
Abstract
This article seeks to investigate the relationship between the per capita income of countries and the deaths resulting from COVID-19 per million inhabitants. For this, information from the twenty-eighth of June 2021 is considered for 186 countries, comprising the five continents. Using the ordinary least squares linear regression technique and data on GDP per capita, human development index, percentage of population with two doses of vaccine, deaths from COVID-19 per million inhabitants, available tests per capita, percentage of population with diabetes, hospital beds available per capita, percentage of the population over 70 years old, population density, democracy index and Gini coefficient, the results show that the countries most vulnerable to the pandemic are those classified as upper-middle-income, with per capita income. Capita, proportion of elderly people and democracy index significantly impact deaths per million inhabitants.
Introduction
The new coronavirus is a disease popularly known as COVID-19 and was discovered in December 2019 in the city of Wuhan, China. Caused by severe acute respiratory syndrome coronavirus 2 (Sars-Cov-2), COVID-19 quickly spread across the globe, resulting in a pandemic that was declared by the World Health Organisation on the day 11 March 2020 (Oba et al., 2020). According to Pak et al. (2020), the new coronavirus has not only caused a public health crisis but also the world economy has suffered a major impact that has led to declines in productivity, loss of life, business closures, trade disruption and deterioration in the tourism sector.
Although the outbreak of the new coronavirus supposedly started from a zoonotic transmission event associated with a large seafood market that also traded live wild animals, it soon became evident that efficient human-to-people transmission also occurred (Zhang, W. et al., 2020). The clinical picture of most people who contract COVID-19 will develop only a mild to moderate respiratory disease and will be able to recover without the need for any medical treatment (Zhang, J. J. et al., 2020).
However, elderly people and individuals with pre-existing medical problems, such as cardiovascular disease, diabetes, chronic respiratory diseases and cancer, are more likely to develop a more severe degree if infected with COVID-19, requiring some medical intervention (Jordan et al., 2020; Huang et al., 2020). Based on the literature, this disease is also associated with some complications such as thromboembolism, acute myocarditis, rhabdomyolysis, renal failure, multiple organ failure, encephalopathy and heart failure (Shahbazi & Khazaei, 2020).
In order to try to contain the advance of the new coronavirus, many governments of different nations are applying containment and mitigation policies to delay the large outbreaks of infected patients in order to reduce the demand for hospital beds, while protecting the most vulnerable people from infection, which include the elderly and individuals with some comorbidity. Most of the strategies used by countries include contact tracking, quarantine of infected people and promotion of public health measures that boil down to hand washing, mask use and social distancing (Bedford et al., 2020).
However, for these measures to be applied efficiently, countries need to impose rules for the population to obey and have public compliance on the importance of preventing the virus. According to Mazzucchelli et al. (2020), these impositions of rules to combat COVID-19 are more easily done in countries where the level of democracy is lower. For the author, nations with a high degree of democracy tend to have more time to take measures of confinement, closing schools and prohibiting meetings.
The present work began with a curious comparison in the fight against the pandemic between neighbouring South American countries Brazil and Argentina. Both countries have similar challenges regarding social inequality and economic development. These two nations are also presidential countries and have a concentration of national power at the executive level. Furthermore, in recent years, Brazil and Argentina have experienced an increase in political polarisation, with high levels of mobilisation of movements from the right and left (Abers et al, 2021).
Currently, Brazil is governed by a self-declared right-wing government that, since the beginning of the pandemic, has chosen, at least at the federal level, not to institutionalise the protocols of social distancing that are defended by experts (de Oliveira et al., 2021). On the other hand, the Argentine government’s self-declared leftist, since the beginning of the coronavirus pandemic, has decreed the institutionalisation of social distances, closing of businesses and protective measures such as the use of masks.
The results show that, on average, the implementation of intervention policies in physical distancing is correlated with a reduction in the incidence of transmission of COVID-19 cases (Islam et al., 2020), but according to Rawson et al. (2020), government authorities have difficulty in keeping population mobility under control for a long period of time. In the study by Rieger et al. (2020), it was identified that, over time, there is a deterioration of restrictive lockdown measures, which is characterised by an increase in the movement of people in places not authorised by government decrees.
According to Chaudhry et al. (2020), restrictive lockdown measures are unsustainable in middle-income countries, as the cost to the population is very high, generating social, economic and psychological impacts. Income inequality between countries and poverty levels in cities are correlated with the dissemination of COVID-19, as in these nations the population is concentrated in urban areas and most residents are informal workers, which prevents them from staying in their homes during the pandemic (Bolaño-Ortiz et al., 2020).
Another problem in cities is the higher population density, which is related to the increase in the speed at which the virus is transmitted between people, increasing the number of cases and deaths from COVID-19 (Ilardi et al., 2021). However, Valev (2020) demonstrates that population density does not have a statistically significant impact on the increase in deaths per million inhabitants of COVID-19. The author also points out that there is a correlation between GDP per capita and the increase in deaths caused by the new coronavirus, that is, the higher the per capita income of a country, the greater the number of deaths per million inhabitants.
Due to the level of democracy, countries have different results in combating the new coronavirus pandemic. For a country to have good results in controlling the new coronavirus pandemic, it is necessary that immediate responses are carried out to effectively implement such actions; however, countries with a greater degree of democracy have greater difficulty in implementing confinement policies that are correlated with reduced transmission and mortality from COVID-19 (Mazzucchelli et al., 2020).
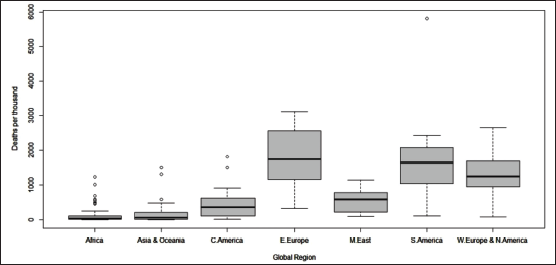
Although it is currently difficult to separate political preferences from rationality, when we analyse the fight against the pandemic through data on deaths per million inhabitants, the differences in the fight against the epidemic between the Argentine and Brazilian governments do not seem to have had many effects, in which Argentina is slightly better than Brazil in the nightmare of the deaths that occurred. In fact, after analysing the data, it is possible to see that South America is the most punished region on the entire planet by COVID-19. However, it is not only South America that finds itself in this situation but also Eastern Europe is in a catastrophic situation.
In a pandemic, people are not affected equally, as poorer populations tend to be affected more drastically. For example, in the fourteenth century, the world was hit by the Black Death, which reduced the population by a third, with the majority of fatalities being observed in the poorest strata of society. In medieval Europe, undernourished peasants with poor access to health were easy prey for the bubonic plague.
Nowadays, the new coronavirus has also affected the population unequally, as poorer populations are more likely to have chronic diseases, which increases the risk of mortality associated with COVID-19 (Ahmed et al., 2020). According to Shahbazi et al. (2020), there is a correlation between the Human Development Index and the COVID-19 morbidity and mortality because in countries with a higher HDI there is an increase in life expectancy that is also equivalent to an increase in the number of elderly people in the country. It is worth remembering that the new coronavirus mainly affects the elderly population, thus showing that older people are more likely to have a disease progression, as the immune system is less able to deal with infectious challenges (Zhou et al., 2020).
There is also a low mortality rate in regions where income is lower due to underreporting of new cases of COVID-19, as the health system in these locations has difficulty in employing tracking policies for people infected by the virus (Shahbazi et al., 2020) and this underreporting of cases also has an impact on the mortality rate, as countries with a higher number of cases per million inhabitants have a higher number of deaths from the virus (Valev, 2020).
Although the aetiology of the new coronavirus is widely studied, there is still a gap about how socio-economic variables impact the effects of the pandemic on the population in different parts of the world. Thus, this article aims to contribute to the literature by providing empirical evidence on how these factors influence mortality in different regions of the five continents and also for future public policies for disease prevention. In addition to this brief introduction, the work has three more sections. The second section describes the data used and the quantitative methods, section three presents and discusses the results and, finally, section four concludes.
Methodological procedures
Data
In order to analyse the data that can contribute to decision-making related to the targeting of public health policies worldwide, we consider income variables, such as GDP per capita and Human Development Index; health: percentage of the population with two doses of vaccine, deaths from COVID-19 per million inhabitants, tests available per capita, percentage of the population with diabetes and hospital beds available per capita; demographic: percentage of the population over 70 years; geographic: population density and finally, social: democracy index and Gini coefficient, which measures social inequality.
Data from 186 countries were consolidated by the authors and obtained, on 28 June 2021, in Our World in Data, 1 such as the percentage of the population with two doses of vaccine, deaths from COVID-19 per million inhabitants, percentage of population with diabetes, percentage of population over 70 and available hospital beds per capita, ONU 2 population, population density and GDP per capita and World Meters 3 available tests.
Methodology
In addition to analysing the correlation between the variables considered by the work, we will use the statistical method of ordinary least squares (OLS), seeking to capture a linear relationship between such variables. The equation initially estimated is:

Where,
As explained by Yue et al. (2018), OLS is the best-known of all regression techniques, being a method for estimating unknown parameters in a linear regression model. It aims to minimise the sum of squares of differences between the observed responses—explained variable—in the given data set and those predicted by a linear function method of a set of explanatory variables.
The OLS method is seen as the sum of the squared vertical distances between each data point in the set, and the corresponding point on the regression line, the smaller the differences, the better the model fits the data. The regression equation is also the mathematical formula applied to explanatory variables to better predict the dependent variable, in which each explanatory variable is associated with a regression coefficient that describes the strength and sign of the relationship of this variable with the dependent variable (Yue et al., 2018).
Results
After analysing the data, it is possible to see that South America is the most punished region on the entire planet by COVID-19. However, it is not only South America that is in this situation but also Eastern Europe is in a catastrophic situation, as can be seen in Figure 1.
Deaths by COVID-19 in Every Region of the World.
The dependent variable is the number of deaths per million inhabitants of the countries, and initially, we analyse which, among the explanatory variables of the model, have the most significant correlations with the dependent variable, which can be seen in Figure 2.
Correlation Between the Considered Variables.
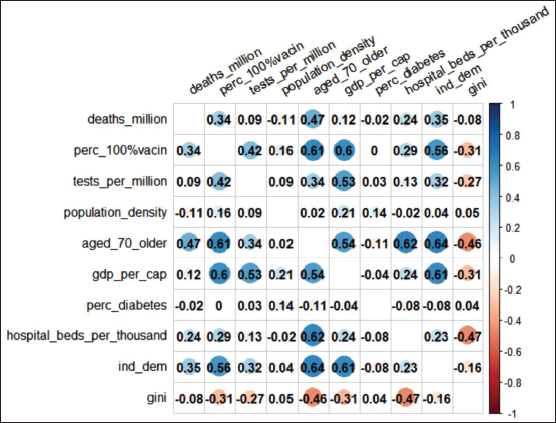
For Ilardi et al. (2020), the increase in the population density rate is related to the transmission of the new coronavirus, which will impact the increase in the number of cases and also the increase in the mortality rate. However, the results found in this study were contrary to this finding, after all, population density has a negative correlation with the mortality rate.
The percentage of diabetics also had a negative relationship with the increase in the mortality rate, which also diverges from the results proposed by Jordan et al. (2020) and Huang et al. (2020), who concluded that diabetic individuals had a higher risk of clinical complications that could lead to an increase in the mortality rate of people infected by SARS-CoV-2.
As pointed out in the literature, the percentage of the population over 70 years old has a strong correlation with the mortality rate. In addition, the democracy index also has a slight positive correlation with the variable deaths per million inhabitants, probably as a reflection that democracies take longer to take measures to combat the pandemic since they have less reprehensible mechanisms for the movement of people and maintenance of lockdowns for a short period of time as predicted by Mazzucchelli et al. (2020).
Another clear correlation is between the percentage of the population with two doses of vaccine and per capita income. As you can see from the diagram, this correlation is quite strong, which was to be expected, as countries with higher incomes manage to acquire vaccines more quickly.
In a context of virtually war that humanity is currently facing, initially, one could imagine that the poorest countries would be the most affected, as they have less strong states and populations with less formal education to face the pandemic. However, when analysing the data from countries divided by quartiles of per capita income, it is clear that the poorest regions have much lower mortality rates than the richest regions. 4 These results can be seen in Table 1.
Deaths by COVID-19 Per Million Inhabitants.

Even though the countries with the highest per capita income have high mortality rates, interestingly, it is the upper-middle-income countries that have the highest rates. In fact, countries in the bottom quartile of per capita income have a mortality rate nearly 20 times lower than upper-middle-income countries. This result can be explained because the population of these countries has an inequality in access to health services, with high and high-middle-income countries tending to have more access to health care, which provides more tests for the diagnosis of COVID-19. On the other hand, low-middle-income and low-income nations tend to have greater underreporting of cases of the new coronavirus, as local people do not have easy access to health care (Shahbazi et al. 2020).
A second explanation is that in middle-income countries, the population is considered urban, which increases population density, and as expressed earlier, workers in middle-income countries are mostly informal, which makes it impossible to carry out a lockdown very much prolonged, as this sanitary measure causes a drop in the income of residents, which is also correlated with an increase in civil disobedience in relation to the fulfilment of social distancing policies imposed by local governments (Rieger et al., 2020).
However, there is one more relevant point. Despite having worrying levels of deaths per capita, the upper-middle-income countries have a high standard deviation, which makes their median smaller than that of richer countries. This reveals that there is great heterogeneity among countries at this level of income, that is, upper-middle-income nations have a higher rate of inequality in access to health services. This result also confirms what Ahmed et al. (2020) point out, that is, poorer populations are more affected by COVID-19, as they are more likely to have chronic diseases that are responsible for increasing the mortality rate of the new coronavirus.
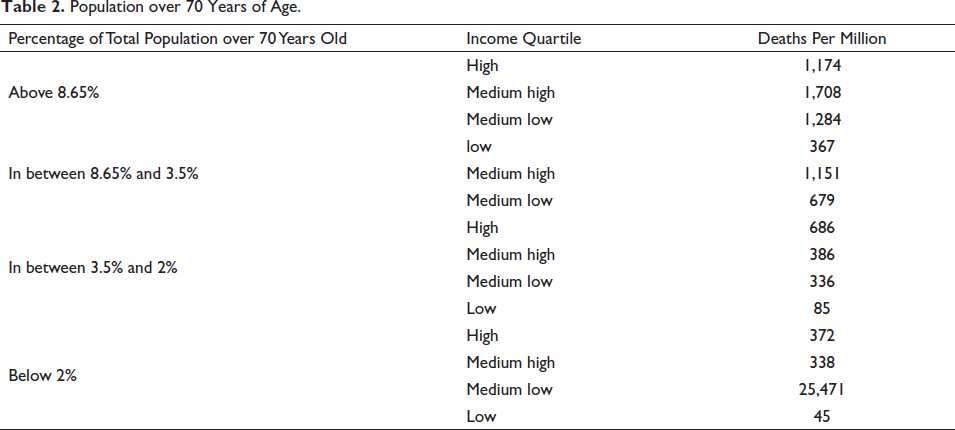
It can be argued that, in addition to income, the most relevant variable for higher mortality is the proportion of elderly people in the country’s population, even because, as shown above, the percentage of the population over 70 years of age is the variable with the highest correlation with deaths per million. However, even in countries with a higher proportion of elderly people in relation to the total population, the highest mortality occurs in upper-middle-income countries (with the exception of countries with a very low population of elderly people over 70 years old, where mortality in high-income countries is slightly higher than those of upper-middle-income countries), as shown in Table 2.
Population over 70 Years of Age.
As we are considering a disease communicable between human beings through the airways, it is to be expected that higher concentrations of people and populations can contribute to higher mortality per capita. However, counterintuitively, the correlation—albeit weak—between countries’ population density and mortality is slightly negative (for example, Bangladesh, one of the countries with the highest population densities on the planet, has a mortality rate of 93 per million, 27 times smaller than Brazil, which has a population density 50 times smaller).
This finding contradicts what Ilardi et al. (2020) point out the positive correlation between population density and the increase in cases and deaths from COVID-19. However, this result confirms what was exposed by Valev (2020), that is, there is no positive correlation between the population index of a country and the increase in cases and deaths per million. This is because not only the density of a country is enough but also there is the need for it to have a large enough per capita income that leads to a greater connection with the outside world.
Estimating the linear regression described in Equation 1, we arrive at the result presented in Table 3.
Regression Results.
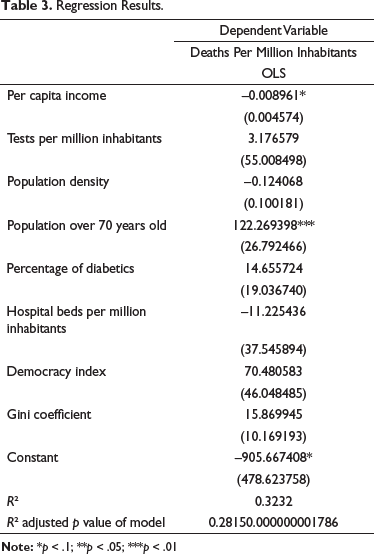
Although the p value of the estimated model is small, it is clear that the p value of several variables is very high, with only the variables per capita income, population over 70 years old and democracy index, having statistically significant values (5%, 1% and 10%, respectively). The R² adjusted of model—which denotes how much the independent variables explain the dependent variable—was 28.15%. The variable per capita income of countries has a negative impact, albeit very low, on deaths per million inhabitants, which is consistent with the fact that countries with income classified as high average have higher fatalities.
This may be because countries with higher middle incomes have a higher life expectancy than countries with low incomes, which increases the proportion of the population over 70 years of age (Shahbazi et al., 2020). At the same time, in these countries, the number of informal workers who are prevented from staying at home during the pandemic is greater than those in high-income countries (Bolaño-Ortiz et al., 2020), as are countries with higher population density - which is related to the increase in the speed at which the virus is transmitted between people (Ilardi et al., 2020) – compared to those with high incomes.
The significance and high positive impact of the population over 70 years, variable on deaths per million inhabitants is due to the higher incidence of chronic diseases in the elderly. They are more likely to develop a more severe degree if infected by COVID-19, requiring some medical intervention (Jordan et al., 2020; Huang et al., 2020). The democracy index had a statistically significant and positive result. According to the literature, countries that have more democratic governments have a greater difficulty in imposing restrictive measures to control the increase in COVID-19 cases (Mazzucchelli et al., 2020).
Conclusion
Initiatives like that of the US government, which donated three million vaccines from the Jansenn 5 to the Brazilian government, in addition to being commendable, are extremely necessary to combat the pandemic on a global scale. As shown, there is a strong correlation between income and vaccination. As a result, rich countries are seeing their mortality rates stagnate while poor countries, as they have more fragile economies and little trade in the world, are still unscathed.
Thus, upper-middle-income countries need greater attention from the international community, either because they have economies with considerable trade or because their fiscal restrictions do not allow for the maintenance of very extensive lockdowns, as well as the purchase of vaccines at levels necessary for full immunisation.
However, even considering the upper-middle-income countries—which have a high heterogeneity, with some succeeding in fighting the pandemic and others in worrying situations—public policies at the world level must be focused on a regionalised basis. As shown, South America and Eastern Europe—at the moment—need the greatest need for attention.
This is because it is in the interest of the entire world that the pandemic does not go out of control in any region, as this could trigger the emergence of increasingly lethal or even resistant vaccine variants, requiring the international community to give a greater focus in these countries, notably South America and Eastern Europe, than in the poorer countries. As a suggestion for future research, the investigation of the influence of the levels of lockdowns adopted on deaths by COVID-19 can be mentioned.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.