
Abstract
Patient safety, which is both an overarching principle and a key factor in determining the quality of healthcare, continues to be a priority in healthcare systems on a global scale. A cross-sectional study in accredited Indian hospitals aimed to evaluate the HSOPSC V-2 (Hospital Survey on Patient Safety Culture). 1,603 healthcare professionals participated, assessing psychometric features using confirmatory factor analysis in SMART PLS 4. The average composite positive response rate was 64.8%. High positive responses (79%) were seen in ‘teamwork’, ‘communication about error’, and ‘hospital management support for patient safety’. However, ‘staffing and work pace’ (30%), ‘response to error’ (50%), ‘communication openness’, and ‘reporting patient safety events’ (both 59%) had lower positive responses, indicating room for improvement. Findings suggest I-HOSPSC 2.0’s content validity, reliability, and construct validity in measuring patient safety culture in Indian hospitals. It can aid administrators in assessing safety culture and improving patient safety and treatment efficacy. Notably, this is the inaugural HSOPSC V-2 validation research in the Indian healthcare context. Future research should explore the tool’s psychometric properties based on care setting levels due to substantial differences between public and private healthcare setups in India.
Keywords
Introduction
Patient safety, which is both an overarching principle and a key factor in determining the quality of healthcare, continues to be a priority in healthcare systems on a global scale. It has been established that a culture of safety is one of the most important factors in ensuring the continued development of patient safety in the healthcare industry (World Health Organization, 2017). Safety culture is a collection of values, beliefs, standards and attitudes that are held in common by a group and that combine with the structure and control systems of an organisation to produce behavioural norms (Noort et al., 2015; Perrow, 2004). This component of organisational culture has an effect on the activities and behaviours of its members (Cox & Flin, 1998).
Despite the fact that numerous efforts have been made over the course of the past two decades to enhance patient safety and the quality of care, a sizeable proportion of patients continue to sustain injuries while obtaining medical treatment. The development of robust organisational safety cultures is a priority for today’s healthcare systems, which are focused on enhancing the level of patient care safety already available. It has been determined that ‘safety culture’ is an essential component of a healthcare organisation’s capacity to gain an open understanding of safety occurrences and to lessen the risk of avoidable injury to patients.
A lack of a strong safety culture is one of the factors that has been identified as contributing to dangerous patient care (Lee et al., 2017). There has been an increase in interest in the evaluation of safety cultures within healthcare organisations as a result of the perceived significance of safety culture in terms of both improving patient safety and its influence on clinical outcomes. Therefore, evaluating the safety culture is an essential step in the process of enhancing the quality of healthcare and protecting patients (Sorra et al., 2019a).
The culture of safety in healthcare institutions has been measured using a variety of different measures since their development. The Hospital Survey on Patient Safety Culture (HSOPSC), which was created by the Agency for Healthcare Research and Quality (AHRQ) in 2004, is the instrument that is used most frequently all over the world (Sorra et al., 2019a). The HSOPSC is a self-administered questionnaire consisting of 42 questions that evaluate the perceptions of hospital employees regarding 12 aspects of the safety culture of a healthcare organisation. The updated version of the survey, known as the HSOPSC 2.0, was made available by the AHRQ in 2019, and it contained 32 items distributed across 10 dimensions (Hellings et al., 2007). Many published studies still do not disclose the requisite psychometric features of questionnaires in sufficient detail (Flin, 2007; Nieva, 2003; Singla et al., 2006). In addition to being evaluated on the required large sample sizes, the HSOPSC is also believed to have good psychometric qualities, making it among the most rigorously studied instruments. Psychometric analysis is the application of recognised statistical assessment procedures in order to evaluate the psychometric qualities of questionnaires and determine the fundamental safety culture dimensions (Ito et al., 2011).
The AHRQ suggests using HSOPSC 2.0 rather than the previous version (Sorra et al., 2019a). So, the aim of this study is to evaluate the psychometric features of the HSOPSC 2.0 instrument in Indian hospitals.
Methodology
Study Design
A cross-sectional study was conducted to assess the content validity and other psychometric properties of the HSOPSC 2.0 in an Indian healthcare setting. The evaluation of the tool consisted of two phases. In Phase 1, the instrument was subjected to face and content validity from experts in the healthcare field. Phase 2 consisted of an investigation into both the instrument’s internal consistency and its construct validity.
Content Validity of the HSOPSC 2.0
HSOPSC 2.0 includes 32 safety culture factors tested on 5-point answer scales for agreement (strongly disagree to strongly agree) or frequency (never to always), in addition to ‘does not apply or do not know’. Two single questions ask respondents to rate their department’s patient safety on a 5-point scale (poor to excellent) and to record the number of patient safety incidents.
The English version of the HSOPSC 2.0 was modified so that it could be used in Indian healthcare. This was done to fix any technical and practical problems with its use.
Phase 1: HSOPSC content was evaluated by a panel of healthcare personnel in face-to-face interviews. Experts were requested to offer clarification recommendations for any points they found confusing. The responses from interviews were used to make small revisions towards the word choice, and the items were changed accordingly. The panel agreed that the HSOPSC material is very applicable to the safety culture in Indian institutions with minor modifications.
A team of five specialists was recruited to calculate the content validity index (CVI) for each individual item and the entire scale. The scale-CVI (S-CVI) was calculated by averaging each item’s CVI score, whereas each item’s CVI score (I-CVI) was generated from the proportion of experts who rated the item as 3 or 4, respectively. I-CVI scores more than 0.80 are deemed satisfactory, and S-CVI rates greater than 0.90 are regarded as exceptional (Polit & Beck, 2020). I-HSOPSC 2.0 produced I-CVI scores between 0.80 and 1.00 and an S-CVI of 0.935%, showing strong content validity. The CVR score for the I-HSOPSC instrument was 0.74, suggesting that all questions were required.
Phase 2: The sample size requirements for CFA were calculated based on the recommendations ratios of 5 to 20 cases per item (Furr, 2018). Thus, our sample size of 1,603 was deemed sufficient for obtaining a stable factor solution for the 32 items of I-HOSPSC 2.0. This research was approved by the Institutional Review Board of the relevant university and done in compliance with the World Medical Association Code of Ethics (Declaration of Helsinki).
Dimensions and Items of the Hospital Survey on Patient Safety Culture, Version 2.0, After Face and Content Validation.
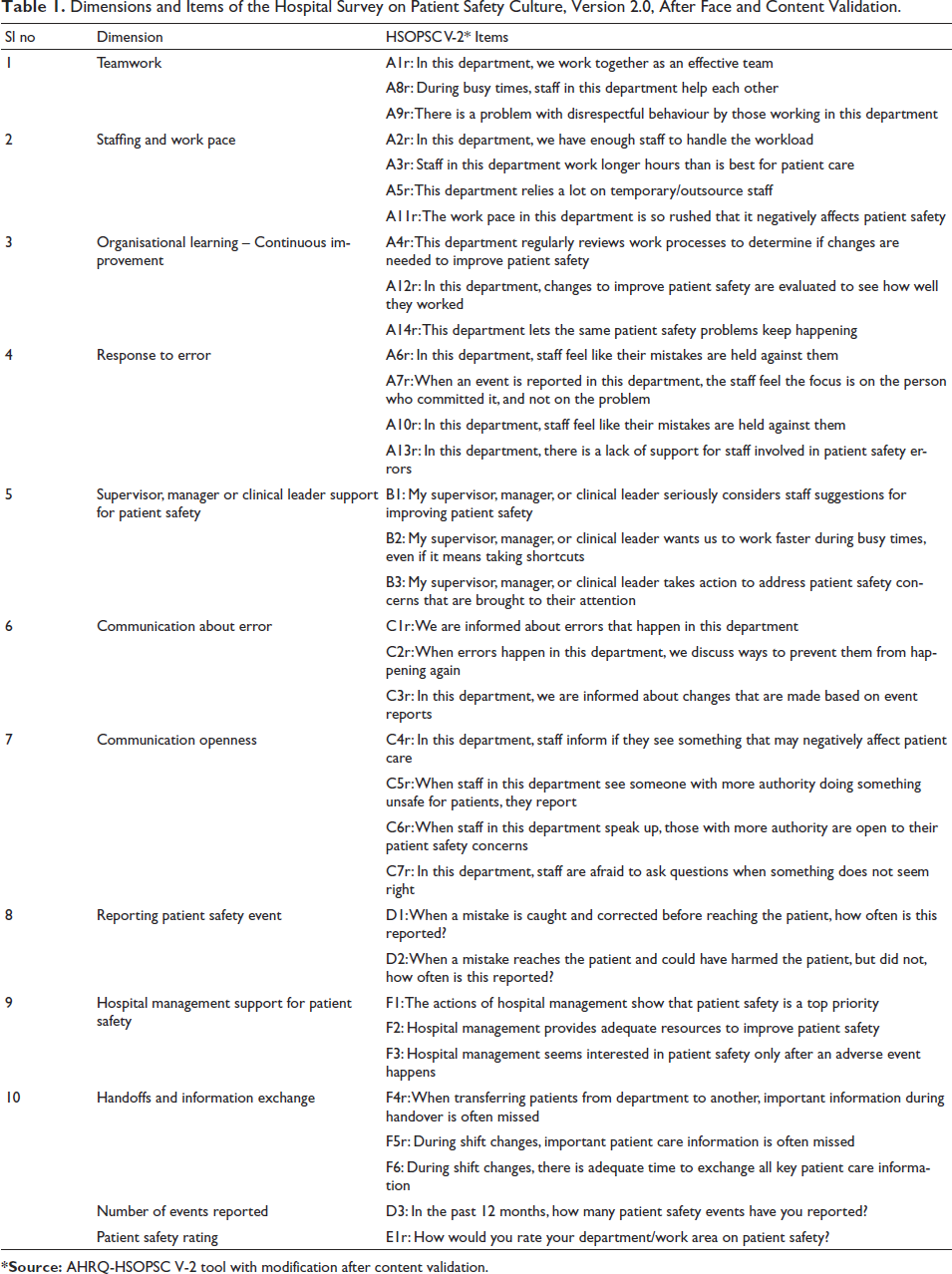
*Source: AHRQ-HSOPSC V-2 tool with modification after content validation.
Data Collection and Management
Healthcare personnel from various hospitals in India completed the online poll, totalling 1,603 voluntary healthcare professionals. Items with negative wording were reverse-coded. The information was encoded and entered into a digital data file.
To test internal consistency or reliability, Cronbach’s alpha was determined for each factor, with a minimum acceptable reliability requirement of 0.60, as recommended for the majority of research purposes (Bujang et al., 2018; Suhr, 2003).
The Kaiser–Meyer–Olkin (KMO) coefficient was utilised as an additional sample adequacy metric. KMO coefficient values vary between 0 and 1. Using SMART PLS 4 software, a CFA was conducted to verify the model fit of the HSOPSC 10-factor structure with Indian data (n = 1,603).
Data Analysis
All questionnaire items with negative wording were recoded. The descriptive statistics for participant characteristics and I-HOSPSC 2.0 subscales were calculated. The percentage of positive replies for each subscale was calculated to compare the present study and the original U.S. survey (Sorra et al., 2019b). We calculated the mean percentage of respondents who replied ‘strongly agree’ or ‘agree’ or ‘always’ or ‘most of the time’ for favourably written items and ‘strongly disagree’ or ‘disagree’ or ‘never’ or ‘rarely’ for negatively worded items. Each subscale’s internal consistency was assessed using Cronbach’s alphas, with 0.7 being the lowest acceptable dependability (Nunnally & Bernstein, 1994). The factor structure of the I-HOSPSC 2.0 was examined through CFA using SRMR and NFI fit indices (Chua, 2022).
Results
Participants’ Characteristics
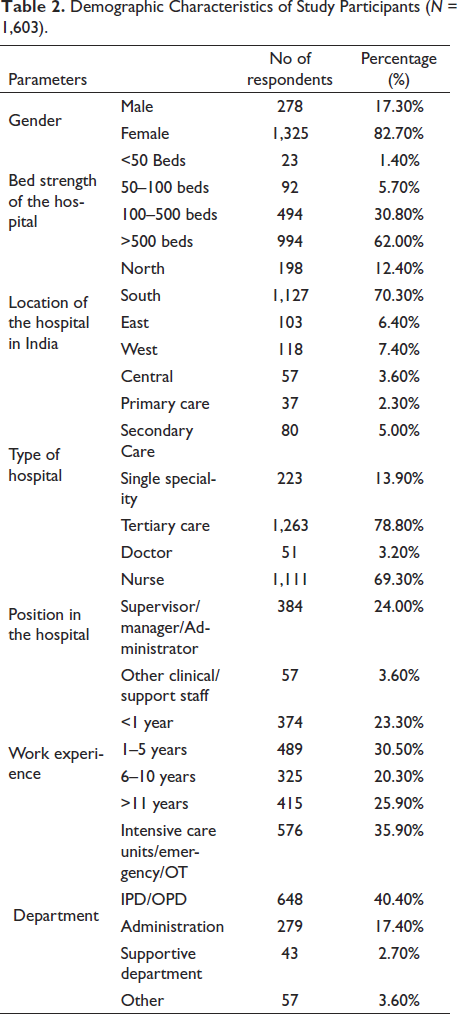
As shown in Table 2, 82% of the 1,603 participants were female. The majority (62%) of the responses were from hospital settings with more than 500 beds, and the majority was from South India (70%). On average, participants had 1 to 5 years of experience (30%) and had worked in the hospital in the inpatient or outpatient department (40%).
Demographic Characteristics of Study Participants (N = 1,603).
Reliability Statistics and the Positive Response Rate of Patient Safety Culture
Table 3 presents the Cronbach’s alpha and percentage of positive responses for the I-HSOPSC 2.0. Compared to the results from the original U.S. study (Sorra et al., 2019b), Indian healthcare professionals reported similar safety culture scores for each subscale except for staffing and work pace, which were lower than the original study scores, and hospital management support for patient safety, which was higher than the original study. Table 3 also shows that Cronbach’s alphas for all subscales were greater than 0.70, with the exception of handoffs and information exchange (0.45).
Reliability Statistics and the Positive Response Rate of Patient Safety Culture.
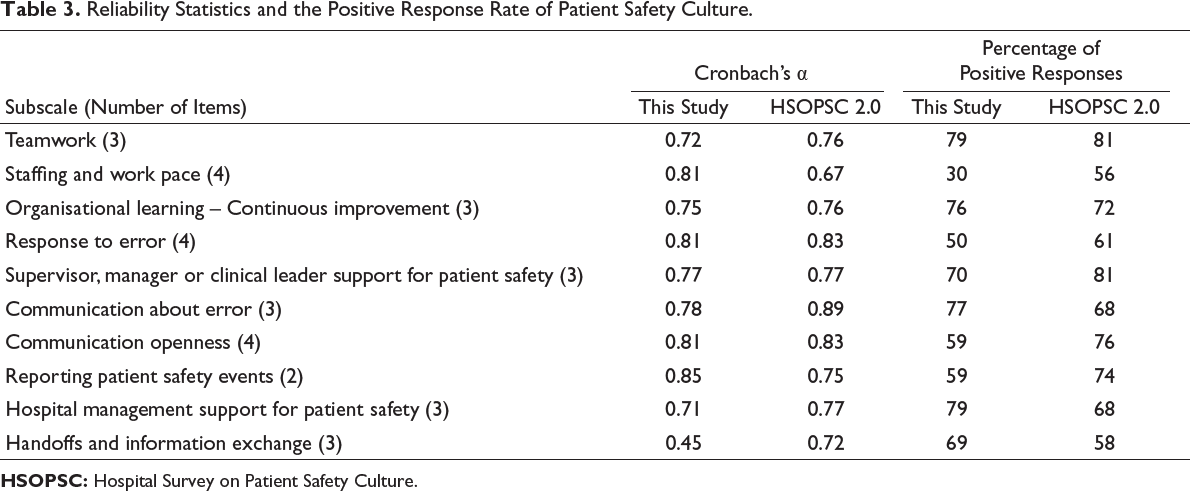
Results revealed that average composite positive response rate was 64.8% (Table 3). The dimensions ‘teamwork’, ‘communication about error’ and ‘hospital management support for patient safety’ showed the highest positive responses (79%, 79% and 77%, respectively). The dimensions such as ‘staffing and work pace’, ‘response to error’, ‘communication openness’ and ‘reporting patient safety events’ showed low positive responses (30%, 50%, 59% and 59%, respectively) and had scope for further improvement.
Confirmatory Factor Analysis Results
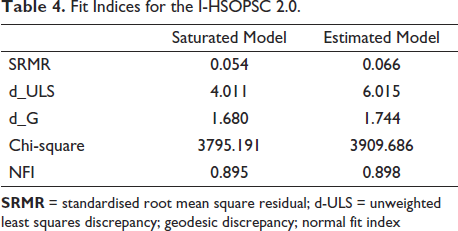
All items within each factor had factor loadings greater than 0.5, ranging from 0.85 (Mehmetoglu & Jackobsen, 2017). SRMR = 0.054 and NFI = 0.895, as shown in Table 4, suggest that the 10-factor model offered a satisfactory fit to the data with threshold values of approximate fit indices such as SRMR and NFI (e.g., SRMR = 0.08 and NFI > 0.90) (Henseler et al., 2014). The d_ULS and d_G variables have no inherent significance. Validation of the factorial structure of an instrument is one sort of evidence crucial to proving the construct validity of an instrument (Hair & Alamer, 2022; Rönkkö & Evermann, 2013; Tenenhaus et al., 2004).
Fit Indices for the I-HSOPSC 2.0.
Discussion
Numerous studies were conducted outside of India that confirmed the factor structure of the HSOPSC instrument and identified a number of variables that are applicable to those nations. An examination of the Japanese version demonstrated a reasonable level of congruence with the core instrument’s factor structure and the patient safety culture was mainly dependent on the unit of their work (Fujita et al., 2014). In contrast, a UK study’s confirmatory factor analysis found a poor fit, prompting the researchers to advocate a small reorganisation of the factor model (Waterson et al., 2010). It is conceivable that different healthcare environments contain substantial variations, which would diminish the instrument’s validity and effectiveness. According to these findings, such and other safety culture measures require substantial testing before they can be widely utilised or before conclusions can be reached regarding their applicability in countries or circumstances other than those for which they were designed.
In this study, the psychometric features of the HSOPSC 2.0 instrument were evaluated in the Indian healthcare system. Internal consistency, content validity and construct validity were all good, indicating that the I-HSOPSC 2.0 can be used to measure the perceptions of patient safety culture among healthcare professionals in Indian hospitals. A similar study was conducted in Korea using HSOPSC V-2 and 10-factor model provided an acceptable fit to the data: χ2/df ratio = 2.51 (χ2 = 978.37, df = 389, p < .001), RMSEA = 0.05, SRMR = 0.06 and CFI = 0.89 (Lee & Dahinten, 2021).
In the present study, the internal consistency coefficient for the 3-item handoffs and information-sharing subscale was 0.45; the subscale’s alpha value in the American version was 0.72. Despite the fact that the subscale did not meet the 0.70 level proposed by Nunnally and Bernstein (1994), it was nonetheless statistically significant. Our findings therefore justify the removal of subscale handoffs and information exchange from the HSOPSC 2.0 for usage in Indian hospitals. Cronbach’s alphas for the remaining nine subscales varied from 0.71 to 0.85, indicating each subscale’s excellent internal consistency.
The CFA results for the instrument’s 32 components supported the 10-factor structure of the HOSPSC 2.0. Each item contributed to the anticipated subscale, demonstrating construct validity. In addition, as expected, all subscales were related to patient safety grade, providing additional support for the construct validity of the I-HSOPSC 2.0.
Comparing our results to those of the U.S. study (Sorra et al., 2019b), Indian healthcare professionals assigned fewer positive values to seven elements of patient safety culture and comparatively high scores to three others (organisational learning and continuous improvement, communication about errors and hospital management support for patient safety).
The present study findings revealed that the response rate in dimension of ‘teamwork’, ‘hospital management support for patient safety’ and ‘communication about error’ showed the highest positive responses. The dimensions of ‘staffing and work pace’, ‘response to errors’, ‘reporting patient safety events’ and ‘communication openness’ had received the least positive responses. These findings are in congruence with the studies conducted in India using HSOPSC V-1 (Meena & Shetty, 2021; Rajalatchumi et al., 2018).
In addition, the Indian government should re-evaluate the national guidelines for minimum staffing levels and monitor hospital compliance.
This study’s findings support the utilisation of the I-HOSPSC 2.0 for examining the patient safety culture in Indian hospitals. This instrument can aid hospital administrators in identifying areas for enhancement in order to increase patient safety and care quality. With this instrument, hospital managers would be able to compare their results to those of other departments, hospitals and nations; to date, such evaluations have been limited because of the lack of a valid and reliable instrument for measuring patient safety culture in India.
Limitation
Besides the fact that our study provides evidence of the reliability and construct validity of the I-HSOPSC 2.0 for measuring patient safety culture in Indian hospitals, it is important to emphasise that there are certain limitations. First, the majority of respondents in this survey were female and worked in tertiary care facilities. Hence, the results may not be representative of all healthcare practitioners and cannot be extrapolated to other healthcare settings. Future studies should examine the psychometric features of this instrument within a broader validation framework. Second, the poll was distributed online, and there is evidence of administration bias. Third, to the best of our knowledge, no papers have been published that explore the psychometric features of the HSOPSC 2.0 in an Indian context; hence, we were unable to compare our results to those of other published studies of the instrument.
Conclusion
Our findings give preliminary evidence of the instrument’s internal consistency, content validity and construct validity, based on data from Indian hospital healthcare professionals. Our CFA results specifically support the utilisation of the 32-item, 10-factor I-HSOPSC 2.0. Nonetheless, additional study is needed to look into its psychometric features in a wider context of validation.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.