
Abstract
Prior to the COVID-19, various issues in ethics, laws, regulations and security risks limited physicians in their ability to deliver medical care via telemedicine. However, in 2020, telemedicine quickly became mainstream when the US government issued a waiver granting the use of telemedicine to reduce COVID-19 transmission. This study examined the US physicians’ acceptance of telemedicine after its sudden wide-scale implementation. The authors developed a survey based on the Unified Theory of Acceptance and Use of Technology to assess the US physicians’ intentions and attitudes toward the use of telemedicine in the delivery of medical care. This survey was distributed between March and June in 2021 across several voluntary online physician groups. The survey was validated using factor analysis. The 110 participants who completed this study were all active physicians practising telemedicine in the USA. The majority of the participants were female (93%), between 34 and 59 years of age (93%), had at least 10 years of medical experience (84%) and practised in a city (92%). The behavioural intention to use telemedicine was influenced by performance expectancy (β = 0.34, p<.001), social influence (β = 0.34, p<.001), facilitating conditions (β = 0.14, p<.05) and attitude towards telemedicine use (β = 0.36, p<.001). Attitude towards telemedicine use was influenced by performance expectancy (β = 0.60, p<.001), effort expectancy (β = 0.16, p<.05) and social influence (β = 0.16, p<.05). In addition, telemedicine experience moderated the influence of performance expectancy on behavioural intention negatively (β =−0.39, p<.001) and moderated the influence of facilitating conditions on behavioural intention positively(β = 0.27, p<.001). This study found that the physicians’ performance expectancy of and attitude towards telemedicine use were significant predictors of physicians’ acceptance. Social influence from colleagues and administrators also played an essential role in impacting physicians’ acceptance of telemedicine. Physicians’ effort expectancy merely affected their attitude towards telemedicine use. Facilitating conditions—such as the inability to perform physical exams, labs, etc.—only influenced the physicians’ intention to use telemedicine. Finally, the survey data suggested that as physicians gained telemedicine experience, their performance expectancy predicted lower behavioural intention than counterparts with less experience.
Keywords
Introduction
Telemedicine is defined as the distant delivery of healthcare and exchange of medical information between patients and their healthcare providers via information, communication and networking technologies in order to promote health maintenance, prevention, alleviation and remedy of disease, pain and suffering (Waller & Stotler, 2018). Telemedicine enabled patient interactions with healthcare providers, exchange of medical information and patient remote monitoring from distant locations; the latter proved especially useful in rural and remote environments where medical services were limited (Craig & Petterson, 2005). Telemedicine also increased access to medical care through video consultations with healthcare providers (Waller & Stotler, 2018). Using home-based video interactions, a healthcare provider could perform an observational assessment after obtaining a thorough history of symptoms and exposure risk from the patient (Portnoy et al., 2020). Typical applications of telemedicine included general health care, dermatology, eye exams, nutrition counselling, medical consultations and prescriptions, nursing, teleradiology, psychotherapy, teleneurology and other applications (Nittari et al., 2020). As telemedicine improved access to medical services, increased healthcare delivery, reduced healthcare costs and promoted communication between health professionals and other benefits, it would be imperative to understand how readily physicians would accept telemedicine in medical care (Ekeland et al., 2010; Hjelm, 2005).
Telemedicine had remained relatively uncommon in healthcare delivery prior to wide-scale implementation, in 2020, due to the public health emergency from COVID-19. Its uncommon use was mainly because of prevalent business models, minimal cost benefits, limited financial funding, concerns about data security and compliance and inadequate legislation available for legal and ethical issues (Chen et al., 2013; Effertz et al., 2017, Mehrotra et al., 2021; Nittari et al., 2020; Peters et al., 2015; Sterling & LeRouge, 2019). Nonetheless, telemedicine was recognised as a disruptive innovation that could transform the healthcare industry by potentially reducing costs, and increasing quality of care, as well as patient satisfaction (Schwamm, 2014; Sterling & LeRouge, 2019). Despite these benefits, the healthcare industry often found little or no cost benefits from telemedicine due to inadequate insurance reimbursement. The early business processes around telemedicine were geared towards businesses rather than users due to its low utilisation, extra resources needed for staff training, additional staffing and difficulty in satisfying the requirements of regulatory and compliance agencies, for example, Health Insurance Portability and Accountability Act (HIPAA), 1996, Privacy, Security and Breach Notification Rules (Chen et al., 2013; Nittari et al., 2020; OCR, 2022; Sterling & LeRouge, 2019; Wade et al., 2010). Often, providers and patients did not utilise telemedicine services because health insurance like Medicaid (Centers for Medicare & Medicaid Services, 2020) in the United States did not reimburse telemedicine expenses well (Acheampong & Vimarlund, 2015). The number of telemedicine visits thus remained infrequent prior to 2020, as many healthcare providers refused to carry out telemedicine activities due to legal risks, such as the possibility of malpractice suits (Nittari et al., 2020). By and large, many healthcare providers could not provide telemedicine services unless they practised in rural/remote areas with limited medical access (Campbell et al., 2001) or during emergencies, such as natural disasters, injury hazards (Simmons et al., 2008), exposures to contaminations and disease epidemics (Ohannessian, 2015). As such, ‘face-to-face consultation between physician and patient remained the gold standard of clinical care’ (WMA General Assembly, 2018).
It was not until the global outbreak of the COVID-19 in 2020 that telemedicine became a mainstream method in order to reduce COVID-19 transmission risks (AMA, 2020). Many businesses shifted from face-to-face interactions to real-time audio and video communications, social media and other internet platforms through the information and communications technology (Nicola et al., 2020). Similarly, a drastic shift occurred in medicine, whereby the US legislation required all insurers, including Medicare (Centers for Medicare & Medicaid Services, 2020) and employee health plans, to reimburse medical services delivered through telemedicine in response to the COVID-19 public health emergency (PHI, 2020; Severino & Director, 2020). As a result, the number of virtual visits in the USA surged to more than 12% of all outpatient visits between March and April in 2020 (Mehrotra et al., 2021). Similarly, scholarly literature saw an explosion of papers on telemedicine. Despite all this, the physicians’ acceptance of telemedicine has received limited research interest.
The Unified Theory of Technology Acceptance and Use
To adequately predict how users would accept any technology, Davis’s Technology Acceptance Model (TAM) was the first of its kind that envisioned how perceived usefulness and ease of use could influence one’s intention to and subsequent use of the system (Davis, 1989). In order to predict users’ intention and resultant use of the technology, parsimonious explanations of end-user reactions were necessary. Further studies and expansions of the TAM resulted in two major upgrades. First, TAM was extended into TAM2 by including social factors that could influence users’ intentions and usages (Venkatesh et al., 2003). Second, through empirical validations and comparisons, Venkatesh et al. (2003) formulated the Unified Theory of Acceptance and Use of Technology (UTAUT) by combining several prominent models, along with TAM and TAM2. This yielded several core determinants of users’ intentions and usages, along with several moderators of key relationships (Venkatesh et al., 2003, Venkatesh et al., 2012). Ultimately, the goals of assessing technology acceptance were to promote successful implementations and continuous improvements (Berg, 2001).
The UTAUT was built on the following theoretical constructs (Fishbein & Ajzen, 1975):
Attitude (affect: feelings and evaluations) was referred to the ‘person’s feelings towards and evaluation of some object, person, issue or event’ (Fishbein & Ajzen, 1975). In particular, attitude towards technology use was defined as ‘an individual’s overall affective reaction to using a system’ (Venkatesh et al., 2003). Belief (cognition: opinions and beliefs) was defined as ‘the person’s favourable or unfavourable evaluation of an object’ (Fishbein & Ajzen, 1975). A belief was further distinguished into three groups: ‘Behavioural belief’ was related to believing the consequence of a specific behaviour, ‘normative belief’ was a belief subjected to what others believe in and ‘control belief’ involved specific factors that would enhance or degrade behavioural performance (Ajzen, 1991). In UTAUT, performance expectancy (PE), effort expectancy (EE), social influence (SI) and facilitating conditions (FC) were the constructs for beliefs, which would later be expanded in this section. Behavioural intention (conation), a special case of beliefs, was referred to the individual’s intention to perform a given behaviour, indicating the willingness and planning to exert the necessary effort for a specific behaviour (Ajzen, 1991). Behaviours (observed overt acts) were defined as the ‘observable acts of the subject’ (Fishbein & Ajzen, 1975). For instance, the output variable in UTAUT would be the use behaviour (Venkatesh et al., 2003).
The theory maintains that positive attitudes and beliefs, high use and positive behavioural intention (BI) led to accepting the technology favourably (Davis, 1989). The two constructs that defined the use of and the intention to use the system were the use behaviour and BI, respectively. Moreover, to explain and predict these behaviours, UTAUT included the four determinants—PE, EE, SI and FC—that would influence user intentions and usage (Venkatesh et al., 2003). In addition, several studies found that the attitude towards the use of telemedicine (ATT) played a central role in influencing user acceptance of technologies (Dwivedi et al., 2019). Finally, UTAUT suggests that the four moderators with specific user characteristics—age, gender, experience and voluntariness of use—would alter the determinants’ effects on ATT, BI and use behaviour (Dwivedi et al., 2019; Venkatesh et al., 2003).
The Research Constructs
This research employed the UTAUT to examine the physicians’ acceptance and use of telemedicine. This section presents how the authors developed the research constructs in accordance with the UTAUT literature. To ensure each construct developed met the original definition, the authors developed three to four survey items from the original theory (also named ‘root scales’), so they were more relevant to physicians’ acceptance of telemedicine during the pandemic.
‘Use behaviour’ was an objective measure that indicated the extent of a physician’s use of telemedicine. Typically, use behaviours were measured and recorded via methods such as collecting system logs (Venkatesh et al., 2011). Unfortunately, the present study did not involve collecting and recording any observable data for use behaviours.
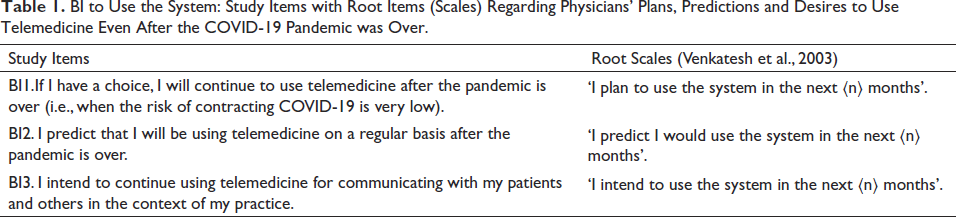
‘BI’ was a subjective measure of a physician’s intention to employ telemedicine in a clinical setting. As outlined in Table 1, physicians’ plans, predictions and desires to use telemedicine even after the end of the COVID-19 pandemic were shown to be true predictors of their intentions to use telemedicine. According to Venkatesh et al. (2003), users’ BI to use technology rather than their actual use behaviour would strongly suggest their acceptance of technology. Therefore, it would be sufficient to utilise BI to predict physicians’ acceptance of telemedicine.
BI to Use the System: Study Items with Root Items (Scales) Regarding Physicians’ Plans, Predictions and Desires to Use Telemedicine Even After the COVID-19 Pandemic was Over.
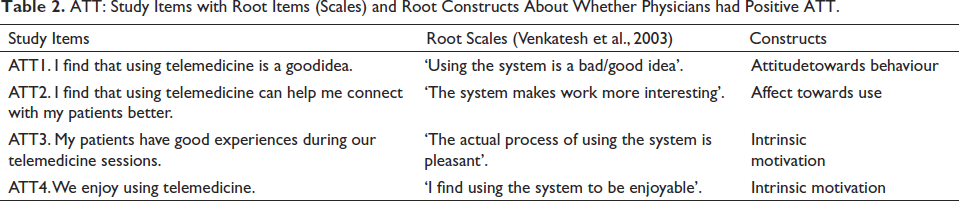
ATT was defined as ‘an individual’s affective reaction to using a system’ (Venkatesh et al., 2003). As shown in Table 2, ATT was derived from the four root UTAUT constructs. The root constructs were described as follows. First, attitude towards behaviour would reflect positive feelings healthcare providers had towards telemedicine use. Second, effect towards use would represent the extent of joy, elation or pleasure healthcare providers experienced when they conducted telemedicine visits. Third, intrinsic motivation would reflect how much healthcare providers were motivated to use telemedicine for the sole purpose of the activity (Venkatesh et al., 2003).
ATT: Study Items with Root Items (Scales) and Root Constructs About Whether Physicians had Positive ATT.
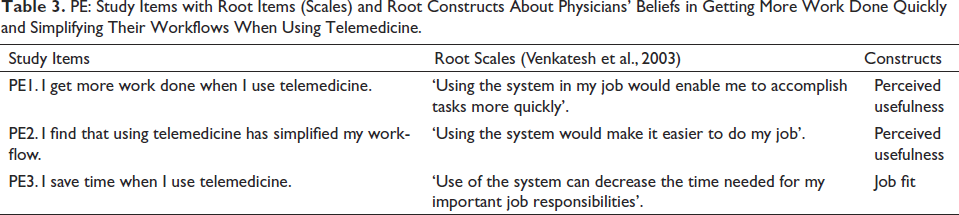
‘PE’ was defined as ‘the degree to which an individual believed that using the system would help him or her to attain gains in job performance’ (Venkatesh et al., 2003). As shown in Table 3, the PE items are based on two root UTAUT constructs,. Both perceived usefulness and job fit were related to how much healthcare providers believed telemedicine would enhance their clinical performances (Venkatesh et al., 2003).
PE: Study Items with Root Items (Scales) and Root Constructs About Physicians’ Beliefs in Getting More Work Done Quickly and Simplifying Their Workflows When Using Telemedicine.
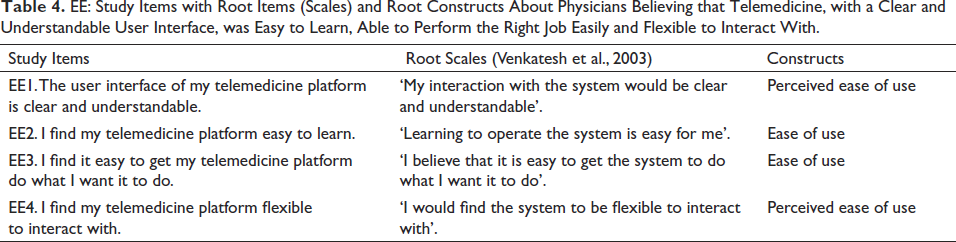
‘EE’ was defined as ‘the degree of ease associated with the use of the system’ (Venkatesh et al., 2003). As illustrated in Table 4, this study incorporated EE from the following two root constructs under UTAUT. First, as per (Venkatesh et al., 2003), perceived ease of use would show how much healthcare providers believed that the telemedicine system was “free of effort.” Second, ease of use would reflect healthcare providers’ perceptions about how easy it was to use telemedicine (Venkatesh et al., 2003).
EE: Study Items with Root Items (Scales) and Root Constructs About Physicians Believing that Telemedicine, with a Clear and Understandable User Interface, was Easy to Learn, Able to Perform the Right Job Easily and Flexible to Interact With.
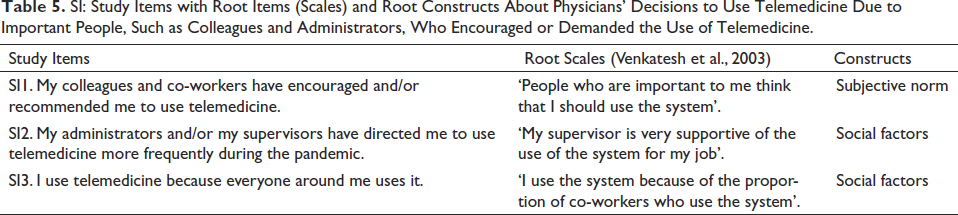
‘SI
SI: Study Items with Root Items (Scales) and Root Constructs About Physicians’ Decisions to Use Telemedicine Due to Important People, Such as Colleagues and Administrators, Who Encouraged or Demanded the Use of Telemedicine.
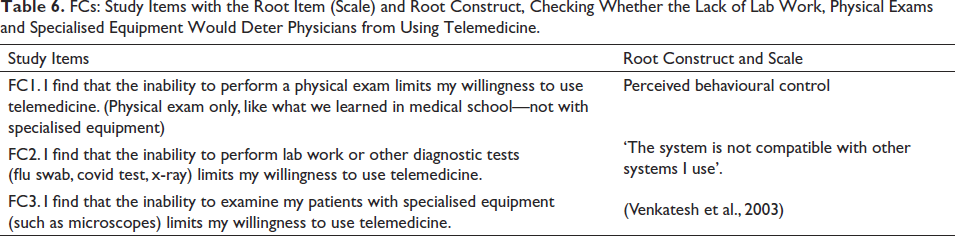
‘FC’ was defined as ‘the degree to which an individual believed that an organisational and technical infrastructure existed to support the use of the system’ (Venkatesh et al., 2003). Some types of telemedicine were more easily arranged at patients’ homes. For instance, consultative visits would require video-conferencing equipment (e.g., webcams, etc.) to communicate between providers and patients, whereas remote monitoring would focus on taking periodic biomedical measurements by remotely using low-cost equipment, such as blood pressure cuffs, thermometers and digital scales (Baker & Stanley, 2018). On the contrary, facilitated virtual visits would require specialised equipment, such as a telemedicine examination camera and digital microscope, to conduct remote physical exams. Typically, these virtual visits would necessitate patients to travel to facilities equipped with proper technologies and resources (Baker & Stanley, 2018). ‘Physicians must be aware that certain telemedicine technologies could be unaffordable to patients and hence impede access’ (WMA General Assembly, 2018). Consequently, imposing these FCs might further limit people from using telemedicine platforms. Therefore, it would be interesting to see whether the lack of lab work, physical exams and specialised equipment would prevent physicians from using telemedicine, as shown in Table 6.
FCs: Study Items with the Root Item (Scale) and Root Construct, Checking Whether the Lack of Lab Work, Physical Exams and Specialised Equipment Would Deter Physicians from Using Telemedicine.
Moderators
A moderator is a variable that can affect the influence of an independent variable on a dependent variable. The UTAUT suggests four moderators: age, gender, experience and voluntariness of use. This subsection describes the moderators suitable for this study.
‘Age’ stereotypes often occur in workplaces. Older workers might be ‘much more accustomed to seeking and applying traditional (i.e., ‘non-technology’) solutions to job-related tasks whereas younger workers are much more reliant on the use of technology for job accomplishment’ (Morris & Venkatesh, 2000). Age was specified as the number of years, as indicated in Table 7.
Moderators: Study Items with Two Moderating Variables Available in This Study.
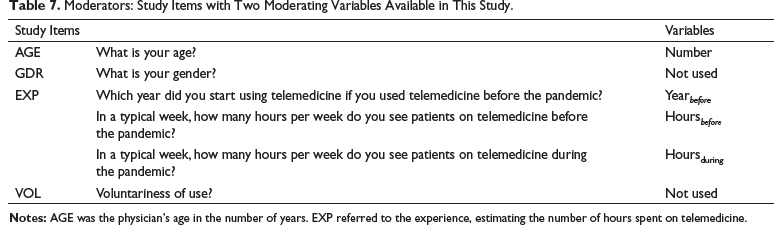
The justification for using ‘gender’ as a moderator would lie in the gender stereotypes, in which women might possess different ideals from men in workplaces (Venkatesh et al., 2011). However, gender differences were unlikely to occur among physicians because of their professional values and continual commitments to their profession (Venkatesh et al., 2011). Therefore, the gender moderator was dropped from the present study.
‘Experience’ (EXP) was related to how much time a user spent using the system. In the UTAUT model, measuring experience involved collecting longitudinal data once every few weeks or months (Venkatesh et al., 2003). However, because collecting data periodically was infeasible in the present study, this study instead compiled self-reported times by querying about the duration of telemedicine use before (hours before since years before) and during the COVID-19 pandemic in a typical week (hours during) (Araujo et al., 2017), as shown in Table 7. The authors gauged the respondents’ experiences by summing up their typical weekly hours of telemedicine use before (EXPbefore) and during (EXPduring) the COVID-19 pandemic in the equation below.

‘Voluntariness of Telemedicine Use’ (VOL) was defined as ‘the degree to which the use of the telemedicine [was] perceived as being voluntary, or of free will’ (Venkatesh et al., 2003). At the onset of the pandemic, many physicians shifted from in-person visits to telemedicine visits, which continued until the time of the survey, as most physicians were employed by health systems and corporations (Primary Care Collaborative, 2022). As such, the voluntariness of use as a moderator would not have any significant variance during which the study was conducted and was thus dropped from this study.
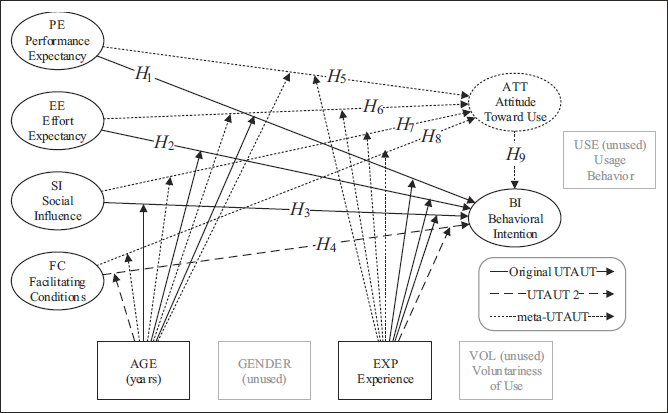
The Figure 1 delineates the relationships between the determinants, moderators and the outcome variables presented above.
Hypotheses
Based on the above discussion, this study presents the following hypotheses.
H1: PE would have a positive and direct effect on BI.
H2: EE would have a positive and direct effect on BI.
H3: SI would have a positive and direct effect on BI.
H4: FC would have a positive and direct effect on BI.
H5: PE would have a positive and direct effect on ATT.
H6: EE would have a positive and direct effect on ATT.
H7: SI would have a positive and direct effect on ATT.
H8: FC would have a positive and direct influence on ATT.
H9: ATT would have a positive and direct influence on BI.
Methods
The authors administered online surveys between March and June in 2021. Hosted on SurveyMonkey, these surveys were advertised on several voluntary online community support groups for physicians exchanging information about the ongoing COVID-19 pandemic. As such, any active physician with either an MD or DO degree who practised telemedicine in the United States could participate in this survey. Before filling out the surveys, all participants agreed to a written informed consent required by the Institutional Review Board (IRB). The IRB reviewed the survey methodology and granted clearance pertaining to ethics concerning human subjects and privacies. Despite 165 participants attempting to fill out the surveys, only 110 who completed the surveys could be used in this study.
Most of the participants were women (93%) between 34 and 59 years of age (93%), had at least a decade of medical experience (84%), and practised medicine in the urban (67%) and the Middle Atlantic USA (48%). Many participants practised medicine in hospitals (70%) for at least 30 hours per week (72%), specialising in paediatrics (20%), internal medicine (14%), psychiatry (11%) and other medical fields.
Most participants did not use telemedicine before the COVID-19 pandemic (88%). During the pandemic, 40% of survey participants conducted more telemedicine visits than in-person visits with patients. Most participants (66%) did not have a choice in whether they used telemedicine in their practices, while others were responsible for making the full decision on telemedicine use (20%) or involved in decision-making groups (14%).
Participation in the survey was purely voluntary; participants were free to take surveys and withdraw at any time. Additionally, all participants were required to agree to the informed consent to be eligible for the survey, which minimised any coercion or undue influence.
Measures and Covariates
Figure 1 illustrates the hypothesised relationships described above. The output construct was the BI listed in Table 1 with three items: BI1, BI2 and BI3. The mediator was the ATT listed in Table 2 with four items: ATT1, ATT2, ATT3 and ATT4. The first determinant was PE listed in Table 3 with three items: PE1, PE2 and PE3. The second determinant was EE listed in Table 4 with four items: EE1, EE2, EE3 and EE4. The third determinant was SI listed in Table 5 with three items: SI1, SI2 and SI3. The last determinant was FC listed in Table 6 with three items: FC1, FC2 and FC3.
Table 7 summarised the moderators in the present study. The first moderator was AGE, an integer value representing the number of years in age. The second moderator was EXP, an integer value calculated using Equation 1 that would estimate the amount of time per week the user partook in telemedicine activities since the beginning of their telemedicine use.
Data Collection
The online survey consisted of several pages that could take up to 30 minutes to complete. On the first page, the participants would fill out their personal information, including their age, gender and location where they practised medicine. On the next page, they would provide their work habits and telemedicine use before and during the COVID-19 pandemic. The next few pages included items derived from the UTAUT model.
Once all the survey responses had been collected, the authors scaled the survey items on a uniform Likert-7 scale between –3 and 3, depicting strongly disagree (–3), disagree (–2), somewhat disagree (–1), neither disagree nor agree (0), somewhat agree (1), agree (2) and strongly agree (3).
In order to be consistent with the responses to the other determinants, responses to the FC items (FC1, FC2 and FC3) were scored on a reversed scale. For example, for item F1 (‘I find that the inability to perform a physical exam limits my willingness to use telemedicine’ in Table 6), –3 denoted strongly agree and 3 strongly disagree.
Data Diagnostics
This section describes the statistical analysis performed to determine the statistical validity of the collected date.
Exploratory Factor Analysis (EFA)
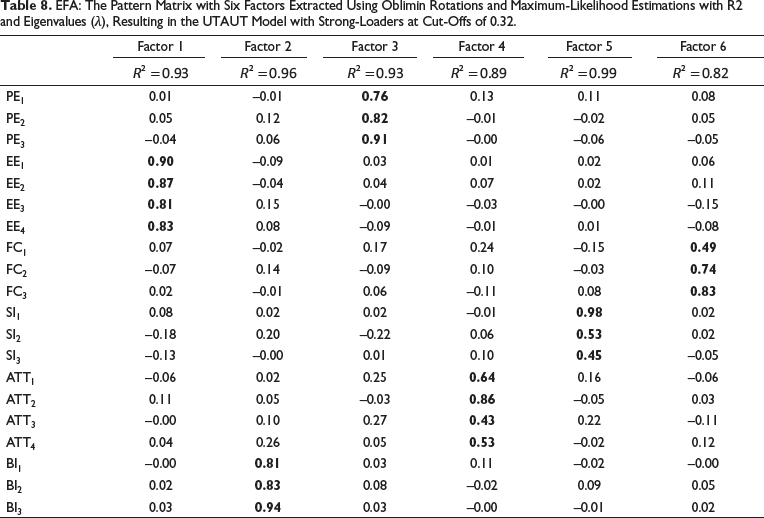
EFA is a statistical technique used to discover the underlying structure. This analysis involves a pattern matrix consisting of loaders (correlations between -1 and -1) that were arranged in item rows and factor columns (Tabachnick et al., 2013). With the pattern matrix, one would isolate all the correlating items with strong loaders into independent factors (Tabachnick et al., 2013). As a rule of thumb, choosing strong loaders of 0.32 and above would help identify items with over 10% overlapping variance within the same factor (Tabachnick et al., 2013). The authors followed the above guideline to achieve optimal results by verifying Table 1 through Table 6 with strong loaders over 0.32, as delineated in the pattern matrix.
Sample Size Power and Precision
A well-fitted model is one such that the measured items have significant relationships, which in turn are represented by a non-significant chi-square value (χ2). On the other hand, a significant χ2 (i.e., p < .05) indicates that the measured items are, in fact, independent (Tabachnick et al., 2013). However, χ2 often becomes significant due to minute differences between various items in large samples (Tabachnick et al., 2013). First, as the value of χ2 depends on the sample size, a model with χ2/df > 3 is considered poorly fitted (Cole, 1987). Second, the root-mean-square error of approximation (RMSEA), which indicates the lack of fit compared to a perfect model (Tabachnick et al., 2013), should not exceed 0.08 (Chen et al., 2008). Third, the standardised root-mean-square residual (SRMR) should also not exceed 0.08 (Hu et al., 1999). Therefore, several fit indices ranging between 0 and 1 were developed to determine the extent of the model fit in a large sample size (Tabachnick et al., 2013). Other fit indices, such as comparative fit index (CFI), normed fit index (NFI), Tucker-Lewis index (TLI), goodness-of-fit index (GFI) and adjusted goodness-of-fit index (AGFI), should have high values (e.g., 0.95 or above) in order to indicate a good-fitting, parsimonious model (Tabachnick et al., 2013).
Construct Validity: Convergent and Discriminant Validity
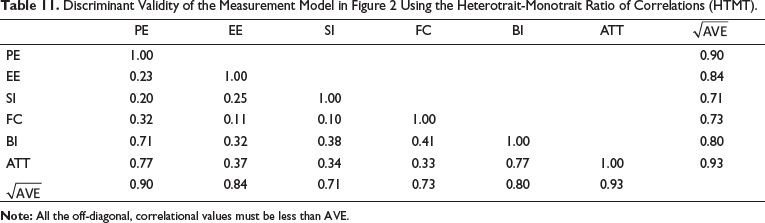
A construct is valid when both convergent and discriminant validities are valid. Convergent validity implies that the measures observed within the same constructs are all related. A common way to determine convergent validity is to observe the values of the average variance extracted (AVE), Cronbach alpha (α) and composite reliability (CR) with AVE ≥ 0.50 (Fornell & Larcker, 1981) as well as α ≥ 0.70 and CR ≥ 0.70 to be convergent valid (Henseler et al., 2009). On the contrary, discriminant validity suggests that the measures from different constructs are not related to one another. One could thus observe discriminant convergence from the correlation table, in which all the correlations with other factors should not exceed the square root of the AVE (Baker & Stanley, 2018) to ensure that different traits were indeed unrelated to each other.
Analytic Strategy
The authors conducted structural equation modelling (SEM), (Nachtigall et al., 2003) to understand various direct and moderating effects. In general, SEM is a collection of statistical techniques that enables researchers to ascertain any relationships between independent and dependent variables (Tabachnick et al., 2013). As such, the authors developed a measurement model to estimate and predict the items described in Table 1 through Table 7 by using the maximum likelihood estimator with the survey data. Subsequently, the authors employed the diagnostic methods described above, in order to validate the measurement model and ensure the model’s acceptability.
To rule out the hypotheses described in the third section, the authors built several structural models that contained a combination of effects and moderations. This resulted in nine direct paths and twenty paths for moderation. By running the structural model with composite values, which were computed from the measurement model, the authors estimated the standardised β-weights with p values. The authors then utilised these β-weights to predict the extent of physicians’ acceptance of telemedicine in accordance with the hypotheses listed in the third section.
Results
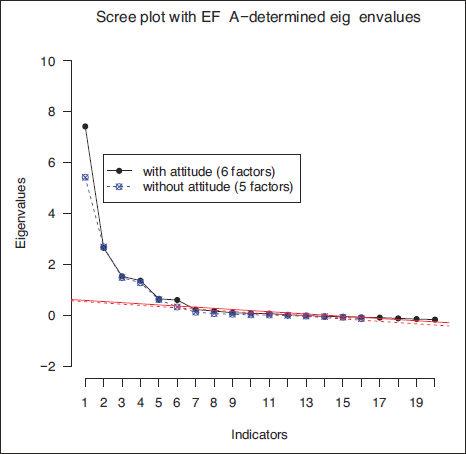
The initial task was to verify whether the items were related to each factor in Table 1 through Table 6 from the survey responses. First, the authors applied the scree test to estimate the number of factors by examining the scree plot (Figure 2)—line plots of eigenvalues in factor analyses against their factor numbers—with and without the ATT described in Table 2. Although several mechanisms were available to determine the cut-off number in a scree plot (Costello & Osborne, 2005), the authors found that cutting off factors after the curve started to flatten aligned well in this research. In other words, the apparent asymptote began around the sixth factor, as illustrated in Figure 2. Finally, to statistically explore and verify the underlying relationships between variables, the authors conducted the EFA on the survey responses with the items in Table 1 through Table 6, as shown in Table 8.
EFA: The Pattern Matrix with Six Factors Extracted Using Oblimin Rotations and Maximum-Likelihood Estimations with R2 and Eigenvalues (λ), Resulting in the UTAUT Model with Strong-Loaders at Cut-Offs of 0.32.
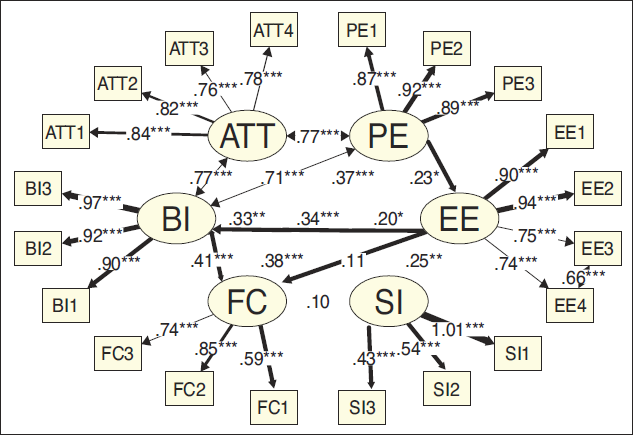
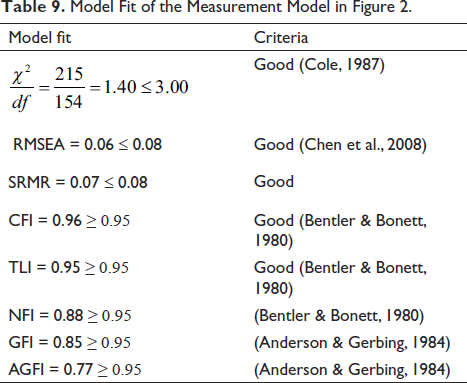
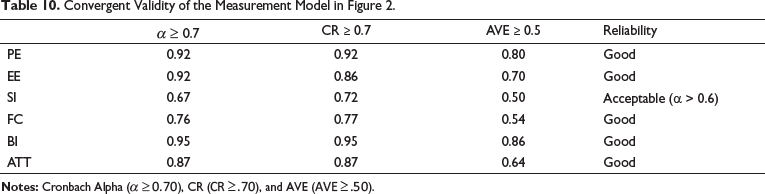
Once the relationships in Table 1 through Table 6 were compared in Figure 2 and Table 8, the authors subsequently applied SEM to compute the measurement model, which quantified the relationship between survey responses and underlying factors described in Section 3. This was illustrated in Figure 3. The authors also included a correlation between EE3 and EE4 in the measurement model (Figure 3) because of their similarities in Table 4. The model appeared to be fitted due to sufficiently fit indices’ values, as shown in Table 9: χ2/df ≤ 3.0, RMSEA < 0.08, SRMR < 0.08, CFI ≥ 0.95 and TLI ≥ 0.95. In addition, the model was convergent valid with α > 0.6, CR ≥ 0.7 and AVE ≥ 0.5, as shown in Table 10 . It was also divergent valid with correlations greater than
Model Fit of the Measurement Model in Figure 2.
Convergent Validity of the Measurement Model in Figure 2.
Discriminant Validity of the Measurement Model in Figure 2 Using the Heterotrait-Monotrait Ratio of Correlations (HTMT).
Finally, to determine which hypotheses from the third section were supported, the authors conducted confirmatory factor analysis on the structural models in Figure 1 using the measurement model in Figure 3. Table 12 presents the direct effects (D) between independent and dependent variables without any moderations, as well as the moderating effects using several moderators: age alone (A), experience alone (E) and both age and experience (A + E) together.
Direct and Total Effects (Σ) on BI and Attitude Towards Telemedicine Use.
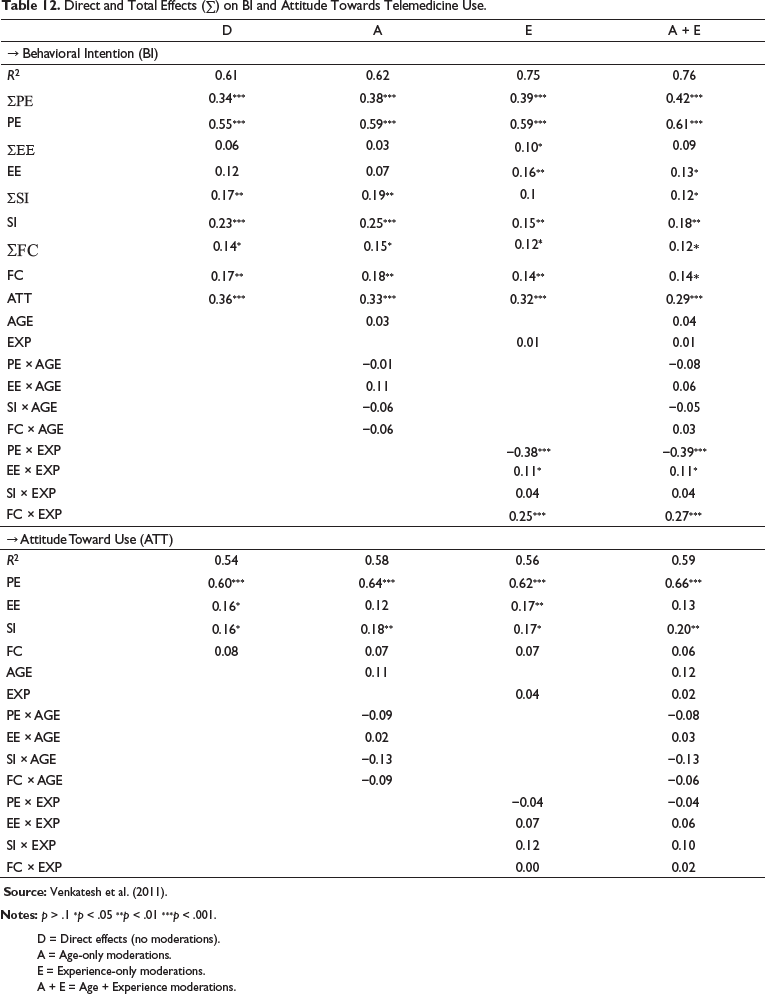
D = Direct effects (no moderations).
A = Age-only moderations.
E = Experience-only moderations.
A + E = Age + Experience moderations.
Discussions
This article explored the US physicians’ acceptance of telemedicine during the COVID-19 pandemic, using the UTAUT. Specifically, this study evaluated the direct effects of physician factors—including their PE, EE, SI and FC (e.g., inability to perform lab work and physical exams)—on their BI and ATT. Furthermore, this study explored the moderating effects of age and experience on these direct effects.
Table 12 summarised Hypotheses from H1 to H9, for which the authors utilised standardised regressions to determine how well they were supported. These values were depicted in Table’s column D, the direct effects. The entries in Table 13 with significant standardised regressions (i.e., p < .05) implied that the corresponding hypotheses were supported and thus marked with checkmarks in the hypothesis column.
Summary of Findings: Direct Effects.
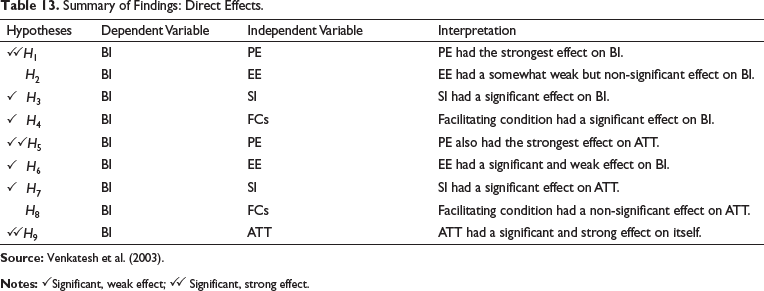
The hypotheses marked with, ✓✓, on the other hand, were strongly supported in this study when their standardised regressions were greater than 0.3 (i.e., with at least a medium effect of 0.3 (Cohen, 1988; Fey et al., 2022).
Hypotheses H1 and H5 were both strongly supported, as physicians’ PE appeared to have the most significant effects on both ATT (β = 0.60 with p < .001 in PE ↓ ATT) and BI (β = 0.34 with p < .001 in PE ↓ BI). Similarly, H9 was strongly supported, as physicians’ ATT exhibited a strong effect on BI (β = 0.36 with p < .001 in ATT ↓ BI). These three findings were consistent with several studies on healthcare professionals’ attitudes towards technologies (Ward et al., 2008), physicians’ acceptance of telemedicine (Garavand et al., 2022) and users’ acceptances of other technologies (Blut et al., 2021).
This article found that EE affects physicians’ attitude (β = 0.16 with p < .05 in EE ↓ ATT) but, interestingly, not their intention to use telemedicine (p > .05 in EE ↓ BI), thus supporting H6 but not H2. A systematic review of physicians’ acceptance of telemedicine (Garavand et al., 2022) examined several studies on UTAUT. While those studies supported the influence of PE (or perceived usefulness) on physicians’ acceptance (i.e., H1), only slightly more than half of those studies supported a similar influence of EE (or ease of use).
This article also examined the role SI played in physicians’ acceptance of telemedicine. As such, both Hypotheses H3 and H7 were supported in this study. SI appeared to play an essential role in influencing physicians’ acceptance of, and attitude towards, telemedicine use (β = 0.17 with p < .01 in SI ↓ BI and β = 0.16 with p < .05 in SI ↓ ATT). These findings were consistent with other studies in technology acceptance (Garavand et al., 2022).
The authors also examined the influence of FC on physicians’ BIs. They found that H4 was supported while H8 was unsupported. In other words, FCs were likely to impact physicians’ BI (β = 0.14 with p < .05 in FC ↓ BI) rather than their attitude towards telemedicine use (p > .1 in FC ↓ ATT). This was reasonable; according to a case report (Pappan et al., 2021), the inability to perform labs or a physical exam on a patient with severe abdominal pain might impact whether their physicians intend to use telemedicine but not the physicians’ overall ATT with other patients. This finding confirms similar conclusions by some other studies on UTAUT.
This article also explored how physicians’ age would moderate various effects. Physicians’ age did not seem to moderate any of the effects in this study because all the standardised regression weights β related to the age moderator were non-significant (i.e., p > .1), as shown in Table 12. This result confirmed the similar conclusion drawn by another study (Venkatesh et al., 2011).
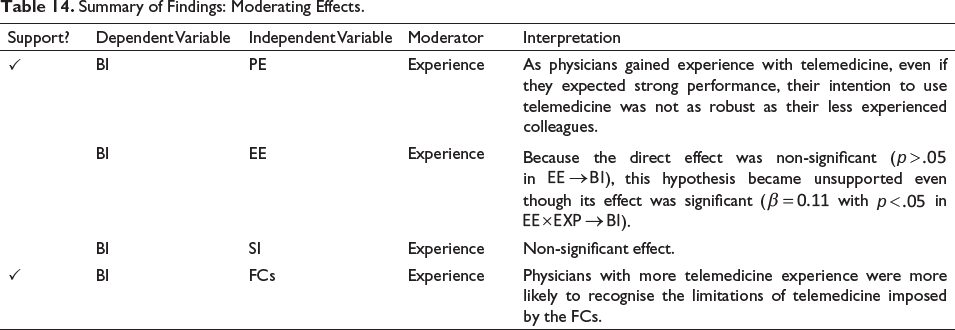
Lastly, summarised in Table 14, this article explored how physicians’ experience (EXP) with telemedicine moderated the effects on BI. EXP, the number of hours a physician weekly spent using telemedicine, appeared to moderate the PE’s effects towards BIs negatively (β = −0.39 with p < .001) but positively on FCs’ effects towards BIs (β = 0.27 with p < .001). These moderations were shown in Table 12’s column A+E. This suggested that as physicians gained experience with telemedicine, even if they expected strong performance, their intention to use telemedicine was not as robust as their less experienced colleagues. On the other hand, physicians with more telemedicine experience were more likely to be painfully aware of the limitations of telemedicine imposed by the FCs. This was in contrast to their less experienced colleagues, who might not have yet encountered a real-life situation in which FCs played a major pitfall in a telemedicine visit. In fact, when queried about the lack of a physical exam via telemedicine, one survey respondent, who had three times more telemedicine experience than most participants, quipped, ‘listening to the lungs is powerful’. One could imagine a clinical scenario in which a patient’s pleural effusion (‘water on the lungs’) could be missed during a telemedicine visit due to the lack of a physical exam.
Summary of Findings: Moderating Effects.
Limitations
These participants in this study were physicians from online support groups exchanging information about the COVID-19 pandemic; therefore, this study could exhibit similar limitations as any online surveys (Andrade, 2020). Namely, these participants could already be savvy in technology use and online communications, which were prerequisite skills to use many telemedicine platforms. Moreover, due to their active online presence in physician interest groups, this study’s subjects were a self-selected group of physicians who could be more readily accepting of telemedicine. Finally, as the participants were physicians primarily located in suburban and urban United States, their beliefs could differ from those serving rural and poor communities.
Conclusion
This study employed the UTAUT to examine the US physicians’ acceptance of telemedicine. As a critical predictor of telemedicine acceptance, physicians’ BI was influenced by their PE, SI, FCs and ATT. Physicians’ ATT was also influenced by PE, EE and SI. In addition, more experience with telemedicine also altered the influence of PE and FCs on physicians’ intention to use telemedicine.
The authors recommended further exploration of the physicians’ acceptance and use of telemedicine in providing healthcare to patients. Such efforts could lead to meaningful implications on the direction telemedicine and digital health product developers should focus their work in the exciting field of digital health.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.