
Abstract
The child mortality rate is an important indicator presenting crucial information about the health status of a country. In the current study, we examined whether health care utilisation reduced the under-5 mortality rates, an important health status indicator, in Turkey. We employed an autoregressive distributed lag bounds test. We used doctor consultation and health expenditure as the independent variables. We found out that both doctor consultation and health expenditure had negative impacts on the under-5 mortality rates in the short run; however, the effects of both variables were not statistically significant (p > .05). Also, we showed that while the effect of doctor consultation on the under-5 mortality rates was negatively and statistically significant (p < .05) in the long run, the effect of health expenditure was not statistically significant (p > .05). Turkey should allocate more to health care services specifically targeting infant and child health to reduce its infant and child mortality rates.
Introduction
Welfare and good health status and their determinants have gained a longstanding interest among both academics and policymakers. As people and communities are changing constantly, namely they are dynamic, what to be understood from the terms of welfare and good health status has been changing constantly too. Although the perception of welfare and good health status has been in a change, and, as a result of this change, its determinants have been changing. We can categorise the determinants of the perception of welfare and good health status such as social and economic environment, physical environment, individual characteristics and behaviours and health care services (WHO, 1998; WHO, 2013).
Among the categories mentioned above, health care services and utilisation of them are important to increase the welfare and health status in a society. Although the weight of health care services among the factors affecting the welfare and good health status is the subject of debate (Hurley, 2000; Thornton, 2002), their impacts on the welfare and good health status are undeniable facts (Alpugan, 1984). In countries where health care services are not provided in sufficient quantity and at high quality, life expectancy at birth is quite low and age-related mortality rates are quite high (OECD, 2020). Health care services are among the sine qua non of the welfare and good health of societies. However, there are some countries where the health status indicators are low even though health care services are delivered in sufficient quantity and at high quality. Among these countries, the USA is one of the most coming up with. Health expenditure per capita in the USA is relatively high compared to the other developed countries, but many health status indicators in the USA are lower than many other developed countries (McGovern et al., 2014). This raises the question of whether health care services are being delivered effectively.
In the current study, we investigated the effectiveness of health care services in Turkey. We examined whether health care utilisation reduced the under-5 mortality rates, an important health status indicator, in Turkey using autoregressive distributed lag (ARDL) bounds test.
Literature Review
ARDL is a popular time-series approach to reveal the effects of independent variables on the dependent variable in health care services. Mehrara (2011) examined the relationship between health expenditure and health status in Iran for the time period of 1970–2007 based on the ARDL approach and revealed that health care expenditures are among the most important factors in the lowering of infant mortality.
Khandelwal (2015) investigated the impact of energy consumption, fiscal deficit and gross domestic product on public health expenditure in India for the time period of 1971–2011 with the help of ARDL. The author revealed that there was a long-run causal relationship between energy consumption, fiscal deficit, gross domestic product and public health expenditure, while in the short run, only gross domestic product was found to be significantly causally related to health expenditure.
Abdullah et al. (2016) used the ARDL approach to examine the cointegration between environmental quality and socio-economic factor for national health expenditure in Malaysia. They indicated that sulphur dioxide, fertility and infant mortality rate showed a significant factor in the country’s health expenditures.
Ahmad and Hasan (2016) revealed the impact of public health expenditure and governance on health outcomes via ARDL by using the data from 1984 to 2009 in Malaysia, and they found out that public health expenditure positively and significantly affected life expectancy in the long run.
Murthy and Okunade (2016) examined the determinants of health expenditure in the USA by using 1960–2012 annual time-series data and found out that per capita real income, the population percentage above 65 years and the level of health care technology exert had positive effects on the health expenditure per capita.
Zaidi and Saidi (2018) evaluated the relationship between health expenditure, carbon dioxide and nitrous oxide emissions and economic growth in the sub-Saharan African countries using a panel ARDL modelling based on the time period of 1990–2015. They indicated that economic growth had a positive impact on health expenditure while carbon dioxide and nitrous oxide emissions had negative impacts on health expenditure in the long run.
Akingba et al. (2018) showed that health expenditure per capita positively and significantly affected Singapore’s economic growth in the long run when they adopted the data covering the period 1980–2013 and ARDL as the method.
Nguyen et al. (2019) examined the long-run and short-run impacts of population ageing and income on health expenditure in Vietnam for the time period of 1990–2017 by employing the ARDL approach and found out that there were stable effects of population ageing and income on health expenditure in the short and long run.
Hadiza and Yahaya (2019) conducted a study using the ARDL approach to determine the impact of total population and health expenditure on HIV/AIDS in Nigeria from 1990 to 2018. According to the results of this study, total population and health expenditure had a positive and significant impact on HIV.
Shahzad et al. (2020) used ARDL to explore the dynamic relationships between health expenditure, economic growth, carbon dioxide emission, information and communication technology and renewable energy consumption in Pakistan. They employed the data from the time period of 1995–2017 and found out that economic growth and carbon dioxide emission had a positive impact on health expenditure while information and communication technology and renewable energy consumption had a negative impact on health expenditure.
Imandojemu et al. (2020) used the ARDL approach while they were evaluating the determinants of Human Capital Development Index in Nigeria for the time period of 1990–2018. They showed that the relationship between government expenditure on education and health and life expectancy on Human Capital Development Index was positive and significant while the relationship between fertility rate and human capital development was negative and significant.
Hayat et al. (2020) aimed to test the hypotheses of the modernisation theory and the social-democratic theory related to child mortality in Pakistan via ARDL by using the data belonging to the time period of 1972–2014. They found out that gross domestic product per capita was a significant variable responsible for the decline in child mortality.
Methods
Variables and Data Source
In view of our aim to reveal the effects of doctor consultation (dc), as the number per capita, and health expenditure (hex), as $ per capita by purchasing power parity, on the under-5 mortality rates (u-5m), per 1,000 live births, in Turkey, we used the annual data of Turkey for the time period of 1973–2016 (i.e., 44 years). The data on dc and hex were taken from the health database of the OECD (2020), and the data on u-5m were taken from the health database of the World Bank (2020). We took the natural logarithms (log) of the variables and obtained Log(u-5m), Log(dc) and Log(hex).
Analysis
We employed ARDL bounds testing approach in the current study. ARDL bounds testing is a widely used approach to measure long- and short-run effects of independent variables on the dependent variable. This model was introduced by Pesaran et al. (2001). In this model, the series should integrate at the order I(0), namely at the level and/or I(1), namely at the first difference.
If different variables have different orders of integration in a study, the ARDL can be used. As a result of this advantage of ARDL, this approach has become widely used because other cointegration techniques such as Johansen (1988) and Engle and Granger (1987) cointegration tests cannot be used in cases when different variables have different orders of integration (Khandelwal, 2015). Although our variables are integrated in the same order, we used ARDL because it can work in cases when other cointegration tests cannot work due to the limited number of observations, which is another advantage of ARDL (Tang, 2003).
In a typical ARDL model, firstly, long-run cointegration is tested with the help of an F-statistics-based bound test. The null hypothesis in this test is that there is no cointegration among the variables while the alternative hypothesis is that there is cointegration among the variables. if the alternative hypothesis is accepted, then the short-run and the long-run results are presented separately. The ARDL uses the Error Correction Model (ECM) to obtain the short-run results, and the error correction term with lag (ECT(–1)) in the ECM should be negative and statistically significant (Anand et al. 2019).
We used some diagnostic and stability tests to reveal the goodness of our model. These tests have tested whether there was a serial correlation, heteroscedasticity, model specification error and normality related problems. We employed CUSUM and CUSUM of squares (CUSUM-SQ) tests for the stability of the model.
The ARDL bounds testing approach requires an appropriate lag determination before the analysis (Baharin & Saad, 2017). In our study, we determined the optimal number of lags by benefiting from the information criteria values of Vector Autoregressive (VAR) model. Based on the results, the optimal lag length for our ARDL model was determined as Lag 2 because it was the most preferred lag length by Akaike information criterion (AIC), Schwarz information criterion (SC) and Hannan-Quinn information criterion (HQ). The data were analyzed with the support of EViews 10.0 software and the results were interpreted at the 5% significance level.
Findings
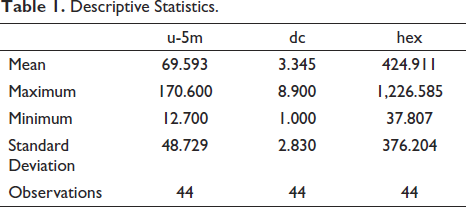
We, first, presented the descriptive statistics of the variables in the study. Table 1 shows that the mean values of u-5m, dc and hex were 69.593 ± 48.729, 3.345 ± 2.830 and 424.911 ± 376.204, respectively. The variable of u-5m had values between 170.600–12.700, the variable of dc had values between 8.900–1.000 and finally, hex had values between 1,226.585–37.807.
Descriptive Statistics.
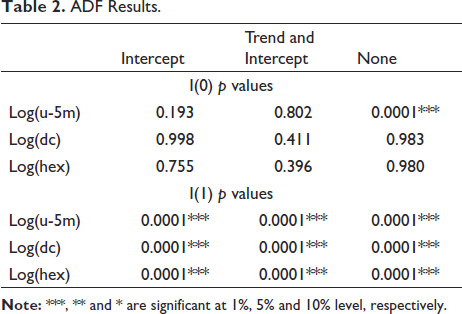
In ARDL bounds testing, the stationarity of the variables is important, and this can be checked by some unit root tests. In the current study, we employed Augmented Dickey-Fuller (ADF) unit root test, whose null hypothesis is that there is a unit root in the variable. Table 2 presents the p values of the variables in ADF unit root test. After examining the Table 2, we can conclude that all of our variables become stationary at the first difference and our variables are integrated at first order (I(1)).
ADF Results.
We used a VAR model to determine the optimal lag length of the ARDL. Table 3 presents the VAR results. According to the results, the most selected lag length among AIC, SC and HQ was 2, and therefore, we determined the optimal lag length as 2.
VAR Results.
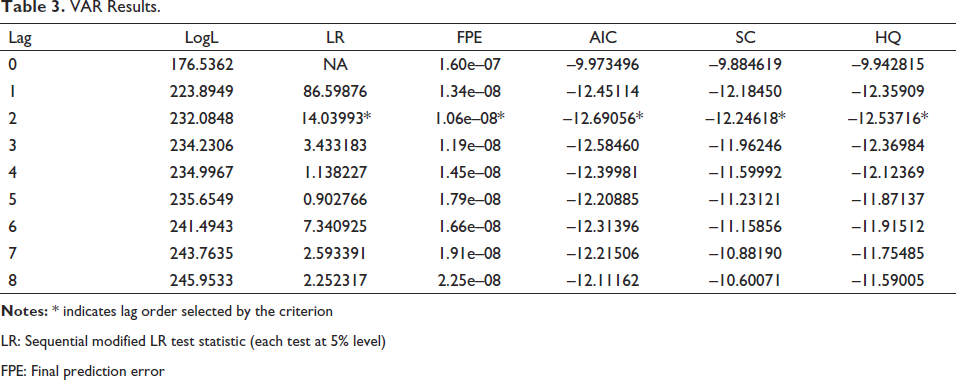
LR: Sequential modified LR test statistic (each test at 5% level)
FPE: Final prediction error
We can see the results of F-statistics-based bound test in Table 4. According to Table 4, the F-statistic value (7.88) was higher than the upper bound at both 5% (3.86) and 1% (5.00), and therefore, we accepted that there was a long-term relationship among our variables.
Bound Test.

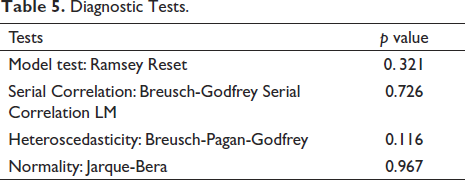
We employed Ramsey Reset, Breusch-Godfrey Serial Correlation LM, Breusch-Pagan-Godfrey and Jarque-Bera tests to reveal whether our model had model specification error, serial correlation, heteroscedasticity and normality-related problems. The results are presented in Table 5. According to the results of these tests, we concluded that our model did not include any problems mentioned above (p > .05).
Diagnostic Tests.
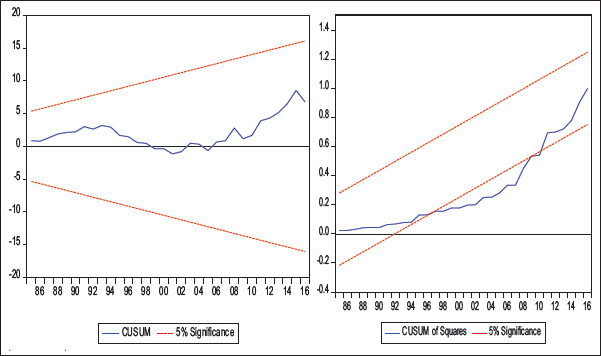
We also tested the stability of our model and employed CUSUM and CUSUM-SQ (Figure 1). When we examine Figure 1, we can see that our model is stable according to the CUSUM and shows a slight deviation according to the CUSUM-SQ. We decided that this slight deviation did not deteriorate the stability of the model because it was again in the confidence level as Yakışık and Çetin (2014) stated.
Stability Tests.
We presented our model’s long-run results in Table 6. As shown in Table 6, the estimated coefficients of dc and hex had expected signs in the long run because both the variables had negative signs, and these variables were expected to lower the u-5m. However, while the effect of dc on u-5m was statistically significant (p < .05), the effect of hex was not statistically significant in the long run (p > .05).
Long Run Results.

In the short run, both dc and hex had negative impacts on the u-5m; however, the effects of both variables were not statistically significant (p > .05; see Table 7). The coefficient of ECT (–1) (–0.127222) was significant and showed that about 12% deviation of u-5m from its long-run level was adjusted in one year, meaning that u-5m had an unstable behaviour in Turkey.
Short Run Results.

Discussion and Conclusion
We examined the effectiveness of health care services in Turkey in the current study. We found out that doctor consultation and health expenditure, both are important health care utilisation indicators, had negative and insignificant impacts on the under-5 mortality rates in the short run. However, we found out that the effect of doctor consultation on the under-5 mortality rates was negative and significant in the long run. This is an expected case because the impacts of health care service utilisation can be felt in long run. The outcomes of increasing health resources in a country can be observed in the long run because health care services sector is not a sector where the feedback of new investments can be measured in a short run.
There are some studies supporting our findings. For example, Imandojemu et al. (2020) indicated that government expenditure on health positively affected Human Capital Development Index, which includes under-5 mortality rates as an indicator for the survival component. Ahmad and Hasan (2016) also found out that public health expenditure positively and significantly affected life expectancy in the long run. Hayat et al. (2020) showed that an increase in gross domestic product per capita, an important determinant of health expenditure, might reduce the child mortality. Contrary to these studies, Hadiza and Yahaya (2019) found out that health expenditure had a positive and significant impact on HIV unexpectedly. This finding can be explained with the view that spending more on health care services especially on diagnosis tests naturally enable health professionals to detect more HIV cases, and, as a result of this, health expenditure for diagnosis tests may increase HIV cases. Also, the relationship between health expenditure and HIV cases may be bidirectional, namely health expenditure may increase as a result of an increase in HIV cases because people with HIV are required to receive more medical treatment.
Health care utilisation is crucial to reducing mortality rates and increase health status in a society. In this regard, governments have important duties. They are responsible for the allocation of the sources in health care services; therefore, they should give importance to infant and child health care services, especially preventive health care services for infants and children. Families have also important responsibilities because they usually decide on behalf of their infants and children. They should take care of their babies’ and children’s vaccination. Recently, opposition to vaccination among families with infants and/or children has been increasing in Turkey. Vaccination is important for babies and children to grow up healthy and live a healthy life in the future. For this reason, educational activities should be organised to inform families that the vaccine is not harmful to their babies and children but is very beneficial.
Infant and child mortality are important health status indicators; therefore, both underdeveloped and developing countries are trying to improve their infant and child mortality rates. As a developing country, Turkey has also taken some important measures to reduce infant and child mortality rates. Although Turkey has decreased its infant and child mortality rates since 2000, these mortality rates are still high in Turkey. Turkey should allocate more to health care services specifically targeting infant and child health to reduce its infant and child mortality rates.
Limitations
This study has some limitations. First, gross domestic per capita was overly correlated with health expenditure per capita; therefore, we could not use gross domestic per capita even though we wanted to include it in our ARDL model. Second, we wanted to use at least one variable presenting information about Turkey’s educational status, but we could not reach any data regarding education for the time period which the study covered. Finally, we also wanted to use an indicator regarding vaccination in Turkey; however, we could not obtain the data for all the years covered by the study.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Informed Consent
Not applicable.
Funding
The author received no financial support for the research, authorship and/or publication of this article.