; Hick & Biddinger, 2020; Prakash Narain et al., 2021).
Countries such as Italy, France, India, Brazil, the United Kingdom and the United States have witnessed major surges of patients, which posed critical problems in levelling the demand for intensive care units (ICU) and medical staff. The lessons from the Ebola outbreak in Guinea, Liberia and Sierra Leone (Parpia et al., 2016) or the recent experiences from South Korea in containing COVID-19 (Tang et al., 2020) proved that accessibility to healthcare services would significantly help reduce the number of deaths.
Given the widespread impacts of the COVID-19 pandemic on the global economy and society (Narain et al., 2020), it is ultimately important to assess the efficiency of healthcare systems around the world in order to provide guidance for appropriate policy responses, especially looking back at the early stage of the pandemic as of January–March 2020 (Gupta et al., 2020). We re-examine this situation using the data envelopment analysis (DEA) approach and a comprehensive data set of more than 100 healthcare systems combined from different sources (Dong et al., 2020; Mayer & Zignago, 2011; The World Bank, 2020; WHO, 2020b). Although healthcare is the second-most popular sector for DEA applications (Liu et al., 2013), most of them focused on hospitals (Hollingsworth, 2003; Kohl et al., 2019; Sikka et al., 2009) and DEA studies on healthcare systems worldwide are still limited. For example, Ozcan (2014) only notices two studies, while Kim and Kang (2014) document 10 studies that examine the OECD and other cross-country healthcare systems. Although the choice of inputs is similar among those studies, the outputs selection varies due to the research purposes. For example, when examining the efficiency in delivery healthcare services to the population, Bhat (2005) used the number of populations aged 0–19 years, 20–64 and 65 or older as outputs. In contrast, Santos et al. (2012) used the number of pregnant women tested for HIV and the number of HIV pregnant women receiving antiretrovirals, among others, as outputs for their DEA model to examine the efficiency of countries in preventing the mother-to-child HIV transmission. Consequently, new DEA studies for new settings such as the recent COVID-19 outbreak may need to introduce new output(s), depending on the research purpose.
Methods
DEA with Bad/Undesirable Outputs
The basic idea behind the DEA is to envelop a best practice frontier from all observed decision making units (DMUs) where a DMU is technically efficient if it lies on this frontier while inefficient DMUs lie under the frontier (Ngo & Le, 2019). Since DEA can deal with multiple inputs and outputs at the same time without the need for a priori production function (Flokou et al., 2017), it can be straightforwardly applicable to the healthcare sector where the definition of such function is complex.
To analyse the healthcare system at the aggregate level, we follow Häkkinen and Joumard (2007), Joumard et al. (2008), OECD (2010) and de Cos and Moral-Benito (2014), among others, to treat the whole healthcare system in a given country as a DMU. Since there are differences between the examined countries (e.g., income levels or sizes), we employ the variable returns to scale (VRS) assumption in our analysis, instead of the constant returns to scale (CRS) one. Due to data limitation, especially at the aggregate level, we choose our input variables following the healthcare efficiency literature, while new outputs are introduced to capture the COVID-19 situation.
Three main inputs of hospitals are capital, labour and operating expenses (Kohl et al., 2019)—we therefore look at the aggregated numbers at national level to get the inputs of the healthcare system. That is, we use the total number of hospital beds (Beds), the total number of physicians and nurses (Labour) and the total health expenditure (Expense) as our inputs. Previous studies on healthcare systems (Behr & Theune, 2017; Joumard et al., 2008; Kim & Kang, 2014; OECD, 2010) also use those inputs in their DEA models.
We then look at the expected outputs of a healthcare system regarding the COVID-19 issue. There is evidence that the number of recovered cases better reflects the true output of the healthcare system instead of the number of treated cases (Kohl et al., 2019; Maniadakis et al., 1999). Additionally, the absence of the COVID-19 vaccines in early 2020 led to the argument that preventing the spread and reducing the number of infested cases were most important (Kaplan, 2020). To the extent that the number of confirmed cases and especially the number of deaths are exponentially increasing every day during the early state of the COVID-19 pandemic (Dong et al., 2020; MacIntyre, 2020; WHO, 2020a), it is essential to examine if the healthcare system can help increase the number of recovered cases (Recovered Cases) as well as to reduce the number of deaths (Deaths) and infected cases (Infected Cases).
Note that among those outputs, the smaller Infected Cases and Deaths the better, given that the healthcare system using the same amount of inputs. Traditional DEA is unsuitable to handle these two variables; we therefore follow Cooper et al. (2006) and treat those two numbers as bad/undesirable outputs, while Recovered Cases is a desirable one. In this sense, we extend the DEA literature on the efficiency of healthcare systems not only in terms of the COVID-19 situation but also in terms of using undesirable outputs in our DEA model. As such, our study evaluates the healthcare systems in terms of using three physical and financial inputs (i.e., Beds, Labour and Expense) to produce one desirable output (i.e., Recovered Cases) and two undesirable outputs (i.e., Infected Cases and Deaths). Consequently, healthcare systems that can produce more desirable outputs and less undesirable outputs relative to less input resources are recognised as efficient.
Formally, let us consider the production possibility set defined by:

where X denotes the input matrices; Yg and Yb denote good (desirable) and bad (undesirable) outputs matrices, respectively; λ is the intensity vector; and L and U are the lower and upper bounds of the intensity vector, respectively.
Following Cooper et al. (2006), the CRS technical efficiency of DMU (
subject to





where s− and sb are the vectors of excesses in inputs and bad outputs, respectively; sg expresses shortages in good output; s1 and s2 denote the number of elements in sg and sb, in our case s1 = 1 and s2 = 2. Note that if CRSTE = 1 then the DMU is said to be fully efficient.
The VRSTE efficiency scores are estimated similar to the CRSTE ones but by adding the following constraint to Equation (2):

Data
Our data are gathered from different sources. The COVID-19-related data (i.e., infected cases, recovered cases and deaths) are extracted from the live update database provided by the Center for Systems Science and Engineering at Johns Hopkins University (Dong et al., 2020). For the first 62 days of the pandemic, from 23 January 2020 to 25 March 2020, this database covers the COVID-19 updates for 181 countries and territories all over the world. Regarding the aggregated data on beds, labour and expense, they are obtained from the World Development Indicators (WDI) provided by The World Bank (2020). After matching those data and removing missing information, we ended up using 105 countries in our analysis. The full list of countries is provided in the Appendix.
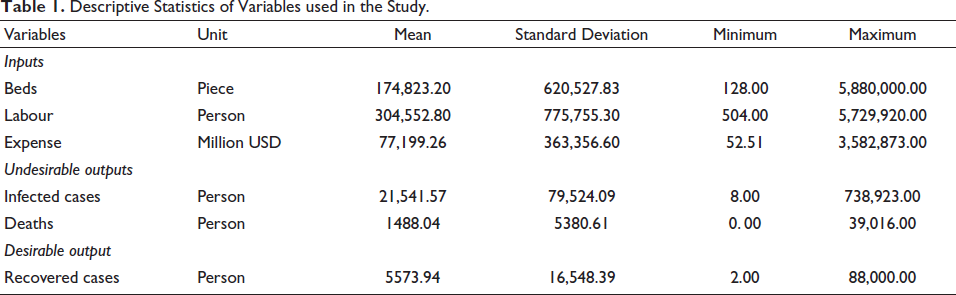
Some descriptive statistics of those variables are reported in Table 1 indicate that our sample countries have, on average, a resource of nearly 175,000 beds, more than 300,000 physicians and nurses, and a budget of about $77,000 million for its healthcare system. The number of infected cases and deaths from COVID-19 over the study period averaged more than 21,000 and nearly 1,500, respectively; but averagely only about 5,500 persons were recovered from the disease. A simple comparison between labour and recovered cases, for example, shows that it took around 55 physicians and nurses just to help one patient to recover, assuming that the whole healthcare system is mobilised to fight the novel coronavirus outbreak. The question is, is this mobilisation efficient?
Descriptive Statistics of Variables used in the Study.
Results and Discussions
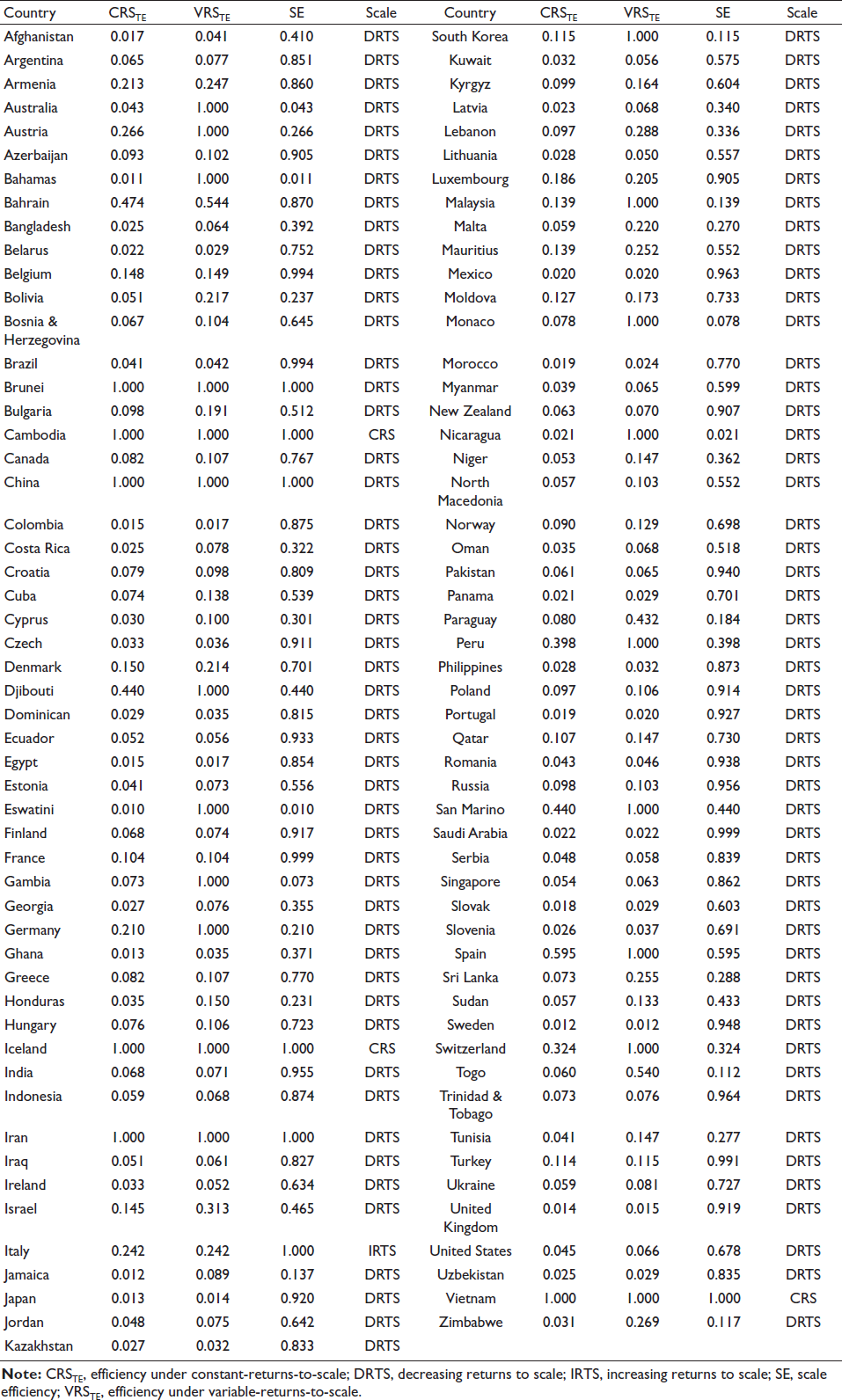
We report, in Figure 1, the graphical and descriptive results regarding efficiency of the world’s healthcare systems against COVID-19. We observe the mean values of CRSTE (efficiency under CRS assumption) and VRSTE (efficiency under VRS assumption) are only 0.140 and 0.290, respectively. Both measures are skewed towards lower efficiency score values (see Figure 1 and Appendix). This finding unfortunately suggests that the mobilisation of healthcare systems is not very efficient against COVID-19, given the physical and financial resources used.
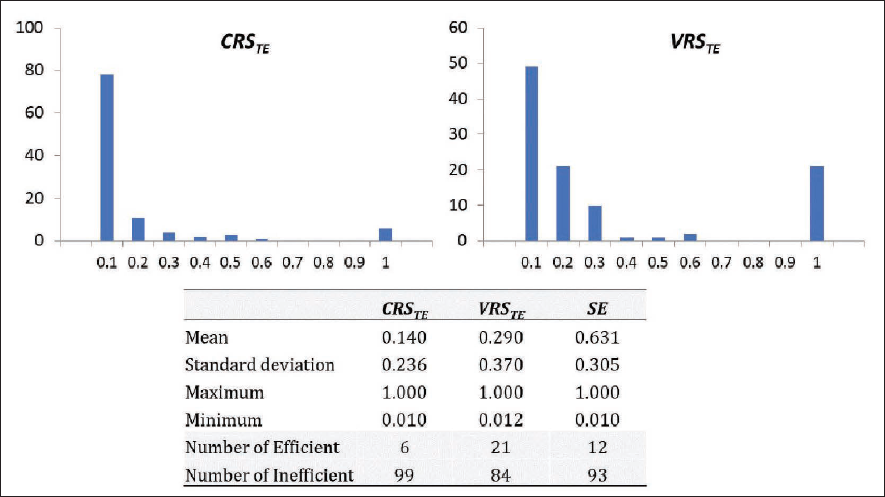
Under the CRS assumption, there were only six efficient healthcare systems in dealing with COVID-19 including Brunei, Cambodia, China, Iceland, Iran and Vietnam. When the VRS assumption is considered, as expected, this figure jumps to 21 with the addition of Australia, Austria, Bahamas, Djibouti, Eswatini, Gambia, Germany, Korea, Malaysia, Nicaragua, Monaco, Peru, San Marino, Spain and Switzerland (see Appendix). These differences, regarding the full sample of 105 countries, are statistically significant under a Mann–Whitney–Wilcoxon’s test (Z = 5.271, p = .001). It indicates the role of SE in our analysis because the global healthcare systems are doing their best in terms of the technical combination of the inputs to produce the outputs, but their scales (sizes) are not optimal yet. Particularly, 101 out of 105 countries are experiencing the decreasing returns to scale problem (see Appendix), suggesting that they can double the inputs used but the outputs will not be doubled. For this reason, these countries could tightly rationalise their healthcare resources/inputs towards downsizing and thereby improve the technical efficiency, while the outputs still stay the same.
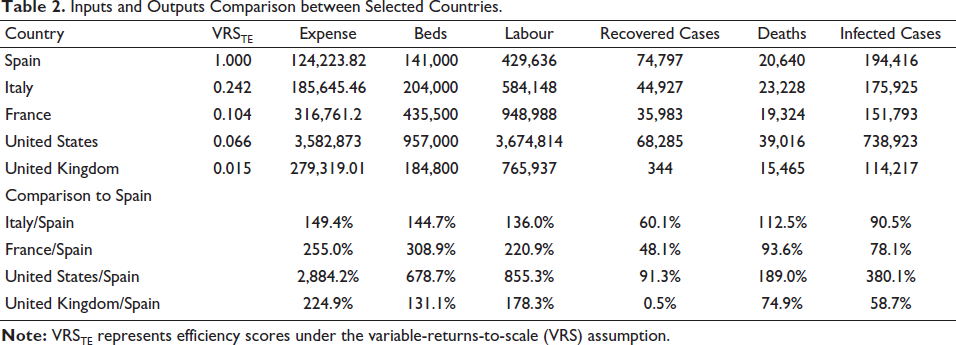
On the other hand, the VRS results show Spain among the top performers, despite its high number of deaths due to COVID-19. A comparison among countries with high deaths can help us understand the reason behind their associated DEA efficiency scores. Table 2 reports the differences in inputs used, outputs achieved and the resulting efficiency of some selected healthcare systems. For example, in comparison to Spain, the United States has nearly 30 times of expense, seven times of beds and nine times of labour higher; however, it did not success in monitoring its bad outputs (i.e., nearly four and two times higher in terms of infected cases and deaths, respectively) as well as the good output (with less recovered cases). This result clearly explains the relatively low VRS technical efficiency scores of the United States or the United Kingdom, which could be linked to specific policy responses of selected countries. For example, there is now evidence to suggest that the United Kingdom failed to fight the COVID-19 outbreak while following a ‘herd immunity’ approach (Stewart et al., 2020) or the United States has been very slow to act against COVID-19 (Watts, 2020).
Inputs and Outputs Comparison between Selected Countries.
Conclusions and Implications
This article examined the efficiency of 105 healthcare systems against the current COVID-19 pandemic in its early stage as of March 2020, particularly 62 days after the pandemic was announced in 23 January 2020, given their resources constraints, to see if the global healthcare system was well prepared and well reacted to the pandemic. Using an alternative DEA approach which accounts for both desirable outputs (number of recovered cases) and undesirable outputs (infected cases and deaths), we show that the average efficiency of the global healthcare systems against COVID-19 was very low, with only six efficient systems under CRS assumption and 21 efficient systems under VRS assumption. This finding suggests that without changes in the sizes of their healthcare systems, most of sample countries could not improve their efficiency, despite increases in the resources because the latter are currently wasted or inefficient. Future research can extend our study while considering more variables when they become available to gauge the heterogeneity of policy effectiveness across countries.
Appendix A. Efficiency of the Global Healthcare Systems against COVID-19.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.