
Abstract
Aims
To examine the extent to which physical therapy at a local tertiary teaching clinic enables best practice and to identify priority areas for service redesign.
Methods
A retrospective file review of clinical records of patients receiving physical therapy (n = 237) from 2011 to 2015 in Manila, Philippines. Data on clinical diagnosis, interventions, parameters of episode of care, goals and outcome measures were extracted and coded by trained researchers using a standardised form.
Results
Most patients (n = 229, 97%) had developmental conditions. Active interventions were employed (n = 236, 99%) and self-management plans appeared in 161 (68%) records. The duration of the episode of care was variable (median = 16 months, range = 1–139). Almost all patients (n = 230, 97%) commenced with weekly sessions, with the total number of sessions ranging from 1 to 150 (median = 15). Therapy goals were reported routinely (n = 236, 99%). Objective measures were recorded in 209 (88%) records at baseline and in 136 (57%) records at follow-up. The time point for outcome assessment was inconsistent (range = <1–36 months).
Conclusions
Service delivery at the clinic requires more robust longitudinal management procedures, streamlined mechanisms for monitoring and better involvement of the family in decision-making. Some elements of existing practice (active, self-management approaches) suggest the adoption of best practice principles. Results contribute to ‘idea generation’ for service redesign.
Keywords
Introduction
The Clinic for Therapy Services, established 1992, is a tertiary teaching clinic that provides care to children with developmental disabilities from low socio-economic backgrounds in Metropolitan Manila, Philippines. The clinic offers allied health services and is a clinical training facility for physiotherapy, occupational therapy and speech pathology students. This needs assessment study evaluated existing service delivery at the clinic as part of a service redesign programme that aims to implement and locally adapt evidence-based management in clinical service delivery and health provider education.
The Clinic for Therapy Services provides vital services for children with disabilities and their families. Paediatric developmental disabilities are globally prevalent (World Health Organization & The World Bank, 2011) and impose a significant burden on the affected children, their families and society. In the Philippines, one in every five persons with disabilities is a child aged between 0 and 14 years (Philippine Statistics Authority, 2013). These children can experience significant limitations in function and in their capacity to participate in valued activities and roles (Anaby et al., 2015; King et al., 2010; Law et al., 2011; Shikako-Thomas et al., 2008; You et al., 2015). In addition, in developing countries such as the Philippines, these children often lack sufficient access to medical, rehabilitation and other healthcare services (Collins et al., 2017; Maulik & Darmstadt, 2007; United Nations Children’s Fund, 2013). There is, therefore, a need for clinic services to ensure best practices by maximising their effectiveness, efficiency and reach.
Best practice for children with developmental disabilities includes fundamental elements that are broadly agreed upon. It is generally accepted that best practice is underpinned by the best available scientific evidence that supports its safety, effectiveness and efficiency (Novak, 2014; Sackett et al., 2001; Schreiber et al., 2009; Westby et al., 2016). In paediatric care, it is also well accepted that the primary focus of management should be on the child, their parent(s) and the extended family (Chiarello, 2013; Hammel et al., 2008; Ketelaar et al., 2001; King & Chiarello, 2014; Rosenbaum & Gorter, 2012; Saleh et al., 2008; Spearing, 2008). Best practice further involves well-coordinated, interdisciplinary care that avoids duplication and fragmentation (Council on Children with Disabilities and Medical Home Implementation Project Advisory Committee, 2014), promotes participation (Novak, 2014; Saleh et al., 2008) and is culturally appropriate and accessible to those with the highest needs (Spearing, 2008).
Physiotherapists play an integral role in best-practice paediatric care by promoting activity and participation and by providing non-pharmacological and non-surgical solutions to movement problems. Many of the processes of paediatric physiotherapy assessment and management, however, have their origins in the twentieth century, predating the evidence-based practice movement. Hence, it is possible that current practice does not sufficiently enable all dimensions of twenty-first-century best practice. For example, traditional paediatric physiotherapy practice is underpinned by developmental principles and a biomedical model focused strongly on the delivery of interventions that aim to ‘normalise’ movement patterns (Damiano, 2009; Law & Darrah, 2014; Wiart & Darrah, 2002). Further, these interventions are typically directed at management of impairments or symptoms, therapist-intensive and delivered with the child as a passive recipient of care (Law & Darrah, 2014). Modern paediatric physiotherapy practice is more holistic, using a biopsychosocial model and the International Classification of Functioning, Disability and Health (ICF) framework that includes greater consideration of activity and participation (Damiano, 2006; Escorpizo et al., 2010; Law, 2003; Law & Darrah, 2014; Lucas et al., 2016; Palisano et al., 2004; World Health Organization, 2001). Modern paediatric physiotherapy practice also focuses on empowering the patient and their family through well-structured self-management programmes that put less emphasis on traditional and more passive interventions (Law & Darrah, 2014). Evaluation of current physiotherapy services at the Clinic for Therapy Services will enable the development of a logic model for change that will facilitate redesign.
Redesign of health service delivery can be effectively facilitated by using a systematic and robust translational research framework. The Sax Institute (2016), in Australia, has developed a translational research framework that involves a series of steps for health services redesign, testing and implementation. These steps include, first, the idea generation phase, followed by testing of feasibility, efficacy, replicability and adaptability and then further testing for effectiveness, scalability and monitoring (Sax Institute, 2016). The ‘idea generation’ phase is an integrated, multidisciplinary and collaborative approach to inform the design of practice innovations (Sax Institute, 2016). This phase involves activities that explore current practice and barriers to best practice and utilises research designs such as clinical record audit and qualitative studies to obtain stakeholder perspectives (Sax Institute, 2016).
The aim of this study was, therefore, to examine the extent to which physiotherapy at the Clinic for Therapy Services enables best practice and to identify priority areas for service redesign. Specifically, we examined processes involved with clinical diagnosis, selection of interventions, parameters of the episode of care, formulation of therapy goals and selection of outcome measures. This study was the first in a series of ‘idea generation’ studies that will inform the development of a logic model for service adaptation, implementation and evaluation.
Methods
The study was a retrospective review of clinical records that was conducted in the paediatric section of the Clinic for Therapy Services, at the College of Allied Medical Professions, University of the Philippines Manila. The clinic uses a student-administered service model in which physiotherapy services are provided by senior undergraduate physiotherapy students under the supervision of registered physiotherapists. Service delivery was suspended at the clinic during a period of renovation and the COVID-19 pandemic. Records were reviewed from a period at which clinic services were at full capacity. The University of the Philippines Manila Research Ethics Board approved the study protocol (UPM REB code: 2014-503-01).
Records were retrieved from all children who received physiotherapy services from June 2011 to March 2015. A patient record was included if the child had at least one physiotherapy assessment during the study period and included children who have also received other allied health services. A data extraction form and manual were created prior to data collection to standardise extraction and coding by the researchers. Data extraction was pilot-tested using 10% of the included records and modified by consensus where disagreements arose.
Demographic and clinical characteristics were extracted from clinical records. These data included age, sex, place of residence, source of referral (public or private health sector), medical diagnosis, use of other allied health services and use of assistive devices.
The clinical diagnosis or therapist’s description of the child’s main presenting problem was categorised according to the ICF Child and Youth Version (World Health Organization, 2007). The ICF domain of Impairment comprised problems of body function and structure including bone and joint, muscle, cardiac and pulmonary systems, pain, sensory integration and others. The ICF domains of Activity Limitation and Participation Restriction comprised difficulties in relation to walking and moving, carrying and handling objects, movement control, self-care, play and environmental exploration, work and domestic roles and interpersonal interactions.
Interventions were categorised first as being active or passive. Active interventions were those that required action from the child and included a therapeutic exercise that targeted impairment of joint mobility, strength or motor control, as well as functional training and behavioural modification. Passive interventions included manual therapies and electrotherapies. The number of records with explicit self-management programmes was recorded. The prescription, application and fabrication of assistive devices were also recorded. Details of the episode of care were extracted including the duration (months), total number of therapy sessions provided and the initial frequency of appointments. The use of objective outcome measures N (%) was recorded both at baseline and on follow-up assessments. The outcome tool was categorised according to the measurement of impairment, activity, participation, quality of life and patient satisfaction.
Data were extracted independently by two researchers and compared for consistency. Inconsistencies were referred to a third researcher and resolved by consensus. Results were reported using descriptive statistics. The datasets used and analysed in the study are available from the corresponding author on reasonable request.
Results
Of the 429 records screened, 237 involved physiotherapy intervention and were included in the study. Baseline data were available from all 237 records. The median (IQR) age of participants was 4.4 (6.1) years, and 100 (42%) were female. Participants were mostly from Metropolitan Manila (n = 156, 66%), and the majority were referred to the clinic from the public hospital system (n = 171, 72%). The majority of participants (n = 229, 97%) had developmental conditions, most frequently cerebral palsy (n = 64, 27%), Down syndrome (n = 74, 31%), hydrocephalus (n = 57, 24%) or global developmental delay (n = 7, 3%). Approximately half of the participants (n = 135, 57%) received physiotherapy treatment only and did not use occupational therapy or speech pathology services. Only 21 (9%) of participants used assistive devices such as wheelchairs (n = 4, 2%), walking aids (n = 5, 2%) or other orthoses (n = 13, 6%).
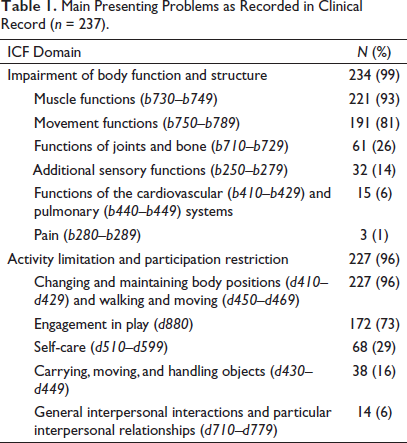
The majority of clinical records listed the presenting problems across multiple ICF domains with 232 (99%) listing impairments, and 227 (96%) listing activity limitations or participation restrictions (see Table 1). The most frequently reported impairments were related to muscle (n = 221, 93%) and movement (n = 191, 81%) functions. The most frequently reported activity limitations or participation restrictions were limitations in changing and maintaining body positions (n = 227, 96%) and engagement in play (n = 172, 73%).
Main Presenting Problems as Recorded in Clinical Record (n = 237).
Goals were reported in 236 (99%) of 237 records. The most commonly identified goals related to lower-level mobility skills (e.g., rolling, crawling, sit-to-stand transition) (n = 120, 51%), followed by ambulation (n = 118, 50%) and sitting (n = 111, 47%).
Active interventions were almost universally employed in the clinic (n = 236, 99%) with 236 (99%) receiving therapeutic exercise and 129 (54%) undergoing functional training and behaviour modification. Passive treatments were used infrequently (n = 38, 16%), with manual therapies used in 36 (15%) and electrotherapies in 4 (2%) cases. A small number of children (n = 12, 1%) were provided with assistive devices. Self-management plans appeared in 161 (68%) of the records. The duration of the episode of care was highly variable with a median (range) of 16 (1 to 139) months. The majority of participants (n = 230, 97%) commenced with weekly therapy sessions. The total number of treatments also varied considerably with a median (range) of 15 (1–150) sessions.
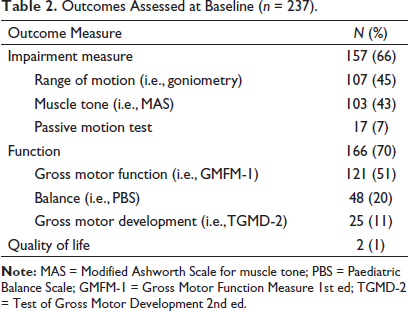
Objective outcome measurement was recorded in 209 of 237 (88%) records at baseline assessment (see Table 2), but in only 136 of 237 (57%) at one or more follow-up points. There was not a consistent time point for outcome assessment. For patient records that had data on re-assessment, time between assessment points ranged from less than 1 month to 36 months. Measurement tools for bodily impairments were recorded in 157 (66%) records. Functional measures were recorded in 166 (70%) records and a quality of life index in just 2 (1%) participants. No records had measures of participation or patient/family satisfaction.
Outcomes Assessed at Baseline (n = 237).
Discussion
This clinical record review demonstrated a need for more robust longitudinal management procedures, better mechanisms for tracking patient outcomes and recording of family input into goal setting and shared decision-making. In contrast, existing practices at the clinic in terms of the use of active interventions, promotion of self-management and focus on promoting activity and participation are well aligned with best practice. Practice guidelines and evidence implementation have traditionally focused on recommending or discouraging particular interventions. These results indicate that service redesign in this setting should focus more on aspects of service delivery rather than service content.
The patients’ journey through their episodes of care was difficult to track in the clinical records. There was considerable variability in the frequency, duration and total number of treatments provided, as well as inconsistency in time points and mechanisms for the evaluation of treatment outcome. A small number of children received more than 100 treatments over a period of several years, suggesting a poorly defined pathway of care. About half of the files had formal outcome assessment after an episode of care, and fewer used standardised outcome measures in these follow-ups. Better longitudinal management planning is, therefore, a priority of a redesigned service. There is a need for a more structured clinical pathway that formalises the planning of treatment goals, time frames, number of services, outcome assessment points and monitoring of change in patient outcomes and provision of care (De Bleser et al., 2006; Kinsman et al., 2010; Lawal et al., 2016; Renholm et al., 2002).
The extent to which caregivers were involved in goal setting and decision-making was not evident in the clinical records. Whilst about two-thirds of the records documented a self-management plan, caregiver involvement in programme design, the level of adherence and engagement with the interventions were not routinely recorded. Family-centred care needs to be collaborative and should involve the child and family in key aspects of decision-making and implementation (Dunst et al., 2007; Espe-Sherwindt, 2008; Ketelaar et al., 2001; King & Chiarello, 2014; Gorgon, 2018). Caregiver perspectives may be explored through qualitative methods to identify mechanisms to promote collaborative decision-making in this context. Further, a logic model for redesign of service delivery will need to consider formal processes for routine involvement of the child and caregiver in decision-making, and for recording these decisions to facilitate collaboration and family-centred care.
With improved levels of family input and family-centred care, a logic model for change might also consider a stronger focus on participation-level therapy goals and quality-of-life outcomes. Almost all of the clinical records had clear statements of the clinical diagnosis, expressed in terms of physical impairments or activity limitations. Prioritisation of the clinical problems and alignment with interventions and outcome measures, however, was difficult to establish. There was also the tendency for standardised outcome measures to be predominantly focused on impairment and activity limitation. This suggests a potential bias towards the physical dimensions of the disability and the need to explore how the impacts of psychosocial factors on the child’s life participation might be considered in aspects of care. Overall, there is a need for the logic model for change to integrate mechanisms for prioritising problems and checking the alignment of assessments, goals and interventions within the clinical pathway.
These results suggest good adoption of some principles of evidence-based practice by the university clinic particularly in relation to active and self-management approaches to rehabilitation. The interventions that were selected were predominantly active and directed towards improving function and participation, with minimal use of passive modalities. Active interventions that involve the patient and their family promote greater task practice to meet required therapeutic intensities and amount of training (Barbeau, 2003; Gannotti, 2017; Gannotti et al., 2014; Kleim & Jones, 2008; Novak, 2014), which cannot be achieved through passive interventions that are applied through infrequent clinic visits (Lucas et al., 2016; Novak, 2014). Active approaches are also more effective than traditional passive physiotherapy modalities (Booth et al., 2018; Clutterbuck et al., 2019; Damiano, 2006; Lucas et al., 2016; Martin et al., 2010; Preston et al., 2017), although these rely on patients remaining engaged with and adhering to self-management through an episode of care and beyond. Whilst a logic model for redesign will need to ensure that active approaches are carried through to a new service, this will not require substantial cultural or service delivery change in this setting.
This study evaluated service delivery in a specific local setting, namely, a tertiary teaching clinic in Metropolitan Manila, Philippines, for the purpose of informing adaptation of evidence-based practice in that local setting. It, therefore, was not intended that the results be generalisable to other physiotherapy clinics. It is possible, however, that the main theme of the need for reform of processes rather than the content of care might be common to other settings. The results provide a snapshot of current practice in this teaching and research facility. A deeper investigation of factors that influence practitioner decisions and an exploration of child and family perspectives through focus group discussions and interviews are planned for the next phase of needs assessment and idea generation.
Footnotes
Acknowledgement
We thank Professor Maria Concepcion Cabatan for providing critical comments to improve the research design during the research proposal drafting stage. We also thank the following individuals who assisted in records screening and data extraction: Stephanie Paige Abellera, Ayra Mae Balingbing, Maika Louise Bugante, Ma. Angelica Castro, Francesca Dalangin, Aaron James Gutay, Rachelle Angeline Lim, Raymart Macasaet, Faye Ann Medina, Christina Pauline Mostacho, Amanda Jessica Susulin, Jon Sergei Aclan, Jellen Agbuya, Timothy John Chua, Marian Pia Diaz, Julius Caesar Fernando, Ma. Cristina Gonzales, Sherwin Andrew Lucero, John Michael Mallari, Katrina Diane Puguan and Junielle Katrina Roxas.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This study was supported by a University of the Philippines Professorial Chair for Edward Gorgon and the Sydney Southeast Asia Centre Partnership Grant.