
Abstract
International comparison of health systems performance provides evidence to countries, policymakers and decision-makers. This study was conducted in order to rank and compare the health systems performance levels of the Organization for Economic Development and Cooperation (OECD) countries according to the determined health performance indicators. In the study, the data of the countries between the years of 2000–2017 were used and evaluated. The study consists of 36 member countries of the OECD. The data was analysed with the MOORA (Multi-Objective Optimization on the basis of Ratio Analysis) method, which is one of the multi-criteria decision-making methods, allowing the comparison of the performance of health systems across countries is compared. As a result of the health system performance evaluations of OECD countries. As a result of the health system performance evaluations of OECD countries, it has been concluded that countries such as Switzerland, Germany and Sweden have a high level of health systems performance, and Mexico, Colombia and Turkey have a lower performance compared to other countries. It is expected that countries with lower health system performance levels due to health system structures, demographic characteristics, education levels and technological development levels can still develop by selecting alternative countries suitable for their purpose and adopting the policies and strategies of such countries to their own systems.
Keywords
Introduction
Policymakers must be responsible to individuals and ensure the effective and efficient use of resources provided to health systems (Paoli et al., 2019). Evaluation of the performance of health systems has become an important tool for the evidence-based approach (Blümel et al., 2020) and in many respects (Mahdiyan, 2020; Noto et al., 2019; Smith et al., 2009). Evaluation of health systems is important to inform policymakers and to highlight inequalities between different societies as well as to improve health systems. Comparing healthcare systems is challenging because the healthcare industry frequently provides various results (Schütte et al., 2018). Despite various structural differences and inequalities, many countries share common health system goals and face similar challenges (Fekri et al., 2018; WHO, 2000). At this point, international comparisons can be a reference source for countries to achieve the goals they set for the improvement of their health systems (Cylus et al., 2017; Nolte et al., 2006; Papanicolas & Smith, 2013; Suhrcke et al., 2006).
Over the past two decades, some international organisations have conducted various studies in order to assess the performance of healthcare systems and create international comparisons (Arah et al., 2006; European Commission, 2014; OECD, 2015; WHO, 2000). For example, the World Health Organization (WHO) published a ranking in 2000 to assess the performance of member nations’ health systems. The Organization for Economic Development and Cooperation (OECD) and the European Commission have developed a conceptual framework for assessing health system performance. In addition to international organisations, some countries have developed and compared conceptual frameworks for health system performance (Hurst & Jee-Hughes, 2001). Schieber et al. (1994) compared the United States’ healthcare system to those of other developed countries and developing countries. Anderson and Hussey (2001) used some indicators to examine the data on the performance of 29 nations’ health systems. Tchouaket et al. (2012) evaluated the health systems performance of some OECD countries and tried to distinguish the homogeneity of performance levels. Braithwaite et al. (2017) defined and compared the frameworks and performance indicators used in some OECD countries to measure and report the performance of health systems. Arah et al. (2003) examined the dynamics of the conceptual framework for health system performance, as well as its effectiveness and performance indicators. In a study conducted by Schoen et al. (2005), it was shown that negative patient experiences with healthcare systems put more pressure on decision-makers from other countries to seek alternative policy options.
Comparing the performance of the health system is a fundamental prerequisite for assessing progress and planning a way to proceed (Sharma et al., 2018). When making comparisons, a cautious approach should be adapted since efforts based on insufficient and biased policies can have a serious policy and political consequences (Papanicolas & Smith, 2013). In order to evaluate and compare the performance of countries, measurable and reliable indicators and methodologies derived from a competent information system are required (Hurst & Jee-Hughes, 2001). Performance indicators serve a variety of purposes, including facilitating measurability, frequently monitoring health systems, monitoring the behaviour of health professionals and organisations on a macro and micro scale, and directing policymakers (Arah et al., 2003; Kruk & Freedman, 2008; OECD, 2015; Smith et al., 2009). Traditionally, monitoring of developments in the health system and performance evaluation efforts have focused on such indicators (Jordans et al., 2016). While determining these indicators, it is necessary to take into account the effects on health service users and the structures, functions and outputs of health systems. Determined performance indicators should also have a great impact for health systems and should represent health systems performance (Arbour et al., 2009; Kruk & Freedman, 2008; Rowe et al., 2008). Despite the large number of national and international studies, methodological problems related to health system performance indicators continue to be discussed (Bankauskaite & Dargent, 2007).
Health systems performance has been limited by certain performance characteristics such as service quality, service access and service cost in various theoretical frameworks. Current methodologies and their limitations require a new search for assessing healthcare systems (Romaniuk et al., 2018). In particular, the lack of a comprehensive data collection tool and the lack of standard indicators that define the overall performance are among the main topics discussed (Fekri et al., 2018).
Performance measures can be used to guide consumer preferences, meet needs, and implement best practices for continuous improvement (Pransky et al., 2001). Factors such as the increase in the elderly population and the frequency of chronic diseases, new and developing medical technology, the increase in the demand and expectations of health services, and the more widespread use of information in today’s world have brought along the necessity of measuring and improving the performance of health systems (McLoughlin et al., 2002). Comparing the performance of healthcare systems may be an effective instrument for policymakers in accomplishing their objectives (Shari et al., 2017). It offers the opportunity to explore new options for mutual learning and formulating an effective national health policy (Fekri et al., 2018). Excluding the WHO (2000) study, literature which ranks nations’ health system performance is rare (Schütte et al., 2018; Sharma et al., 2018).
The aim of this study is to evaluate the health systems performance of 36 OECD member countries based on selected health indicators.
Methods
The study measures the performance with a Multi-Objective Optimization on the basis of Ratio Analysis (MOORA), one of the multi-criteria decision-making methods, and ranks the countries’ performance in order to investigate the relationship between indicators and the performance of healthcare systems.
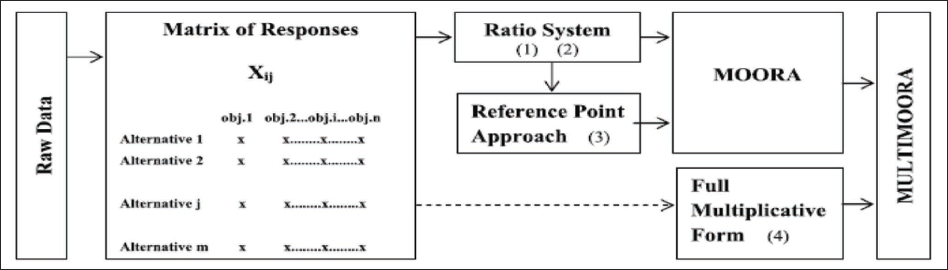
Brauers and Zavadskas (2006) described their method as multi-objective optimisation of many alternatives. When compared to other multi-criteria decision-making methods, MOORA is said to have a high level of reliability (Brauers & Zavadskas, 2012; Chakraborty, 2011; İç, 2020; Kıyıcı et al., 2016). There are studies in the literature that use different approaches such as the ratio method, reference point approach, importance coefficient and full multiplicative form (Karande and Chakraborty, 2012) (Figure 1). In general, the ratio method and the reference point approach are used together, but some studies use just one method (Kalibatas & Turskis, 2008).
Diagram of MULTIMOORA (Brauers & Zavadskas, 2012).
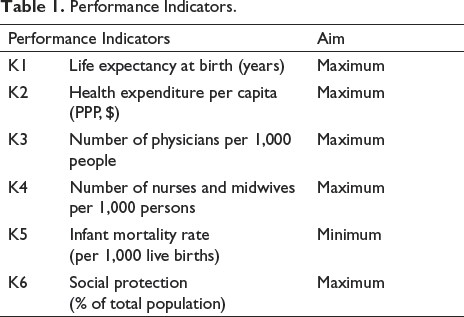
In this study, the health system performance of OECD countries between 2000 and 2017 is ranked by using the ratio method and reference point approach together. Performance indicators indicate quantifiable value by taking into account several factors to assess the degree of performance (Parida & Kumar, 2006). There is no widely accepted standard evaluation method in the literature for assessing the criteria influencing the performance of health systems (Fekri et al., 2018; Schütte et al., 2018; Sharma et al., 2018). For this reason, studies that evaluate health system performance and the conceptual frameworks created are taken as reference when determining performance indicators (Arah et al. 2006; Blümel et al., 2020; European Commission, 2014; Noto et al., 2019; OECD, 2009; Romaniuk et al., 2020; WHO, 2000, 2007). Table 1 presents the indicators selected to evaluate health systems performance. In high-performing health systems, infant mortality rate is expected to be minimum and life expectancy at birth to be maximum (WHO, 2000). Taking these two indicators as reference; In order to determine the maximum or minimum desired values of other indicators, to determine their effects on each other, and to ensure that the research results are more accurate and reliable, correlation analysis was performed and objective functions were created according to the results.
Performance Indicators.
Every year, the OECD gathers and frequently provides statistical data on its member and partner nations. The collection of data by the OECD according to certain standards allows comparative performance measurement studies (Afonso & Aubyn, 2005). Since the data standard and quality are thought to be high, the population of the study was determined as 37 OECD member countries. Luxembourg was not included in the study because there were missing values in the indicators used in the study. The study comprised 36 countries, and analyses and assessments were performed on these countries. There were some deficiencies in the data obtained from OECD member countries between the years of 2000–2017. In order to rectify this situation, in cases were information was unavailable for a specific year data from the most recent year was used. Although it is an undesirable situation, a solution can be produced this way in order to complete the deficiencies in the data set (Moran & Jacobs, 2013). The data on the health systems performance indicator variables used in the research were sourced from the data in the OECD database, which contains many data belonging to OECD members, and the World Development Indicators (WDI) databases of the World Bank, which allow countries to be compared. The number of physicians per 1,000 people and the number of nurses and midwives per 1,000 people were obtained from the WDI database because there was more missing data in the OECD database. It provides separate data for physicians (practitioners, etc.) and also provides data on the number of nurses and midwives in specific breakdowns. Data management and analysis were performed using Excel 2016.
Ratio Method
I = 1,2,3,…,m represents the number of alternatives, j = 1,2,3,…, n represents the number of criteria. The normalisation process (Equation 1) is performed by dividing the sum of the squares of each alternative by the square root of the criteria.
xij is the response of alternative j to objective Ii, j = 1, 2,…,m; m the number of alternatives, i = 1,2,…, n; n the number of objectives.
Following this, performance criteria are established depending on the objective functions (maximum or minimum). For optimisation, these responses are added in case of maximisation and subtracted in case of minimisation. In other words, Equation (2) is applied to the criteria to maximise j = 1,2,…,g and to minimise j = g + 1, g + 2,…,n (Brauers & Ginevicius, 2010);

According to the ratio method, performance ranking is obtained by ranking the
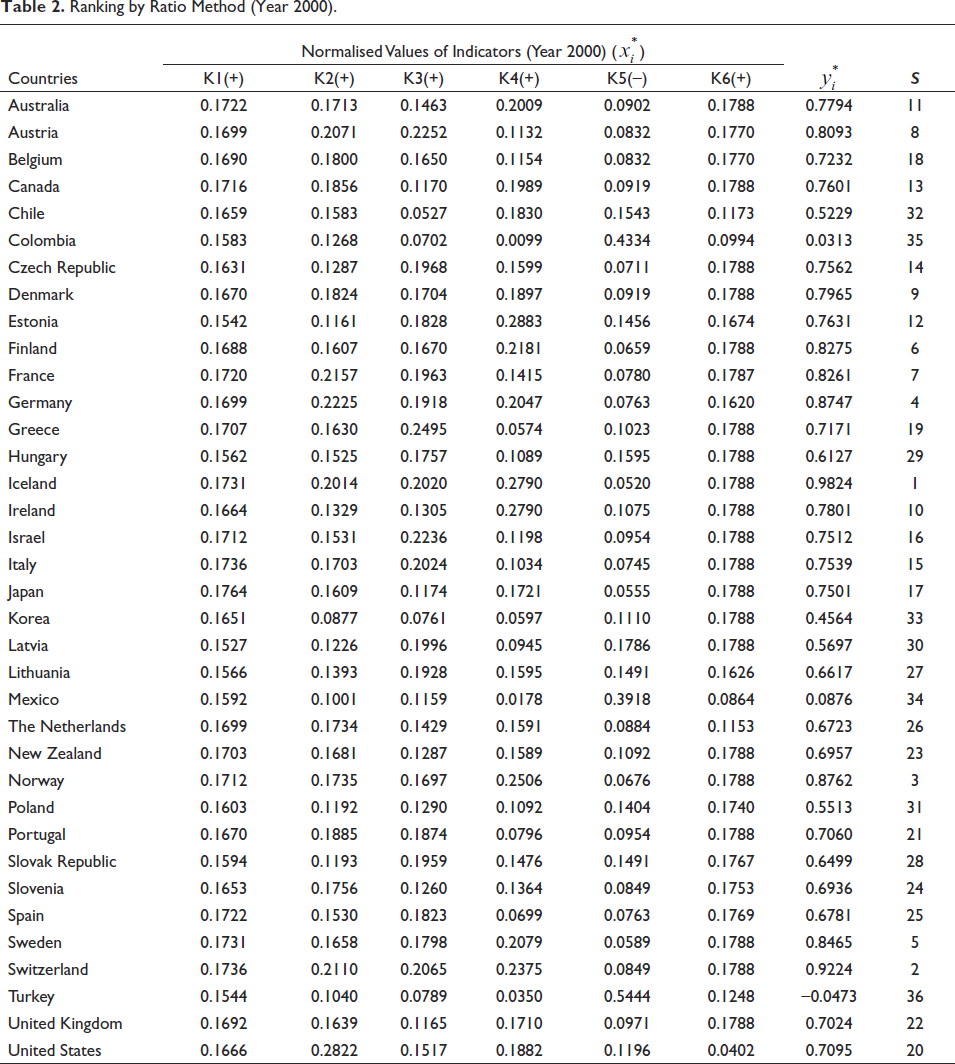
Table 2 shows an overview of the ranking of the health system performances obtained by using the steps of the ratio method of the data of the 36 OECD member countries for the year 2000. The ratio method summed the values for which the maximising of the normalised values obtained for the criteria was expected and subtracted the values for which the minimisation was intended from this total. The result obtained represents the performance score. The country with the highest score was determined to have the highest healthcare system performance, and a ranking was constructed from highest to lowest. It can be seen from the data in Table 2 that the top three countries are developed countries such as Iceland
Ranking by Ratio Method (Year 2000).
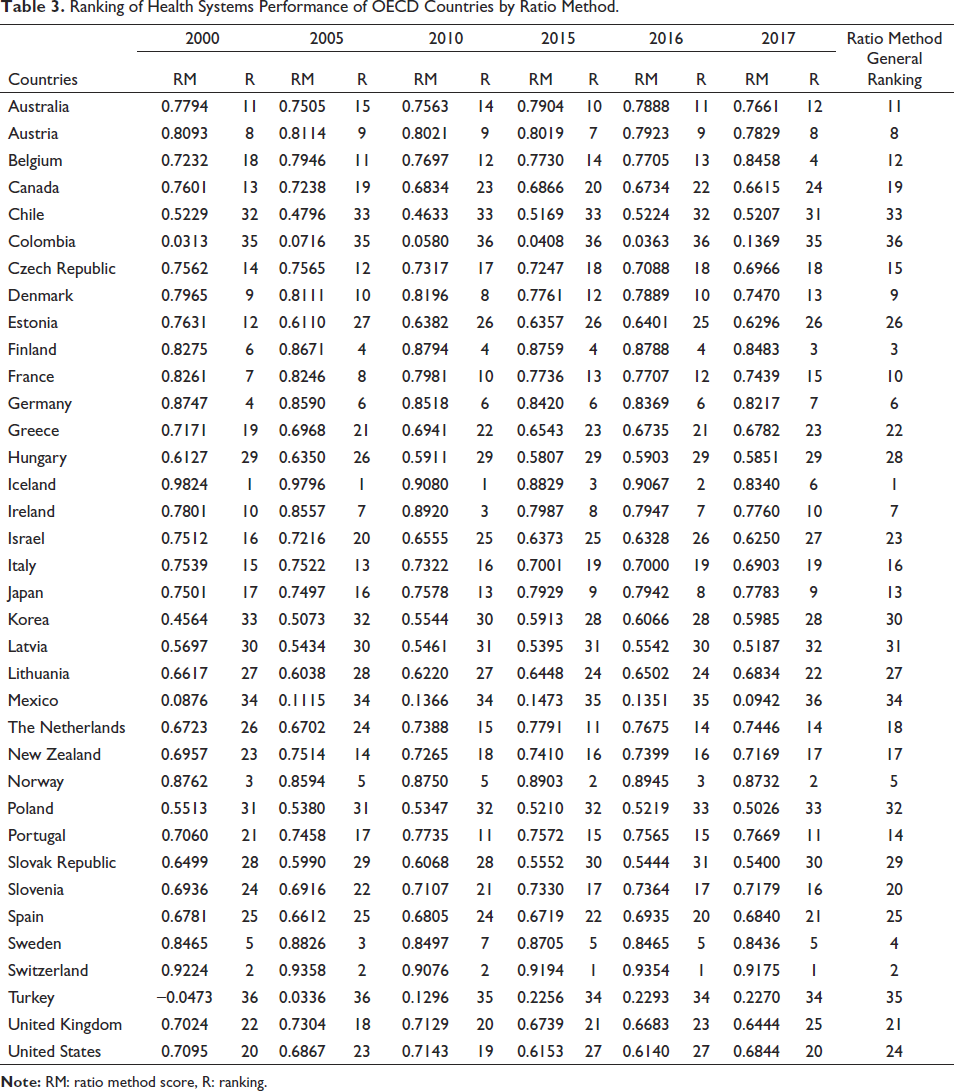
The rankings of some of the other years (2001–2017) evaluated according to the ratio method are given in Table 3. The entire table is presented in Suppl Appendix 1. Table 3 shows that Iceland had the best performance between 2000 and 2010. While Switzerland had the second-best performance until 2010, its health system has become the best country on a yearly basis since 2015. Iceland and Switzerland are followed by Norway, Germany, Switzerland and Finland. Determining the overall ranking, Iceland is the country with the best health performance. Switzerland is in the second place, Finland is in the third place and Sweden is in the fourth place. The USA ranks 24th despite being the country with the highest health expenditure. Mexico, Turkey and Colombia make up the last three places.
Ranking of Health Systems Performance of OECD Countries by Ratio Method.
Reference Point Approach
In addition to the ratio method, the reference points (rj) are determined for each criterion in the reference point approach. If the aim is maximisation, the maximum points, and if the aim is minimisation, the minimum points are determined. Equation (3) is used to measure the distances between these determined points for each

The ‘Tchebycheff Min-Max Metric’ (Equation 4) function is used on the newly created matrix to obtain the data for sorting.

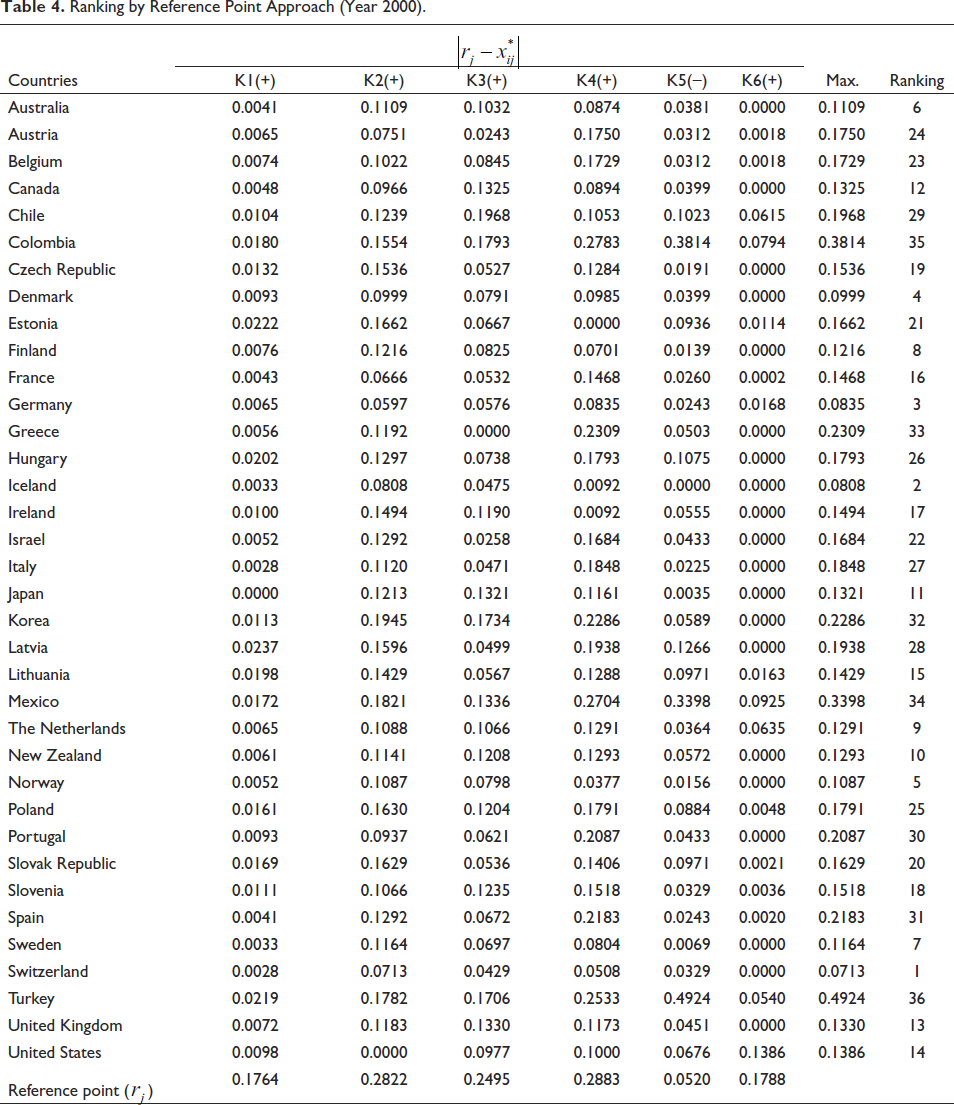
Table 4 illustrates the ranking of health system performance for the year 2000 according to the reference point approach of 36 OECD member countries. From Table 4 it is seen that Switzerland (Max.= 0.0713), Iceland (Max.= 0.0808) and Germany (Max.= 0.0835) are the top three countries in the 2000 performance ranking. As in the ratio method, Mexico (Max.= 0.3398), Colombia (Max.= 0.3814) and Turkey (Max.= 0.4924) are in the last three places. The same steps were applied to the data between 2001 and 2017 and performance scores were obtained according to the reference point (Suppl Appendix 2).
Ranking by Reference Point Approach (Year 2000).
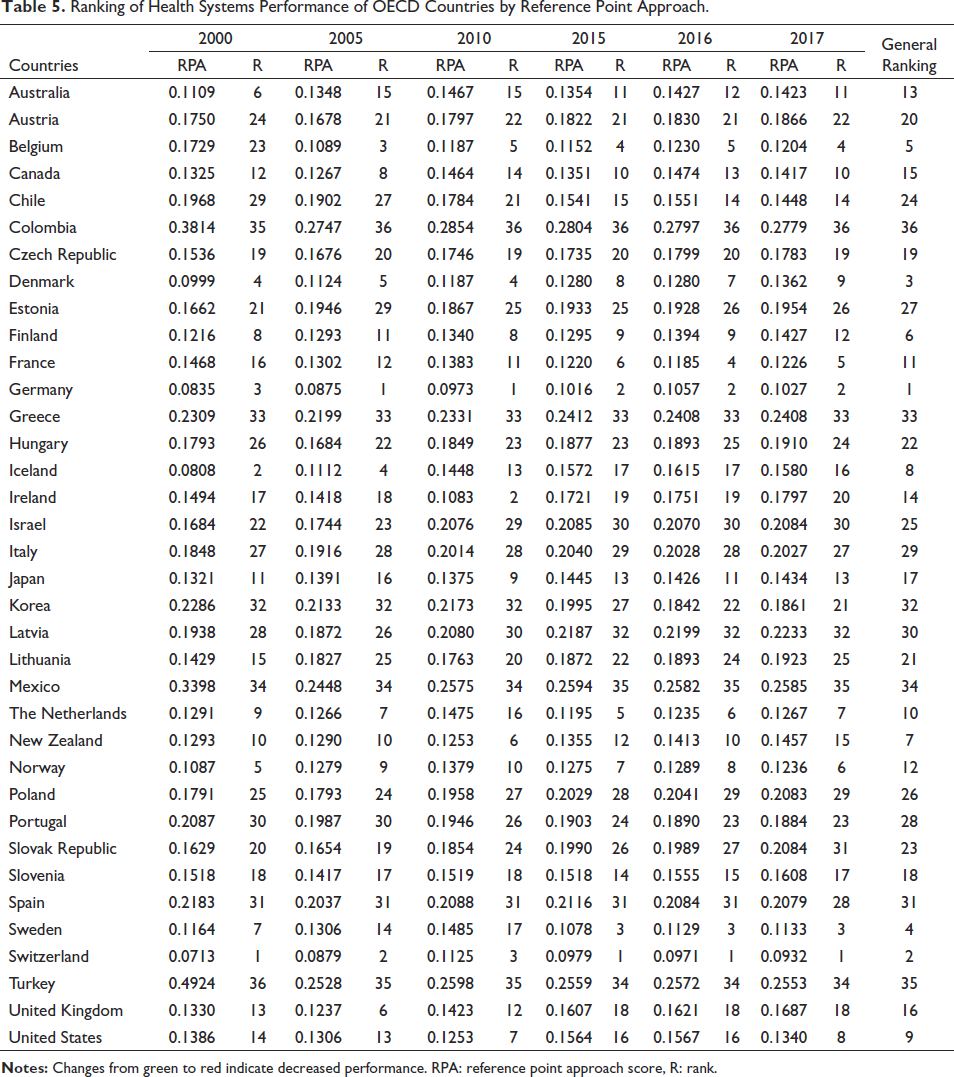
The rankings of some of the other years (2001–2017) evaluated according to the reference point approach are given in Table 5. The entire table is presented in Suppl Appendix 2. Germany has become the country with the best performance between 2005 and 2014. It can be seen from Table 5 that Switzerland is in first place in the last three years. Switzerland has alternated between first and fourth place in the performance rankings. While Iceland was in first place in the early 2000s, it showed a serious decline after 2010. By 2017, Iceland (Max.=0.1580) regressed to 16th place in the ranking. As in the ratio method, Switzerland, Germany and Iceland are followed by developed and developing countries such as Denmark, Norway and Australia. When the changes of the countries between the years are examined, it can be said that there are no serious ranking changes.
Ranking of Health Systems Performance of OECD Countries by Reference Point Approach.
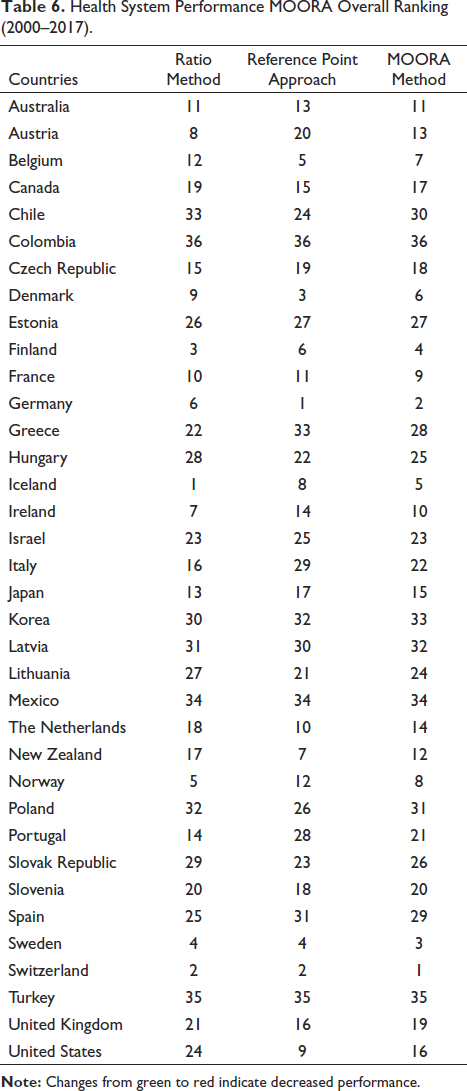
In order to obtain the general ranking, the results obtained from the rankings of the countries between the years 2000–2017 were used and a new ranking was created in Table 6. As shown in Table 6 the overall ranking, Switzerland has the best healthcare system performance. Germany is ranked second, Denmark is ranked third and Sweden is ranked fourth. Mexico, Turkey and Colombia are in the last three in the ranking.
Health System Performance MOORA Overall Ranking (2000–2017).
Discussion
The health level of developed countries is higher than that of developing or undeveloped countries. However, it is very difficult to infer which country’s health system has the highest performance. Performance needs to be evaluated according to worst and best under certain conditions (WHO, 2007). In this study, the performance of 36 OECD member countries’ health systems was assessed using several health indicators. With MOORA, one of the multi-criteria decision-making methods, the performance of health systems was measured and the performance of the countries were ranked. When studies evaluating health systems performance are examined, very few studies using multi-criteria decision-making methods have been found. The study differs from the studies conducted in the field of health systems performance with the method it uses. In this respect, it is thought that the study will contribute by expanding the existing literature.
The performance score of the health systems performance of 36 OECD member countries between 2000 and 2017 was obtained using the ratio method and reference point approach. When the health system performance rankings of the countries are examined, it is seen that the top 10 countries with the best health system performance are Switzerland, Germany, Sweden, Finland, Iceland, Denmark, Belgium, Norway, France and Ireland, respectively. It has been determined that Poland, Latvia, Korea, Mexico, Turkey and Colombia perform poorly in comparison to other countries. In reviewing the literature, studies comparing health systems using different techniques support our findings (Hejduková & Kureková, 2017; Mackenbach & McKee, 2013; Tchouaket et al. 2012). It is also seen that there is a similarity between the findings of our study and the Human Development Index (HDI, 2020) report which states that countries such as Norway, Ireland, Switzerland, Iceland, Sweden, Australia, The Netherlands and Denmark are among the top 10 countries. While obtaining the development ranking of the countries, indicators such as life expectancy at birth, years of education and income are used. These findings also support the concept that the performance of health systems should be assessed with the performance of other systems such as education and the economy, and that these systems might have an impact on each other directly or indirectly.
When the indicators of the countries with low performance are examined, it is seen that the infant mortality rate is high and the health workforce is below the average compared to other countries. There are several possible explanations for this result. According to WHO (2007), health manpower is the workforce that works efficiently to achieve the best health outcomes given the available resources and conditions. A sufficient number of qualified health workers is a critical tool for ensuring the performance of healthcare systems. In order to access quality health services, a sufficient and qualified health workforce is needed (Chen et al., 2004; Hongoro & McPake, 2004). Life expectancy at birth is longer in developed countries than in underdeveloped and developing countries. Among the most important reasons for this is the investment in health manpower. These investments both enable the use of advanced medical technology and reduce the number of people per healthcare worker (Beck & Webb, 2003). Anand and Bärnighausen (2004) found that the decrease in the infant mortality rate of the health workforce was significantly explained in their analysis. According to Speybroeck et al. (2006), countries with higher total health manpower had improved health outcomes. Or (2001) emphasises that the number of physicians per capita is the second most important variable for both perinatal and infant mortality. When considered in this context, it is thought that countries such as Mexico, Turkey and Colombia should develop policies that will increase their health workforce. Romaniuk et al. (2020) state that there is a correlation between per capita health expenditures and health outcomes. Countries allocate a significant share of their national income to health systems. The ratio of health expenditures to the total share in OECD countries is around 9% (OECD, 2021). In our study, although the per capita health expenditure of the USA is much higher than that of other countries, it was seen that the performance of health systems is at an average level (16th). In the study conducted by Squires and Anderson (2015), the health system performance of the USA was found to be low compared to other countries. In the report by the WHO (2000), which compared the health systems performance of 191 countries, it was reported that the performance of the USA was moderate. The present results are significant in some major respects. A possible explanation for this might be that this has been associated with the widespread use of medical technology and higher-cost healthcare delivery.
Conclusion and Recommendations
Evaluating and improving health system performance has become an important policy issue in many developed and developing countries. International comparisons have an important potential driver for health system improvement. Measuring and evaluating health systems performance provides countries, policymakers and decision-makers with evidence for improvement. When assessing the performance of healthcare systems, various indicators are considered. The purpose of the indicators is to change the behaviour of health professionals and organisations at both macro and micro levels and to guide policymakers.
These findings may help us understand that the effective and efficient use of investments in health may increase the performance of the health system. Health workforce, access to health services, health expenditures increase the health status of countries. At the macro level, the health system structure, demographic characteristics, education level, economic structure, technological development level, etc. of countries with low health system performance can develop as a result of adapting the policies and strategies implemented by those countries with high health system performance to their own systems. Examples of high performance in other countries are expected to encourage lower-income countries to make similar attempts and contribute to collaborative learning through the use of performance statistics. In this way, countries have the opportunity to develop strategies and policies based on evidence and statistical data.
In order to increase the performance of health systems, countries need to increase life expectancy at birth. To that end, it is recommended to expand activities such as healthy nutrition, counselling, education, public health training on the management of chronic diseases, professional support, home care services, cancer screenings, physical activities and similar activities to develop a healthy life culture. Improvements should be made to ensure adequate financing for health expenditures and to increase productivity. However, investments in health should be made in line with needs. The effectiveness of science and advisory boards should be increased, and the financial knowledge level of health managers should be increased. Cooperation should be made with health institutions and universities for health workforce, and improvements should be made regarding the working and living conditions of health personnel. In order to reduce the infant mortality rate, the number of health personnel should be sufficient. The quality of service care, the number of follow-ups for maternal and child health, and the number of community-level training on maternal and child health should be increased. The access of mothers and children to health services should be facilitated and the effectiveness of public health units should be increased.
Limitations and Future Studies
The study has several limitations. The generalisability of these results is subject to certain limitations. It is assumed that the variables used in the study represent the health systems performance of OECD member countries. It should not be forgotten that factors other than the determined health indicators can also affect the performance of health systems. When evaluating the results of the study, it should be taken into account that the results of the study may be affected by the fact that countries have different health systems, their economic levels, demographic characteristics and variances in socio-cultural structures. The findings of this study have a number of important implications for future practice. Future studies can expand the scope of the study by using different variables, examining the strategies and policies implemented by the countries.
Footnotes
Acknowledgement
This study is produced from Ferit Sevim’s master’s thesis titled ‘An Evaluation of OECD Countries Health System Performance’.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.