
Abstract
Payment methods based on a controlled or adjusted prospective payment system rather than ‘Fee for Services’ or direct payment are considered beneficial to access the healthcare delivery services. The purpose of this review was to identify technical challenges faced by three WHO regions, namely, Western Pacific, South East Asia Eastern and the Mediterranean while establishing or adopting a diagnosis-related group (DRG)/case-mix grouper and report the extent of implementing this system for reimbursement and healthcare financing in three WHO regions, namely, Western Pacific, South East Asia Eastern and the Mediterranean. The study followed PRISMA guidelines, and 33 articles published from 1st January 2009 to 31st December 2019 were selected for critical appraisal after systematic filtration. The objectives of the implementation of the DRG system in most developed and developing countries in these regions were to bring transparency in the payment system and reduce treatment costs by avoiding unnecessary healthcare services. The countries in the study regions were at different levels of economic and social development status, therefore the implementation and adaptation status of DRG/case-mix system/grouper varied in these countries
The findings revealed that most of the countries faced challenges related to inequalities and inefficiencies in the healthcare system, shortage of funding, poor documentation related to diagnosis and procedures, incomplete medical record files and lack of primary data required for the case-mix system during the DRG/case-mix adaptation phase.
The results also pointed to the importance of initial pilot testing of the DRG/case-mix system/grouper and careful manipulation and adaptation to the local context, especially when the DRG system/grouper imported from other countries.
Keywords
Introduction
Members of the World Health Organization (WHO) expressed their commitment to introduce Universal Health Coverage (UHC) in their countries during the 2005 World Health Assembly (Wei & Feng, 2019). The assembly agreed on developing a health financing system based on prepayment rather than direct payment, which was considered one of the barriers in healthcare delivery access (Myint et al., 2019). It was also considered a goal of WHO sustainable development for 2030 to reduce the rapidly growing hospital costs that are putting pressure on the governments and healthcare budgets (Myint et al., 2019). Further, higher healthcare costs due to increased demand for the healthcare services and increased implementation social protection policies, almost all developed and developing countries are attempting to review hospital services’ payment mechanisms. They are trying to do this to attain better quality and efficiency in the healthcare sector.
In the healthcare sector, hospitals and affiliated clinics are the points of contact for providing healthcare services. These services are mostly funded by the government, social or private health insurance, or out-of-pocket payments. In the past, the healthcare budgets were allocated mostly based on hospital inputs, including salaries, medical supplies and line items. Due to the rapid development in the healthcare sector, many countries started to follow ‘global budgets’ that have more flexibility and independence on budget spending. Additionally, many countries have set their policies for an alternative funding approach based on patient groups and activities (Mathauer & Wittenbecher, 2012). This approach is commonly described as diagnosis-related groups (DRGs)/case-mix base funding (also known as service-based funding, prospective payment and activity-based funding).
DRGs/case-mix can be described as the patient types treated and classified by diagnoses. DRGs are based on the patient’s principal and secondary diagnosis, surgical procedures performed, age, gender and discharge status. Case-mix is a patient classification system that was initially developed to connect a hospital case-mix to costs and was developed at Yale University in the 1970s (Fetter et al., 1980; France, 2003; Wei & Feng, 2019). Initially, DRGs were instigated for payment purposes in the United States during the 1980s. Nationally this system was implemented in the United States by the federal government in 1983. In the next 15 years, it was adopted by other countries in Europe and Australia followed by Asia (Goldfield, 2010). It has also been used in various countries of Europe and Australia for global budget allocation (Ng & Li, 2016). Generally, the DRG-based costing, and payment systems are based on a fixed amount related to patient classification based on the diagnosis/disease. A patient/case is always characterised by the consumption of resources in the DRG system (Cylus & Irwin, 2010). Thus, by using DRGs, hospitals can easily estimate the cost incurred, understand the patients being treated, and predict the expected services required in the future (Centers for Medicare & Medicaid Services (CMS), HHS, 2018).
Case-mix has become a universal measurement tool to analyse differences in clinical practices (France, 2001). Many high- and middle-income countries have also evaluated the case-mix payment system’s impact on the quality of care (Waitzberg et al., 2019). It is a continuously evolving process that is reviewed and updated as the clinical coding schemes are updated and reviewed (Centers for Medicare & Medicaid Services (CMS), HHS, 2018). To date, more than 40 countries worldwide have set their initiatives for a case-mix system for several purposes at various levels with different aspects, institutional setups and methodologies (Moon, 2015; Turner-Stokes et al., 2012). Several countries are still trying to implement DRGs based payment systems in government-owned healthcare settings (Leister & Stausberg, 2005).
It has been acknowledged from the experience of more than 40 countries that the establishment of the DRG/case-mix system in public hospitals is necessary for an effective payment system and promoting the prospective payment process. Studies have been done on implementing the case-mix systems in different countries or continents during recent years. However, we could not find any systematic review conducted in the WHO-defined regions that give a clear picture of case-mix implementation and allows the comparison among different regions.
This systematic review will help establish a comprehensive perception of DRG/case-mix systems for healthcare financing in three WHO-defined regions. For this purpose, we developed a review question that how many countries in three WHO regions, namely, Western Pacific, South East Asia Eastern and the Mediterranean, are using the case-mix system for health financing and reimbursement purpose?
Based on the above question, we established systematic review objectives. The first objective was to identify technical challenges faced by three WHO regions, namely, Western Pacific, South East Asia Eastern and the Mediterranean while establishing their DRG/case-mix grouper or adopting previously standardised DRG/case-mix grouper. The other objective was to report the implementation of the DRG/case-mix system at a pilot or national scale for reimbursement and healthcare financing in the above-mentioned three WHO regions.
To meet the above objectives, we need to review the literature that addressed the technical challenges during case-mix grouper selection and pilot testing of the case-mix system. We also need to review the literature that reported the case-mix system adaptation, strategies for case-mix system implementation for reimbursement and healthcare financing.
Review Methodology
This systematic review focused on the literature related to healthcare financing systems, reimbursement and health data classification systems. The study followed PRISMA guidelines. We compiled the PRISMA checklist for guidelines confirmation (Moher et al., 2015).
Study Period
The systematic review was conducted on data published from the 1st January 2009 up to the 31st December 2019. We selected the specific time horizon for the literature search based on the DRG implementation history. Though DRG was implemented in the USA in 1983, in Australia, it was adopted in 1992; it took decades to be adopted in other countries of the selected regions. Considering that it takes years to get DRG/case-mix operational, 2009 seemed justified to be the starting date. As per the protocol, all efforts were made to include the latest articles. We carried out the literature search on the 14th and 15th March 2020.
Systematic Review Strategy
Based on the above objectives and literature search needs, we developed a systematic review strategy. We followed the flow diagram as given in Figure 1 to develop the search strategy and meet the systematic review objectives.
Flow Diagram for Systematic Review.
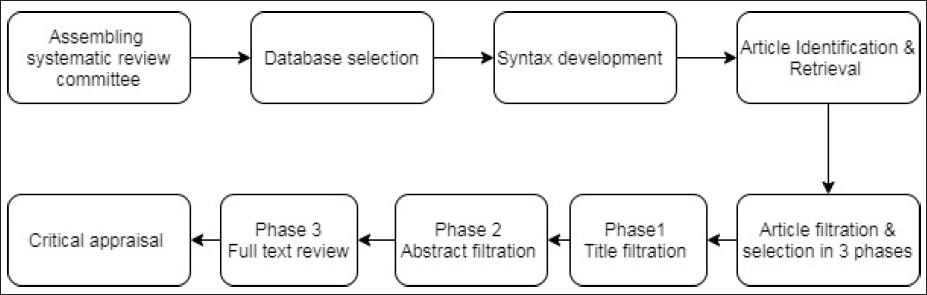
Systematic Review Committee
We assembled a team for systematic review consisting of six members, Asim Mehmood (AM), Zafar Ahmed (ZA), Khalid Ghailan (KG), Sushil Dohare (SD) and Joe Varghase (JV). We discussed the objectives of the study in detail and after reviewing many articles related to case-mix and its implementation in the world, we defined the key search terms.
Selection of Database
We decided to access the available databases through Saudi digital library as we had free access to this digital library subscribed by the Jazan University. We selected the ProQuest Repository through this digital library as the other repositories in the digital library had fewer databases related to Public Health, Health economics and Healthcare services administration than ProQuest. ProQuest had 59 databases, including ProQuest Central. The details of the databases are given as annex.
Syntax Development
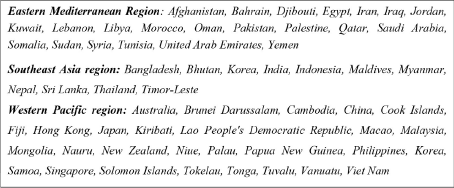
We refined the key terms during pilot testing to design the syntax for systematic review. We decided to apply Boolean logic terms ‘AND’ and ‘OR’ to search the key terms from everywhere (Title and Abstracts of the articles), other than the full text (noft). First, we designed the syntax for one region, and then it was adopted for other regions separately. The final syntax for the systematic review data retrieval was developed by using the key terms (‘casemix’ OR ‘case-mix’ OR DRG? OR ‘diagnosis related group’) AND noft (countries). The names of countries in each region are given in Box 1.
Names of Countries in Each Region.
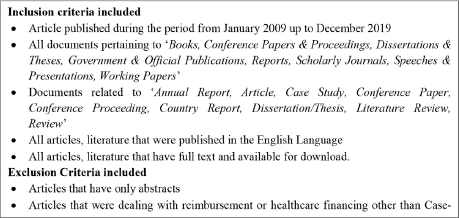
After the development of final syntax, we applied the inclusion /exclusion criteria for articles retrieval to meet systematic review’s objectives. Box 2 shows the inclusion and exclusion criteria applied to filter the articles.
Inclusion and Exclusion Criteria.
Articles Identification and Retrieval
After developing syntax and inclusion/exclusion criteria, we run the customised syntax separately for each region by using the already selected database. We identified and retrieved the articles for each WHO region separately, using the customised syntax for the specific region. We downloaded the master index for each region from the ProQuest repository directly into the Microsoft Excel format. The Excel output of the ProQuest repository given as Annex B contains information (Title, Abstract, Author information, Document number, Journal name publication date, and Subject terms for each article) about retrieved articles. Subsequently, shortlisted articles were also directly downloaded from the ProQuest database and coded.
Articles Selection and Filtration
The articles were shortlisted based on the inclusion and exclusion criteria given in Box 2. We filtered the articles in three phases.
In the 1st phase, two reviewers (AM, SD) reviewed the title of the articles from three Excel files, retrieved from the ProQuest database and identified whether they qualify to be included in the systematic review. In case of any conflict third reviewer (ZA) resolved the conflict for the selection or rejection of the articles to be included in the systematic review.
In the 2nd phase, the abstracts of the remaining articles were critically reviewed and articles that did not meet our objectives were excluded. In this phase, the remaining articles’ abstracts were independently reviewed by two reviewers (JV, SD), and excluded articles by agreement. Disagreements and conflicts were resolved by discussion and referred to a third reviewer (ZA) for confirmation.
In the 3rd phase, we merged the remaining articles retrieved from three WHO regions by using region-specific Syntax and removed the duplicate articles. Full-text copies of the remaining articles were downloaded and reviewed. The critical appraisal of these articles was carried out to assess their contribution for research and for evidence synthesis as per our research question, objectives and need for systematic review. Three independent reviewers (AM, JV, KG) reviewed the full text of these articles in the same way as the abstract screening. A fourth reviewer (ZA) resolved disagreements. The content of the final full-text articles selected for critically appraised is managed by the software Dedoose.
Results
In total, 537 articles were retrieved from the ProQuest repository by using the region-specific syntax. Out of these, 424 articles were identified from the Western Pacific region, 69 articles from South East Asia and 44 articles from the Eastern Mediterranean region.
We assessed the resulted articles separately for each region retrieved by using region-specific syntax. We followed the above given three-phase article selection and filtration strategy.
In the 1st phase, 368 articles from the Western Pacific region, 52 articles from South East Asia and 34 articles from Eastern Mediterranean region were found irrelevant and agreed by the review committee for exclusion.
In the 2nd phase, after critically reviewing the abstract of the remaining articles, 29 articles from Western Pacific region, 8 articles from South East Asia and 6 articles from the Eastern Mediterranean region were excluded.
In the 3rd phase, we merged the remaining articles retrieved from three regions and removed the duplicate articles. Seven duplicate articles were found in this phase and excluded from the study as shown in Figure 2.
Article Selection and the Filtration Process.
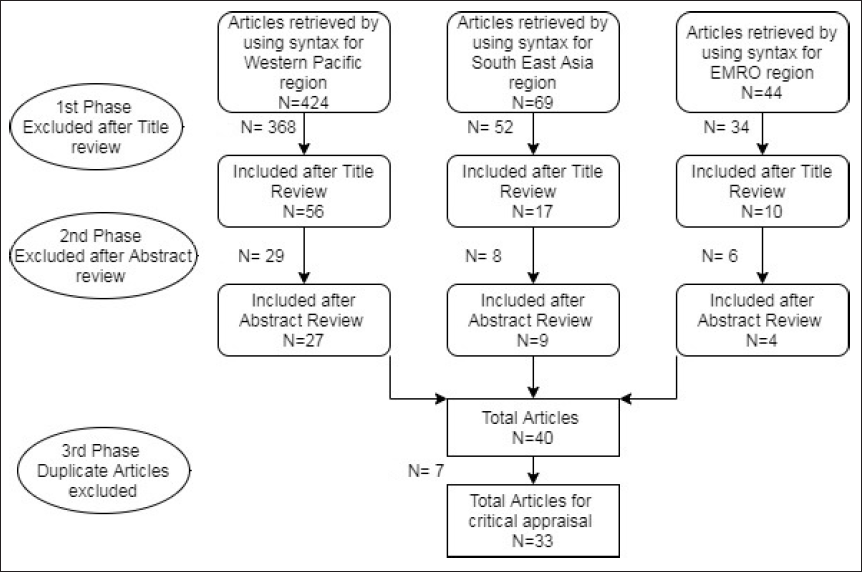
Finally, 33 articles were identified for a full-text review and were included in the study. Among these 33 articles that were selected for final review, six studies were conducted in China (Jian et al., 2015; Jiao, 2018; Tabrizi, 2012; Wei & Feng, 2019; Yu et al., 2016; Yuan et al., 2019), six in Malaysia (Aljunid et al., 2010, 2011a, 2011b; Kamaliah et al., 2009; Mohamad, 2012; Turner-Stokes et al., 2012), four in Indonesia (Gultom & APT, 2012; Kasra et al., 2012; Rahimi et al., 2012; Saputra et al., 2012), two in South Korea (Jeon et al., 2019; Moon, 2015), two in Japan (Nakagawa et al., 2011; Okochi, 2012), two in Australia (Aisbett, 2010; Reid et al., 2011), two in Thailand (Pannarunothai, 2012; Pongpirul et al., 2011; Rahimi et al., 2012) and each one in New Zealand (Ng & Li, 2016), Philippines (Gool, 2012), Egypt (Yahia et al., 2016), Lebanon (Ammar et al., 2013), Iran (Ghaffari et al., 2010) and Hong Kong (Lam et al., 2011). Three articles were systematic reviews representing the data on DRG/case-mix studies in China, Singapore and Vietnam (Myint et al., 2019; Tabrizi, 2012; Turner-Stokes et al., 2012).
Critical Appraisal of Selected Articles for Evidence Synthesis
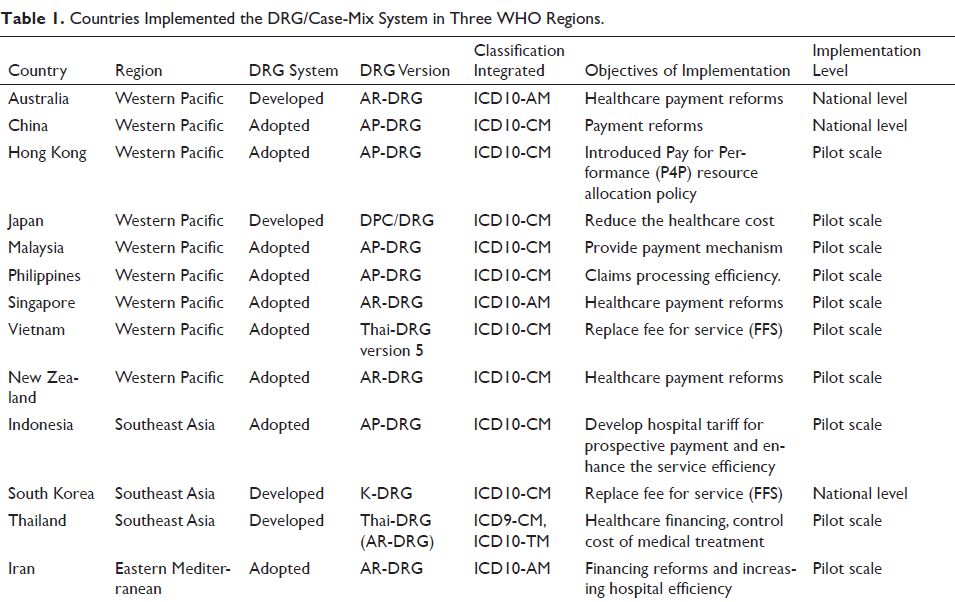
We carried out the critical appraisal of the 33 articles selected from the systematic review. The articles were retrieved and filtered systematically by using three WHO region specific syntax as explained above. There are 61 countries in these three WHO-defined regions that were included in this systematic review. Among these 61 countries, only 15 countries implemented a case-mix system for healthcare financing, reimbursement or tested it on a pilot scale. Out of these 15 countries that implemented the case-mix system, only four countries developed their own DRG grouper system while the other adopted the existing DRG grouper system as shown in Table 1. The other countries of these regions did not take any initiative in this regard or are at initial stages and data was not yet reported or published anywhere (Mathauer & Wittenbecher, 2012).
Countries Implemented the DRG/Case-Mix System in Three WHO Regions.
The following two sections explain the research evidence synthesised as per our two systematic review objectives. One deals with the technical challenges faced during case-mix system/grouper adaptation and the other deals with the implementation of case-mix system-based reimbursement systems in three WHO regions.
Technical Challenges in DRG/Case-Mix System/Grouper Adaptation
DRG has been adapted and improved over the decades in many countries. It remains an evolving process, and a variety of challenges have been identified (Pongpirul et al., 2011). Though the USA’s DRG system was the pioneer but various DRG systems are now available and currently in practice worldwide. Nowadays, DRG systems with unique design characteristics are available that are different from what was initially developed. Many countries developed or modified the existing system, for instance, country variants, DPC systems have been developed by Japan, ‘K-DRG’ developed by the Republic of Korea, ‘AR-DRG’ developed by Australia and ‘Thai-DRG’ by Thailand (Aisbett, 2010; Jeon et al., 2019; Moon, 2015; Nakagawa et al., 2011; Okochi, 2012; Pannarunothai, 2012; Pongpirul et al., 2011; Rahimi et al., 2012; Reid et al., 2011).
Generally, there are two options for countries planning to adopt DRG systems. They can either develop a new DRG system or adopt one of the existing DRG systems and refine it. The first option requires a well-developed health administration and health information system, while the latter is often expensive and bring issues related to intellectual property rights (Wisaijohn et al., 2010).
There are technical challenges that countries should consider before considering any option like; is the country’s situation favourable to implement this system, and what will be the fundamental purpose of using this DRG system (Mathauer & Wittenbecher, 2013)? Healthcare systems also face many challenges, including limited resources, high costs of medical and medical technologies, high consumer demands, and the lack of tools to support planning and management, particularly with the growing complexity of healthcare systems (Yahia et al., 2016).
By adopting any existing DRG system and refining it according to local needs, it is necessary to launch a pilot testing before importing such a system. For pilot testing, some preliminary check points are essential to consider. These may include the generation and implementation of the standard classification system for morbidity and mortality data, development of hospital costing system, awareness of the importance of case-mix systems among clinicians, and the government’s willingness to make regulatory changes to adapt this system (Rahimi et al., 2012; Wisaijohn et al., 2010). The case-mix system implementation also requires a structured and computerised system with well-trained and well-oriented personnel; otherwise, the system would fail. Improved knowledge and understanding of the financial system among managers and staff in hospitals and healthcare systems can help improve services related to the case-mix system (Rahimi et al., 2012). International donors have urged several developing countries to increase current social insurance programs’ performance by adopting the prospective form of payment. Unfortunately, the unavailability of an open-source, low-cost and customisable case-mix grouper is a significant barrier to the introduction of the case-mix framework in most developing countries in these regions (Aisbett, 2010; Aljunid et al., 2011a). Most low- and middle-income countries in these regions are experiencing a population and healthcare transformation, with a growing disease burden, a substantial rise in chronic and non-communicable disease prevalence, and an apparent gap in health services distribution (Ammar et al., 2013; Ghaffari et al., 2010; Gool, 2012; Yahia et al., 2016).
Case-based or prospective payment systems are not exclusively technological mechanisms but are also influenced by social and political aspects which are country specific. Like in China the obstacles created by medical associations China were also a significant challenge that was not prepared to develop, implement, assess, review and improve the DRG system (Jiao, 2018; World Health Organization, 2015). In China, 20 out of 32 provinces introduced certain types of DRGs by 2016 (France, 2001; Turner-Stokes et al., 2012; Wang et al., 2014). However, the system has various other challenges related to data quality in electronic medical records, hospital management issues related to medical ethics, clinical notification and patient confidence (Wang et al., 2014). In South Korea, the significant challenges while adapting this system were directly related to healthcare providers’ where primary concern was the underlying risk of decreasing the quality of the health services to save premium costs and benefits. Additionally, contradictory findings related to increased post-surgical ambulatory visits and overall health expenditure were also observed before and after the DRG payment system’s pilot project (Jeon et al., 2019; Moon, 2015).
From China and South Korea experience, developing countries must adopt simple and basic prospective payment systems to avoid complex challenges during the case-mix system’ initial implementation phase (Wang et al., 2014).
Almost all countries that were included in the study faced similar challenges during the case-mix system adaptation phase. These were related to inefficiency of the healthcare system, shortage of funding, poor documentation related to diagnosis and procedures, and lack of primary data required for the case-mix system (Ammar et al., 2013; Ghaffari et al., 2010; Kasra et al., 2012; Pongpirul et al., 2011; World Health Organization, 2015). Inconsistencies between the diagnosis and procedure codes submitted and those recorded in the medical records had also led to many disputes about medical record reliability and considered as a big challenge for case-based payment system implementation (Pongpirul et al., 2011). Data unavailability at one place under the unified system was also reported in various countries like in Vietnam and Thailand, where the data was scattered into different places and control systems. It made difficult to align with the costing systems because, for implementing the case-mix system, patient-level cost data is one of the significant challenges that cannot be ignored (Mathauer & Wittenbecher, 2013; Pongpirul et al., 2011). Different studies also explored the importance of coding systems, extended length of stay (LOS) and relative cost weights for the case-mix system that can influence the case-mix system integrity and considered as a big challenge (Jadoo et al., 2015; Nakagawa et al., 2011; Turner-Stokes et al., 2012; Wang et al., 2014). To avoid the challenges during and after the implementation, prior planning and consideration of possible stakeholder feedback through society’s involvement are essential (World Health Organization, 2015).
DRG/Case-Mix Implementation for Reimbursement and Healthcare Financing
The objectives of the DRG system implementation in most developed and developing countries were to bring transparency in the payment system and reduce treatment costs by avoiding unnecessary LOS and care. Standardisation of medical coding, improvement of health information technology and enhancement of system capacities are identified as critical steps that are required during the implementation phase (Busse et al., 2011). In addition to this, the coding practice must reflect the patient actual clinical condition to produce reliable and consistent quality data. It was also found that a well-organised computerised system with well-experienced staff is essential for implementing the case-mix system that can help to change the payment system from retrospective to a prospective costing system based on the DRG. Overlooking these factors can fail the system (Aisbett et al., 2007; Ng & Li, 2016; Wang et al., 2014).
Within the three regions included in this systematic review, countries are placed at different economic and social development levels. Higher-income countries like China, Japan, Australia, New Zealand and the Republic of Korea have DRG systems. Among the middle-income countries, Malaysia, Thailand have introduced case-based payments more recently and still exploring new opportunities through pilot testing, while Iran and the Philippines have been developing a system over the last two decades. Lower-income countries like Vietnam are on initial stages for the experiments with different forms of case-based payments for hospital services (Mathauer & Wittenbecher, 2013).
Hospital payment systems based on DRG/case-mix and other case-based payment systems have been established in Australia, Japan, China, New Zealand and the Republic of Korea. DRG system has also been implemented partly in Indonesia, Malaysia, the Philippines, Singapore and Thailand and is under consideration in Iran, Vietnam and Hong Kong.
It is interesting to note that the countries that have already implemented DRG-based hospital payment systems, such as Australia, Japan, New Zealand and the Republic of Korea, have health systems that also provide UHC in some form.
In the Western Pacific region, Australia and Japan have developed their DRG systems, while Malaysia is also trying to develop its system. New Zealand, China, Hong Kong, the Philippines and Singapore have also adopted the existing system for pilot testing and implementation. Australia has a long history of case-mix development since the 1980s to track financial activity and intra-hospital resource allocation. After initial implementation in 1992, this Australian version was periodically updated based on Australian first and second editions of ICD-9 in 1995 (ANDRG versions 3.0) and 1996 (ANDRG versions 3.1). This DRG classification was refined various times and finally, in 2015, version 8.0 of the Australian DRG was released and implemented countrywide (Jackson et al., 2015). New Zealand and Singapore also adopted the Australian version of DRG for classification to resolve payment mechanisms and reimbursement issues. New Zealand followed the AN-DRG version 2.1 initially in 2001 and then periodically updated the system as and when the disease classification system was updated (Ng & Li, 2016). Singapore adopted this system in 1998, and within one year, it was modified for the local needs and extended to all its public hospitals in 1999 (World Health Organization, 2015). In 2003, Japan modified the hospital payment system based on Diagnosis Procedure Combinations (DPC), which was a ‘per day’ treatment system rather than a ‘per case’ payment system (DRG). Due to the high average LOS at hospitals in Japan, this system was expected to reduce the average LOS and health costs (Nakagawa et al., 2011). Additionally, the case-mix system was also tested using the WHO recognised International Classification of Functioning (ICF) in 2001. The ICF offers an extensive overview of hierarchical categories functioning that can be used globally as healthcare professionals’ standard categorisation (Okochi, 2012).
China introduced the concept of DRG in Beijing Province in 2001. The initial systems were refined and updated over time until 2009, when it was ready for countrywide implementation. Until 2016 20 provinces of China have implemented this system in their healthcare systems. They introduced this system to improve hospital efficiency and control the medical cost and standardise healthcare providers’ behaviour (France, 2001; Turner-Stokes et al., 2012; Wang et al., 2014). This implementation has changed the trend of a continuous increase in cost for different healthcare services and set a benchmark for hospitals for price-setting mechanism (Wei & Feng, 2019; Yuan et al., 2019). Hong Kong introduced this system in 2008 under pay for performance policy to streamline the resource allocation for the Hospitals (Lam et al., 2011).
In Malaysia, the case-mix/DRG implementation study started in 1996 and in 2002 the University of Kebangsaan was the first hospital to introduce the full case-mix system (Aljunid et al., 2010; Mohamad, 2012). United Nations University-Case Base Group (UNU-CBG) grouper based on ICD-10-CM was also developed to group the diseases. They developed this case-mix grouper for use in developing countries. It was launched initially in 2009 and is currently being used in four countries (Indonesia, the Philippines, Uruguay and Malaysia) (Aljunid et al., 2011). Additionally, University Kebangsaan Malaysia Medical centre also developed a case-mix for pharmacy services based on Malaysian DRG (MY-DRG) to identify pharmacy services’ actual cost (Jadoo et al., 2015). After its implementation, various case studies were also done to check the effectiveness of the case-mix system (Aljunid et al., 2010, 2011; Kamaliah et al., 2009).
Philippines, Vietnam, South Korea and Thailand have planned to replace the ‘Fee for Services’ system with case base or prospective payment systems (Gool, 2012; Institute of Medicine, 1995; Jeon et al., 2019; Moon, 2015; Pannarunothai, 2012; Wisaijohn et al., 2010; World Health Organization, 2015). In the Philippines since 2011 government introduced the DRG/case-mix to change the provider payment mechanism from ‘fee for service’ to ‘case rates’. This system is still under pilot testing and predicted to bring revolutionary changes in the Philippines’ healthcare system (Gool, 2012). Vietnam also planned to adopt the Thai-DRG-based case-mix system and will refine it to develop its case-mix (Viet-DRG) grouper system soon (World Health Organization, 2015). South Korea and Thailand are the most advanced in DRG implementation. Since 1997, South Korea was working on the concept of a case-mix system. It was initially adopted from the United States and subsequently modified to develop a new system based on local needs. In 2013, South Korea successfully developed and implemented a countrywide, Korean-based DRG (K-DRG) system for reimbursement (Jeon et al., 2019; Moon, 2015). Thailand introduced the DRG system in 1993, intending to reform the healthcare financing mechanisms and, ultimately, to control the cost of medical treatment. To meet these objectives, they introduced many revolutionary changes and developed their DRG system (Thai-DRG) based on ICD-9 CM (Clinical Modification), which was later shifted to ICD-10 TM (Thai Modification) in 2007 (Institute of Medicine, 1995; Pannarunothai, 2012; Wisaijohn et al., 2010).
Indonesia and Iran have set their policies to implement case-mix systems in public hospitals, but they are on initial stages. Indonesia introduced a pilot project in 2005 for a prospective payment system to enhance services’ efficiency in the health sector while Iran launched a case-mix pilot project based on the Australian Version of DRG as a part of financial reform initiative (Ghaffari et al., 2010; Kasra et al., 2012; Rahimi et al., 2012). Indonesia also adopted a newly developed (UNU-CBG) DRG system for this purpose and then modified for local use (Gultom & APT, 2012; Kasra et al., 2012; Rahimi et al., 2012; Saputra et al., 2012).
Saudi Arabia, the United Arab Emirates and the Philippines are in the initial data standardisation stage. Saudi Arabia and the United Arab Emirates have agreed to implement an Australian-based D.R.G. system in 2005, but no pilot study was done on its implementation since then. While studies in Lebanon indicated the development of the case-mix index in hospitals under the Ministry of Public Health (MoPH) for research purposes, there is currently no evidence for implementing the DRG/case-mix system (Ammar et al., 2013).
The other countries of the three WHO regions have not yet set their policies and initiatives to implement this system for reimbursement or improve hospital efficiencies. They have not implemented a case-mix system yet but have computerised data on hospital inpatient activities using ICD-10, supplemented by country-specific coding systems for procedures (Ammar et al., 2013; Turner-Stokes et al., 2012; Wang et al., 2014).
Conclusion
DRG is a valuable tool to save medical costs and increase hospital quality and efficiency. This system is technically and administratively complex, and its practical operation depends on organisational behaviour and can improve the productivity of the healthcare system.
DRG/case-mix and its associated cost weights are also directly related to developing new funding methodologies for the hospitals. It creates coordination between clinical and administrative staff to improve healthcare services’ quality and efficiency while managing the expenditures.
For successful implementation of the DRG/case-mix system, continuous evidence-based assessment and monitoring of healthcare services and adequate management system are necessary parts of this process.
Our literature findings indicate that initial pilot testing of the case-mix system across selected hospitals is safer option for developing countries. If an existing DRG version is imported, care should be taken to adapt it to the local context. Furthermore, adopting a DRG-based system is a part of a long-term process of continuous growth and provider payment system adaptation. It could require merging multiple provider payment structures to achieve the optimum balance of benefits, as has been done in many advanced health funding schemes.
Footnotes
Limitations
There were some limitations in this systematic review. First, we only focused on one database. Second, only three WHO regions were covered in this systematic review. We only considered articles that were published and available online. There is a need to further explore the potential effects of various aspects related to the DRG-based system in the countries included in the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.