
Abstract
Reporting of incidents and near misses among healthcare professionals can help target improvement efforts and system changes to reduce the likelihood of patient injury. This study explored barriers that hinder healthcare professionals’ disclosure of incidents and near misses in hospital settings in Saudi Arabia. Cross-sectional data were collected using a qualitative semi-structured interview with 30 participants, including surgeons, physicians, nurses, allied health professionals, pharmacists, and healthcare quality staff during January and February 2020. Barriers reported by the participants were classified across six themes: fear, lack of knowledge, lack of leadership support, workload, reporting system, and lack of motivation. Health leaders must ensure that the reporting process is planned, designed, and implemented in a nonpunitive manner. When selecting middle-level managers, their knowledge regarding quality of care and patient safety practices should be assessed. The findings of this study add to existing knowledge regarding the barriers preventing the reporting of incidents and near misses among healthcare professionals.
Background
The reporting of incidents and near misses is critical for enhancing patient safety and quality of care. Many accreditation programs, such as those developed by The Joint Commission (2019) in the United States, Accreditation Canada (2020) and the Australian Council on Healthcare Standards International (2020), emphasise the importance of reporting by encouraging healthcare professionals to report any issue that could potentially harm patients or staff.
The World Health Organization (2005) defines an incident as ‘any deviation from usual medical care that causes an injury to the patient or poses a risk of harm. It includes errors, preventable adverse events and hazards’, while it defines a near miss as ‘an error that has the potential to cause an adverse event (patient harm) but fails to do so because of chance or because it is intercepted’.
The relationship between incident reporting and improvements in quality and safety is complex and increasing reporting alone may not be enough to accomplish these improvements (Macrae, 2016). However, incident reporting allows for data collection and aggregation to determine patterns that may lead to corrective action (Hor et al., 2010). Further, examining incidents to learn about their root causes and contributing factors can help prevent future occurrences of similar incidents (Jahromi et al., 2014). However, barriers related to healthcare professionals’ concerns about repercussions reduce the effectiveness of reporting (Cochrane et al., 2009). Several studies have found that healthcare professionals fear administrative sanctions, blame, repercussions and punishment, rejection by bureaucracy and managerial scrutiny (Bodur & Filiz, 2010; Heard et al., 2012; Hwang et al., 2012; Malik et al., 2010; Polisena et al., 2015). Administrative measures include fear of economic sanctions and of losing one’s position (Engeda, 2016). An Australian survey by Evans et al. (2006) found that increased workload ranked near the top of healthcare professionals’ reasons for not reporting incidents and near misses. More recently, Uwimana (2017) noted that the incident report form is exhaustive and takes considerable time to complete. Different countries have different reporting requirements and mechanisms and, consequently, potentially varying sets of barriers. Little research in this area has been conducted in Saudi Arabia. Therefore, this study aimed to explore the barriers that hinder healthcare professionals’ disclosure of incidents and near misses in hospital settings in Saudi Arabia. The study’s outcome could inform the development of effective recommendations for enhancing reporting, which could improve quality of care and patient safety.
Methods
Design and Participants
A qualitative semi-structured interview was utilised to explore the barriers that influence the reporting of incidents and near misses. The study was conducted in a Saudi government hospital with a capacity of 250–300 beds. Healthcare professionals with at least one year of experience were included in the study. Thirty participants from different healthcare fields were purposively selected for the interviews to ensure that there was a variety of professionals, such as surgeons, physicians, nurses, pharmacists, physiotherapists, radiographers and healthcare quality professionals. The final number of participants was determined by data saturation. Data collection occurred over a 2-month period (January to February 2020).
Data Collection
The interview gathered information about participants’ reporting of incidents and near misses. An open-ended question related to the study’s aim was used to gather data about the barriers that prevented healthcare professionals from reporting incidents and near misses. Each participant was provided with an information sheet. All participants were informed that the interview was being voice-recorded and that they had the right to withdraw at any time. Participants’ information was anonymised using pseudonyms and codes. Ethical approval was obtained from the institutional review board of a university in Saudi Arabia (H-2019-091).
Data Analysis
Braun and Clarke’s (2006) step-by-step framework for performing thematic analysis was followed, which involves six steps: familiarising oneself with the data, generating initial codes, searching for themes, reviewing the themes, defining and naming the themes and producing a report. The MAXQDA 12 software (Verbi Software, Berlin, Germany) was used for the text coding and storage.
Results
Characteristics of Participants
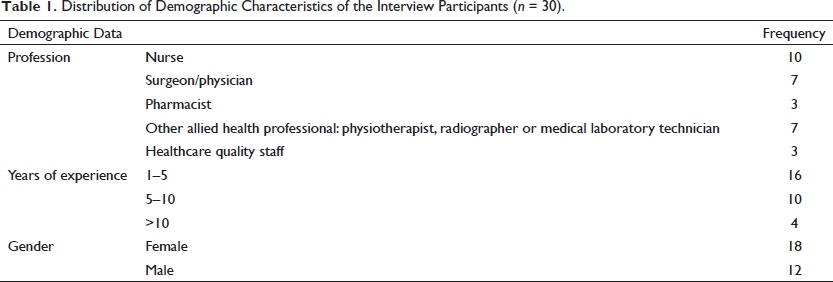
One-third of participants were nurses (n = 10) and 23.3 per cent (n = 7) were physicians and surgeons, while the remaining participants were from different professions, such as pharmacists, other allied health professions and healthcare quality staff (Table 1). Slightly more than one-half (n = 16) of participants had between 1 and 5 years of professional experience, one-third (n = 10) had between 5 and 10 years of experience and 13.3 per cent (n = 4) had more than 10 years of professional experience. Females comprised 60 per cent of the sample.
Distribution of Demographic Characteristics of the Interview Participants (n = 30).
Barriers That Hinder the Reporting of Incidents and Near Misses
Healthcare professionals mentioned several barriers that hindered their reporting of incidents and near misses. Six themes representing these barriers emerged from the interviews: fear, lack of knowledge, lack of leadership support, workload, the reporting system and lack of motivation.
Theme 1: Fear
For most participants, fear was a critical barrier to reporting incidents and near misses. They argued that reporting incidents or near misses could lead to disciplinary actions. Such actions could manifest as mistreatment, non-appreciation of their efforts, and inequitable workload distribution, which made the employee reconsider becoming involved in the report. Participants believed that reporting could negatively affect their employment stability and career advancement. One participant summarised this as follows:
The personnel with higher authority may misuse their authority to stop the employees from reporting the problem because they are worried that it might make their departments look bad or are worried about getting themselves into trouble. (Participant 2, Physician) It is difficult to report incidents. Most managers do not appreciate the reporting. They will take it as a criticism. They will say ‘Why did you report? We do not have problems and complaints in our department.’ After making a report, they will scrutinize your actions. They will go behind your back. They will try to find any small mistake to punish you. They will make you hate your job. (Participant 9, Nurse)
Fear also extended to other factors beyond punishment and professional opportunities. Some employees preferred not to reveal patient safety-related incidents because they believed that it might harm their colleagues. Social ties with their colleagues led to the belief that reporting incidents is a betrayal. As a result, many employees preferred to discuss the issue with their colleagues in an informal setting, rather than following the formal process. Many adopted this attitude to maintain good relationships with their colleagues. They considered that they were doing their colleagues a favour by discussing the issue with them in a friendly way, and pointing out the source of the error without reporting it. Moreover, participants believed that their colleagues might return this favour if the participant were to make a similar mistake in the future.
I am afraid of losing my empathy toward my co-workers. If I report an incident, my colleagues will be upset. This will then make my job more difficult. My colleagues will consider me a troublemaker. So, I usually avoid reporting incidents, as I can talk about it with my colleagues in a friendly way. I do this as a favor to them (Participant 7, Nurse)
Theme 2: Lack of Knowledge
Lack of knowledge was a barrier that limited reporting among hospital staff. Lack of knowledge included several aspects, such as whether near misses required reporting, how the reporting process worked and to whom participants were supposed to report. Some participants believed that some employees’ knowledge about particular incidents was insufficient to warrant reporting, especially when there was limited harm to patients. Ambiguity and uncertainty might have hindered the reporting of incidents and near misses, as the involved healthcare providers were usually uncertain regarding what should be reported and how to report it.
As some employees could not express the problem clearly, they avoided placing themselves into a reporting situation. Some employees may have been unaware of the risk-management programme, its significance, or how to use it. In some situations, employees may have even been willing to hide problems because they believed it the best way to improve the hospital or department’s image.
Some employees underestimate the whole situation. They think that if they prevent harm to the patient, that is enough and no problem needs to be reported. (Participant 8, Pharmacist) Some believe that when reporting incidents or sentinel events, they expose themselves or their colleague to legal accountability, and that if it is referred to the investigations department, this will then entail compensation for the patient or their family and possibly a deduction from the healthcare professional’s salary. (Participant 5, Healthcare Quality Staff)
Theme 3: Lack of Leadership Support
Most participants viewed lack of leadership support as a key factor in the reporting of incidents and near misses. The main aspect of leadership support that was highlighted was reducing fear and lack of knowledge about the nature and purpose of reporting and quality-improvement practices. Participants argued that employees must feel safe and that they should never be punished when trying to highlight problems in order to solve them.
We need support from top management. Everyone should know that we are one team working in the patients’ best interest, and that mistakes can happen. Therefore, we all have to cooperate to prevent incidents from happening in the future. Top management should ensure that there is no misuse of authority that prevents discussion of these problems. (Participant 6, Allied Health Professional)
Some participants explained the challenge of a lack of leadership support by stating that some managers lacked knowledge about healthcare quality-improvement tools and patient safety practices. Participants said that some leaders blamed individuals for reporting and overreacting, and considered reporting as a criticism of their performance.
Some leaders do not support reporting. In my hospital, some managers and department heads are not aware of quality-improvement tools and practices, such as reporting. Some managers are opposed to reporting. Moreover, some managers do not take any action when workers report incidents; instead, they try to find out who made the report to go behind their back. (Participant 2, Physician) Some managers discipline the reporters even if the Quality Department tries to protect the reporters because we lack leadership support even from the top level. (Participant 17, Healthcare Quality Staff)
Theme 4: Workload
Some participants argued that their workload influenced the reporting of incidents and near misses. Participants noted that some employees prioritised their daily routine tasks because they already worked under significant pressure, which is why they avoided taking on additional stressors, such as the reporting process. They stated that the reporting process involved time and effort, as they had to not only gather information and write the report but often also had to complete additional steps in the process. In some situations, reporters were tasked with following up with all departments and individuals involved in their reports.
Reporting can be a burden. When I report an incident, they will keep asking me about my report. I have a heavy workload as is. The Quality Department should have a sufficient team to follow up on the report. I think many employees are worried about the consequences of starting an argument about the ideal way to manage certain issues because they think that this will cost them extra time and effort in the future. (Participant 11, Allied Health Professional) I think that some departments should have full-time quality coordinators who can focus on reporting. As employees, we have a heavy workload and often forget or do not have sufficient time to report an incident. (Participant 4, Nurse)
Theme 5: Reporting System
Participants considered the reporting system and process important barriers to the reporting of incidents. They noted that detailed paperwork and extensive forms made reporting a difficult process and suggested that a user-friendly system could encourage them to report. They expressed difficulty with the length and detail of content, while noting that access to the reporting system was sometimes difficult. Some participants suggested that the reporting system should be electronic to make it much easier to manage statistics and updates.
The system is difficult. It is too detailed and complicated. The complicated paperwork and the long process confuse the staff and make them hesitant to submit a report. This is why many people avoid reporting. Instead, a user-friendly system should be implemented. (Participant 1, Nurse)
Theme 6: Lack of Feedback
Some participants believed that reporting was inconsequential and that nothing would change following a report. Participants’ previous frustrating experiences with quality practices discouraged them from reporting new problems. Some participants thought that no action was taken with their reports and that there was no benefit to reporting again. Therefore, some participants proposed the implementation of a system to motivate individuals to report. They suggested using a fair system that acknowledged individuals who reported incidents and near misses. Positive feedback regarding reports could motivate future reporting.
From my experience, people will not continue to provide suggestions when they receive no feedback from the hospital. Not recognizing the reporters of problematic incidents or near misses who identify unsafe conditions or who have good suggestions for safety improvements could discourage them from reporting again. (Participant 2, Physician) Every time I report, I spend time and effort addressing certain problems, which sometimes affects the relationship with my colleagues, as it gets them into a confrontation with the authorities, which could get them into trouble. Besides, after making the report, nothing changes and no action is taken to prevent such problems in the future. This can be very frustrating and discourages me from reporting problems, as the cost of reporting far outweighs the benefits. (Participant 12, Nurse)
Discussion
This study identified that fear, lack of knowledge, lack of leadership support, workload, the reporting system and lack of motivation were the most significant barriers to healthcare workers’ reporting of adverse incidents and near misses. Fear and worry were emotions that discouraged participants from reporting, as they reported that, in their experience, reporting usually implied penalisation. Many healthcare professionals expressed varying degrees of fear of administrative sanctions if they report incidents. Consistent with other international studies (Zwart et al., 2011), the current study also showed that healthcare professionals feared that disciplinary measures could greatly affect their career. Consequently, healthcare professionals worried that reporting could affect future evaluations, as well as negatively affect their relationships.
In this study, most healthcare professionals lacked the knowledge and skills required for effective incident reporting. This is consistent with Engeda (2016), who found that reporting practices were based on staff’s consideration of the importance of the incident to the patient.
This study revealed that lack of organisational support was an important barrier to the reporting of incidents and near misses. Another study suggested that an independent organisation not subject to the influence of supervisors/leaders or department heads should evaluate incident reports in hospitals (Reason, 2013). A non-accommodating environment, which emphasises professional autonomy, collegiality and self-regulation, is unlikely to foster incident reporting (Malik et al., 2010). Consistent with earlier literature (Ajri-Khameslou et al., 2018; Lynch et al., 2017; Vrbnjak et al., 2016), the current study also showed that the considerable time and effort required in the reporting process influenced healthcare professionals’ willingness to report. In a Swedish study, healthcare professionals indicated that incident reports implied extensive paperwork (Carlfjord et al., 2018). Developing systems to reduce the time required to report incidents might result in a considerable increase in the number of reports.
The findings of this study also revealed that one barrier to reporting was how the reporting systems were planned. Rashed and Hamdan (2019) found that healthcare professionals deemed the reporting structures and processes to be the greatest obstacles to reporting. Likewise, Rishoej et al. (2018) showed that inadequate integration between newly computerised reporting systems and conventional reporting systems seemed to prevent efficient incident reporting. These findings indicate the need for standardised guidelines to ease the transition into computerised incident reporting systems. The assurance of anonymity and confidentiality in reports is also important. A recent study found that an anonymous electronic reporting system would likely increase incident reporting among hospital staff (Archer et al., 2017). Therefore, it is recommended to have several reporting channels for more accurate incident reporting, such as paper-based reporting, stand-alone or integrated computer-based reporting and email or telephone reporting.
Consistent with other studies, the present study’s findings showed that healthcare professionals lacked motivation when composing incident reports. For instance, an anonymous survey revealed that two-thirds of anaesthesiologists in Australia and New Zealand agreed or strongly agreed that feedback was an effective strategy for enhancing adverse incident reporting (Harrison et al., 2018). Uwimana (2017) found that 61.8 per cent of nurses agreed that a barrier to reporting incidents was that they never received any feedback about the action taken regarding the incident. In two regional Australian hospitals, enhanced feedback significantly improved nurses’ and doctors’ reporting rates across numerous departments (Gleason et al., 2018).
The findings of this study add to existing knowledge regarding the barriers preventing the reporting of incidents and near misses among healthcare professionals. Several measures were taken to enhance interpretative rigor and trustworthiness of the findings, such as stringent data analysis and interpretation procedures (Holloway & Galvin, 2016). However, the main limitation of this qualitative approach is that the results cannot be generalised. This limitation is common to qualitative approaches, as they often involve a relatively small sample size; moreover, some of the themes are potentially only relevant to this one hospital.
Conclusions
This study found that fear, lack of knowledge, lack of leadership support, workload, the reporting system and lack of motivation were the most significant barriers to healthcare professionals’ reporting of incidents and near misses. Since fear is a critical barrier to reporting, health leaders must ensure that the reporting process is planned, designed and implemented in a nonpunitive manner. When selecting middle-level managers, their knowledge level regarding quality and patient safety practices should be taken into account. Additionally, providing education and training opportunities for staff to improve their knowledge and skills regarding patient safety practices and incident reporting could enhance the reporting process. Moreover, launching a ‘user-friendly’ system that protects confidentiality could also increase reporting. The minimum requirements to generate a report should be reviewed and summarised, as many participants find reporting systems to be a burden. Providing good feedback regarding reports could encourage those reporting to do so again, as needed. Reducing the barriers to reporting could improve reporting systems, consequently improving patient safety. Future research could further explore the barriers preventing the reporting of incidents and near misses using a quantitative approach that considers the themes explored in this study.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics and Other Permissions
The study was conducted ethically in accordance with the World Medical Association Declaration of Helsinki and was approved by the Ethics Committee, University of Ha’il, Saudi Arabia (Ethics number H-2019-091, Date: 3 December 2019). Written informed consent was obtained from all participants to participate in the study.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.