
Abstract
The study aims to understand the traditional healthcare management of the newborns of the Parengi Porja tribe. The Parengi Porja tribe is a Particularly Vulnerable Tribal Group (PVTG) that inhabits the Eastern Ghats, which is a continuous high hilly region of Visakhapatnam district, Andhra Pradesh, India. The members of this tribe strongly believe that the earliest weeks of a newborn’s life is the time for the greatest probability of death and disability. To avoid these misfortunes, they strictly follow the traditional healthcare regimen for newborns, which has significant socio-cultural importance. For this study, 105 neonates were purposively selected, and their mothers were interviewed for data collection. The research data were analysed by qualitative methods that included participant observation, in-depth interviews and focus group discussion. The collected data were repeatedly cross-checked with other elderly female members like grandmothers, and sutranimaizi (traditional birth attendant [TBA]) through interviews to strengthen the efficiency and authenticity of the data. The findings of the study show that this tribal population has its understanding of the management of neonatal health, which is socio-culturally ingrained, sanctioned and transmitted through generations.
Keywords
Introduction
Newborn survival is a prominent goal in the global health agenda and an important focus, seeking to ensure child survival (Carvajal-Aguirre et al., 2017). Globally, 2.4 million children died in the first month of life in 2019. There are approximately 7,000 newborn deaths every day, amounting to 47% of all child deaths under the age of 5 years, up from 40% in 1990 (World Health Organization, 2020). The mortality risk in the first 4 weeks of newborns’ life is 30 times higher than that in the post-neonatal period, that is, from 1 to 60 months of age (Sankar et al., 2016). WHO put forth a set of evidence-based neonatal health interventions named ‘Essential Newborn Care Practices’, including clean delivery, umbilical cord care, skin and eye care, initiating breastfeeding immediately or within the first hour after birth and thermal protection and immunisation, to combat the alarming rates of neonatal mortality and morbidity (Marsh et al., 2002).
Geographically, neonatal mortality is highly prevalent in southern Asia and sub-Saharan Africa, accounting for 39% and 38% of all neonatal deaths, respectively. The main causes of newborn deaths are premature birth (consequently low birth), intrapartum-related birth complications and infections, but the root cause is poverty—where people cannot access the quality healthcare they need in an emergency (UN Children’s Fund, 2018). India accounts for 640,000 global neonatal deaths. Even though the mortality rate has come down over recent years, the decline shows much slower due to different cultural practices embedded in every society. This ascertains that newborns’ health is not only determined by biological factors but also influenced by the socio-cultural environment of a community.
Among all the Indian states, Andhra Pradesh is leading in neonatal mortality with 34/1,000 live births and is home to the highest variety of tribal populations that contribute to half of the neonatal deaths (Indian Academy of Paediatrics, 2020). The tribal districts in the state bear the disproportionate brunt of neonatal mortality when compared with their non-tribal counterparts (Sample Registration System, 2013). The tribes live in geographical conditions ranging from plains and forests to hills. Their socio-cultural, economic and educational backgrounds differ from those of the Indian urban and rural communities. The most profound impacts of neonatal deaths are found in tribal societies. Issues such as geographical isolation, strong adherence to cultural beliefs and inaccessibility to modern medical services are also added to the poor neonatal outcomes.
More importantly, unless the cultural beliefs underpinning the traditional practices are documented, it might be difficult to achieve any change in healthcare practices. This is more applicable for a country like India with diverse socio-cultural structures because each tribal group has its practice system for care-seeking and caregiving, which necessitates a community-specific study (Pati, 2014). With this backdrop, this article attempts to understand the Parengi Porja notions on their traditional healthcare practices for the healthy survival and long life of newborns.
Materials and Methods
Study Setting
This study was conducted in Munchingiputtu Mandal located in the hilly forested regions of Visakhapatnam district, in the lining of Eastern Ghats, north-eastern part of Andhra Pradesh, India, from August 2014 to June 2018. Andhra Pradesh, given its adverse child health indicators, included Visakhapatnam district as one of the high-focus districts for child health improvement interventions. Visakhapatnam district has a population of 4,288,113, of which 14.5% are tribal population. It is home to seven particularly vulnerable tribal groups (PVTGs), of which Parengi Porja is dominant in Munchingiputtu Mandal. The study areas, namelyVanagumma, Talabirada, Pathaliputtu, Labbur and Jappar, were inaccessible to modern medical facilities and have poor motorable roads. The Parengi Porja is a PVTG that practises a pre-agricultural level of economy (subsistence cultivation and hunting and gathering group), has a low literacy rate (recorded 35%), is stagnant in population growth and leads a poverty-stricken socio-economic life.
Study Design, Study Participants and Inclusion Criteria
A community-based observational study was conducted among 105 neonates ≤60 days of age chosen with the purposive convenience sampling method in this study. The mothers of the neonates were considered the eligible participants for this study, and the grandmothers and traditional birth attendants (TBAs) were the study participants. The neonates were identified through the list obtained from the ICDS office in the Munchingiputtu Mandal. Each ICDS office is the congregation of multiple Anganwadi centres that work for the promotion and provision of nutritional diet for pregnant women, postpartum women, adolescent women and children below 5 years of age for their healthy survival in the poverty-stricken areas in India. This is a ruling issued by the government’s administrative unit intending to work for community well-being, specifically to promote safe motherhood, good child health and appropriate family-planning practices.
Data Collection Tools
Data collection was carried out using a qualitative approach (participant observation and interviews). Interview guides were prepared and pre-tested and comprised pre-decided themes on neonatal care practices to collect information from mothers, grandmothers and TBAs. The interview guide for mothers explored how they care for their newborns from the moment of birth. With this collected information, an attempt was made to assemble the beliefs and perceived rationale behind any specific behaviours. The interview guide for TBAs explored common delivery practices and precautionary steps to avoid dangers. Basic demographic information like age, education, marital status of the mothers were also collected. The researcher conducted the interviews in Telugu and Odia, which are local languages.
Data Analysis
The data were analysed with an approach outlined by Crang and Cook (2007) called the thematic framework that defines the data written on fieldnotes for observations and informal conversations, as well as the transcripts of the interviews, were analysed according to key themes such as place of delivery, umbilical cord care practices, awakening the baby and other healthcare practices. The written text was repeatedly read and manually coded, with the first step being ‘open coding’ in which the meaning of each statement or part of the text is scrutinised with an open mind for unexpected findings. For each code identified, a corresponding text was either marked or attached. The codes were listed and sorted; some were combined, others became sub-categories and still, others were excluded. The whole procedure was time-consuming, characterised by repeated reading, coding and ordering of the text. At the same time, insights, norms, gut feelings, beliefs and practices were registered in theoretical notes and later developed into explanations to find associations between them. The final stage was logical analysis, which is a kind of ‘iterative process’ through which the researcher rechecked eventual misfits and followed up on hunches (Bernard, 2006; Crang and Crook, 2007).
Results
NewbornCare Practices of Parengi Porja Tribe.
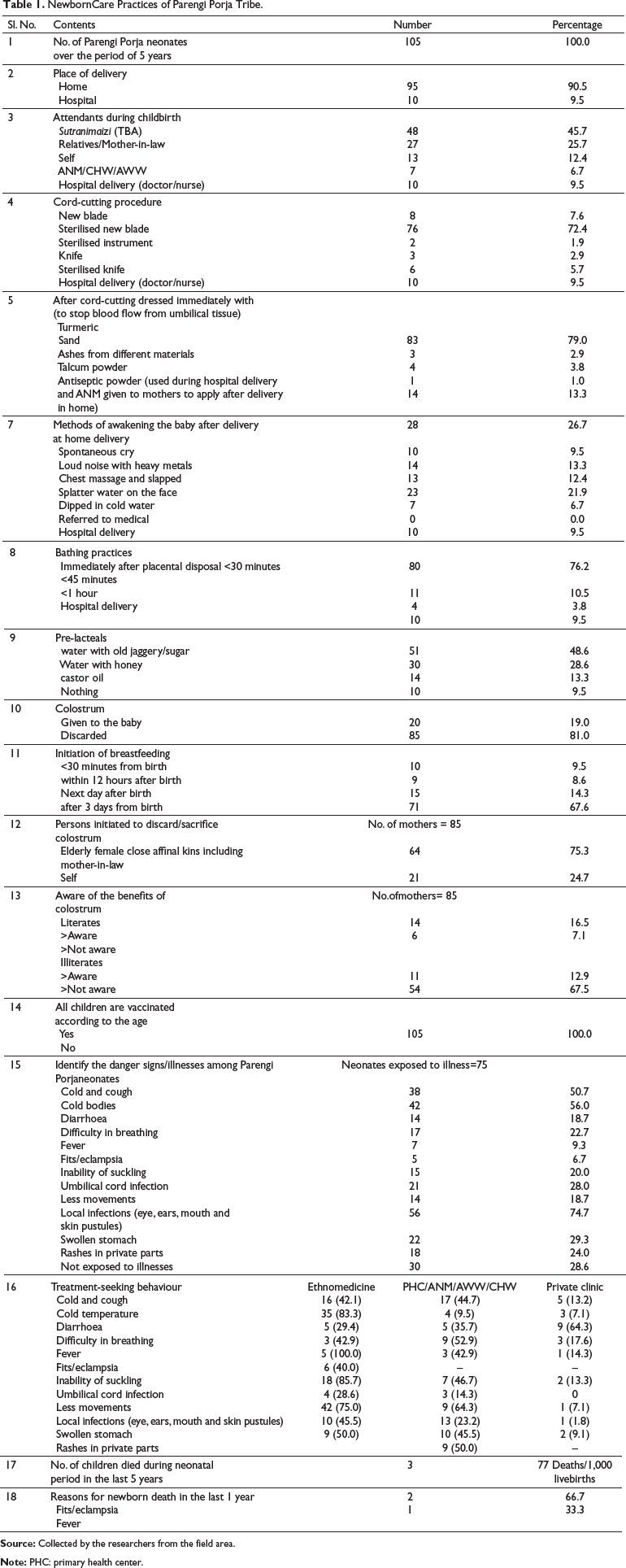
Utmost importance was given to do ‘safe cord care’, in which 72.4% neonates’ cord was cut using a sterilised new blade, followed by 7.6% with a new blade, 5.7% neonates’ cord was cut with a sterilised knife and 1.9% neonates’ cord was cut with sterilised instruments like arrow and sickle. In all neonates, the cord was tied with a clean thread smeared with turmeric paste after cutting. After that, they dressed the umbilical cord stump immediately with different substances like turmeric (79%), sand (2.9%), ashes of coconut shell/spider’s web/cloth/bamboo mat/pot powder (3.8%) and talcum powder (1.0%). Turmeric has natural antiseptic properties and is widely used in many Asian and African countries (Kesterton& Cleland, 2009). On the subsequent days, from childbirth, turmeric powder was generously applied on the cord stump for early drying and fall off without accumulation of pus or wound.
Only 26.7% neonates woke up spontaneously by crying in childbirth. The remaining neonates woke up to different ways of awakening methods, which indicates that the newborns had a breathing problem, which is recognised as an important sign to seek medical help (Pati, 2014). The babies were awakened by splashing water on the face (21.9%), making loud noise with heavy metals (13.3%), chest massage/slapping (12.4%) and through cold-water dip (6.7%).
Early bathing of neonates within 30 minutes (76.2%) of delivery with ragi powder to remove vernix and smearing them with turmeric paste at the end of the bath to keep away from infections and insect infestations is a common practice. Bathing the newborn in less than one hour appears to be a common practice within many cultures, as they consider that newborns are dirty since they came out of their mother’s womb (Yadav, 2007). Early bathing removes maternal bacteria and the vernix caseosa (a potent inhibitor of Escherichia coli; Tollin et al., 2005), which are not known to Parengi Porja, but the tribe still gives importance to remove vernix.
For home-delivered babies, 90.5% of neonates were given pre-lacteal feeding (water with old jaggery/sugar/honey, castor oil) to initiate suckling and to complete defecation of meconium. According to the tribe members, it leads to jaundice and abdomen distension/swollen stomach. The colostrum was not given to neonates and discarded by 81% of mothers. The primary reason for this is that the first milk is a mixture of dust that was formed and cloggedin the mother’s womb during pregnancy. The colostrum was discarded with the initiation of elderly female close affinal kins like mother-in-law, grandmothers and relatives. Only 16.5% of literate mothers and 7.1% of illiterate mothers who were given home-based childbirth had fed their neonates with colostrum as they were continuously exposed to medical health personnel like ANM/AWW/CHW. At the same time, there is a record of 100% of immunisation, which is found to be satisfactory.
The recognition of neonatal illnesses confirming as danger signs by the community members and their corresponding health-seeking behaviour was also documented in the study. In these, the highest percentage of newborns (74.7%) were affected with red and white skin pustules, and watering from eyes, followed by cold bodies (56.0%), cold and cough (50.7%), swollen stomach (29.3%), rashes in private parts (24.0%), difficulty in breathing (22.7%), the inability of suckling (20.0%), diarrhoea and fewer body movements (18.7%), fever (9.3%) and the least affected with fits/eclampsia (6.7%).
Under the treatment-seeking behaviour, ethnomedicines were highly administered to the neonates who suffered from fits/eclampsia (100.0%), cold bodies (83.3%), umbilical cord infection (85.7%) and local infections (eye, ear, mouth, skin pustules—75.0%).
The neonates felt relieved after seeking treatments from the PHC/ANM/AWW for illnesses like cold and cough (44.7%), difficulty in breathing (52.9%), the inability of suckling (46.7%) and fewer bodily movements (64.3%), which is a modern medicine-based treatment with no cost.
Due to the increased severity, diarrhoea (64.3%), difficulty in breathing (17.6%), fever (14.3%), the inability of suckling (13.3%), cold and cough (13.2%), swollen stomach (9.1%), cold bodies and fewer bodily movements (7.1% each) and local infections (1.8%) were treated in private hospitals with an expenditure of ₹1,000 to ₹10,000. Like many Indian tribals, neonatal illnesses were treated mostly with home remedies and by the traditional healer, while the rest were treated by administering modern medical healthcare medicines (Mishra, 2019). In the case of traditional medicine failure, the neonates were taken to consultation under medical practitioners’ care. Modern medical healthcare treatments were sought only when the severity was self-assessed as a ‘critical situation’.
Discussion
This study provides crucial insights regarding tribal neonates’ health. This study was one of the few studies that documented meanings for the socio-cultural importance of traditional newborn healthcare practices among Parengi Porja, a PVTG predominant in the hilly forested areas of Eastern Ghats of Andhra Pradesh, India, by using a community-based observational study design with the qualitative approach. The characteristics analysed were the place of delivery; umbilical cord care practices and its anoints; bathing practices; skincare; oral care and eye care (pre- and post-bathing practice); pre-lacteals, colostrum and breastfeeding practices; thermal regulation care; newborn clothing; purification rites; immunisation practices; identifying the danger signs/illnesses; and treatment-seeking behaviour in the neonates. The findings that emerged from our study are described here.
Place of Delivery
In the study, of the 105 neonates, 90.5% were born at home. A majority of deliveries were assisted by TBAs. The choice of place of birth as home was determined by socio-cultural custom. Tribal members going against this practice were required to pay a huge amount of ₹1,000 to the village headman as part of breaching the cultural custom transcending down from the generations.
A mother of a 2-week-old neonate said,
‘We are desi log (adivasi people) we should not give birth outside the home as it is an “impure practices’ (Interview).
A mother of a 5-week-old neonate said,
Until the sutranimaizi(TBA) confirms our deliveries going to be safe or difficult, by testing us with the 10 drops of oil putting in the middle of the chest region. If oil touched directly on the navel region, then it’s a “safe delivery”. Otherwise, the sutranimaizi suggests us to go to hospital delivery which is a burden to us. focus group discussion (FGD)
Only 9.5% (10) of the deliveries were institutional deliveries. These women said,
We had complications like not urinating, baby touching the chest region, breech babies. We had informed same to village headman. After taking opinions from the village members, we are imposed of Rs.10000/-. With this amount, the celebrations occurred by giving feast and alcohol on the 15th day of my neonate. Also, we paid Rs.20000/- for labour charges in the hospital. (FGD)
It is difficult for them to predict the delivery due period. They felt that predicting the baby’s due is not in their hands. The complications were managed with assistance from the TBA. During the complicated labours that lead to death, access to a vehicle was a problem. Of the 10 women, a quarter of women reached primary healthcare centres by vehicles other than ambulances. Women in complicated labour were carried by men to a certain distance to the motorable road and then taken in available vehicles to the hospital. Almost every respondent and family stressed out that there were problems in transportation availability. There is no cellular phone connectivity due to weather conditions. Even when the ambulance was contacted, it took 2–3 hours to reach the village. In the case of poor weather conditions and prior call by others, the ambulance service may be refused outright.
Umbilical Cord Care practices: Cutting, Anoints, and its Beliefs
In the study, the mothers were found taking squatting positions on gunny bags to have a safe baby delivered on it. The baby was separated by the use of a sterilised new blade (72.4%) for cutting of the umbilical cord in all the home deliveries, which was an encouraging finding. The umbilical cord was cared much from the time it was separated from the placenta. They apply many materials to the cord stump of the newborn for early drying and fall-off, as it is viewed as superfluous and highly dangerous if left out untreated on the child. It was observed that there was a great significance for childbirth artefacts that are used directly or indirectly to cut the umbilical cord.
A mother of a 2-week-old neonate said,
only after the placenta was delivered, I was allowed to cut the umbilical cord (bommilli) of my son leaving 2-4 cms away from the navel region with a sterilized blade after touching it to sterilized artifact namely arrow. It is a kind of prayer to our ancestral deity (pidhordevatha). Otherwise, the newborn will be inflicted with fever or wound in the umbilical cord region. (FGD)
A mother of a 7-week-old neonate said,
‘I had cut my girl baby’s umbilical cord with a sterilized new blade after touching it to sterilized sickle, Then the umbilical cord was tied with thread smeared with turmeric’ (Interview).
After giving the first bath that is soon after childbirth, the umbilical cord was dressed with turmeric (Figure 1) mixed with warm oils (niger oil/castor oil/coconut oil). On the subsequent days, the umbilical cord was found dressed with different materials like ashes prepared out of spider web, bamboo mat, cloth, coconut shell, sivana dal leaves, red colour pot’s powder to early dry and fall off from the newborn.
The Umbilical Cord was Tied with Thread Smeared with TurmericPaste.

A mother of a 3-week-old neonate said,
‘I have used different materials on the umbilical cord stump for early dry and fall off. Otherwise, it could harm baby, as partial dry is a call for flies and ants to eat on the baby’s navel portion’ (FGD).
To avoid delay in cord-cutting, the artefacts were sterilised (Figure 2), which was also an encouraging finding. But the umbilical cord being dressed with ashes of different materials, which are the sources for serious infections like tetanus, is not an encouraging finding (Pati, 2014).
The Arrow and Sickle were the Artefacts Usedby Parengi Porja Tribe during ChildbirthingTime to Cut the Umbilical Cord.

Bathing Practices
After awakening the babies, the babies were wrapped in cotton cloths. Following this, the new mothers buried the placenta in the backyard of the house. Then they took a hot water bath by applying turmeric paste, ragi flour to the body. Next, all the babies born at home were given a bath and scraped off vernix with turmeric paste (Figure 3) by the new mother immediately, which is considered a cleaning procedure. But it was not the same for hospital-born babies. But, even in hospital deliveries, upon returning from the hospital, both the mother and child were bathed before entering the house. The entire process of childbirth was viewed by the people as a polluting process, and therefore both the mother and the child have to be cleaned as soon as possible to avoid bites of poisonous creatures like scorpions, millipedes and insects. Many of the mothers, elderly female close affinal kins like a mother-in-law, grandmothers and TBAs reported the same, as bathing a newborn baby will keep many poisonous creatures away. These bathing ingredients are considered ‘anti-infective materials’.
A Parengi Porja Postpartum Mother Bathing Her 1-day-old Newborn.

A mother of a 4-week-old neonate quoted
‘I washed the baby with ragi powder that removed vernix, then I had smeared turmeric. After wiping the wet, the newborn’s body should be compressed warm oil to keep away termites and poisonous creatures’ (Interview).
To avoid such wild circumstances, the neonates are regularly given all these essential precautionary steps for 10 weeks to avoid skin pustules in red (dangerous) and white colour (non-dangerous) that are formed due to warm foods intake by the mother during her pregnancy. It is important to be noted that the early bathing ritual is a social custom. This is widely practised even in India, Pakistan and Nepal, where birth is considered as impure, so it is necessary to give a bath within six hours of birth (Carlough and McCall, 2005; Kesterton and Cleland, 2009; Penfold et al., 2010; Seyal et al., 2011).
Oral care and Eyecare (pre- and post-bathing practices)
In the study, there is a high prevalence of cleaning the mouth and removing mouth thrush with machi kaya (chebulic myrobalan-myrobalan) and tanikaya (Terminalia berecilla-bibhitaki). These two are widely used in many parts of India and are considered as‘natural immunisers’ that keep newborns and children away from fevers, cold and cough. It was also observed that it activates the capacity of suckling, as strongly believed by the people (Van Hollen, 2003). It also prevents the formation of Epstein’s pearls, which are small white or yellow cystic boils that are often seen inside and outside the upper portion of the jaw, especially newborn infants; usually occurs for 65% to 85% of newborns (Pati, 2014). Nevertheless, the newborns’ family members were worried because the cysts slow down suckling, and if not treated at the earliest, they can spread to other parts of the mouth.
A grandmother of a 5-week-old neonate said,
‘From generations, cleaning the newborn’s mouth with myrobalan and bibhitaki paste are of utmost importance otherwise leads to wound in the mouth, then the baby goes starvation means cannot suckle (breastmilk).’ (Interview).
There is an existence of a common practice to remove excess water in the body by applying indigenous black kohl, ash prepared out of burnt coconut shell or coffee seeds, on the smooth portions that include newborns’ eyes, head, palms, soles. The mothers believe that it helps to remove excess heat, water and cold. Otherwise, the eyes will always appear with ‘eye gunk/eye discharges’ in green/yellow or white. The eye gunk in green and yellow colour is considered dangerous, and the newborns are treated by giving honey or liquor as an immediate ethnomedicine available at home. The eye gunk in white colour is viewed as a sign that the body, head and eyes are in normal condition.
Nearly 90 mothers said,
‘We have smeared smooth body portions of the baby (palms, legs, soles, ears, and head) with black kohl prepared in-home help to avoid insect bites and removes excess heat or cold. This also keeps newborn away from evil eye afflictions’ (Interview).
One of the possible explanations is that applying black kohl on the hands, soles and body is not a harmful factor. But the indigenous black kohl application in eyes should be discouraged, as it more or less leads to eye infections.
Pre-lacteals, Colostrum and Breastfeeding practices
In the study, the use of pre-lacteal feed (nearly 90%) before colostrum feeding was highly prevalent. According to them, the pre-lacteals would largely help in the excretion of meconium (murri). Meconium is a dark green faecal matter that comes for 2–3 days from childbirth. Otherwise, the newborns will be affected by jaundice, and their stomachs will be filled with gas that leads to death since it will not easily be treated with either ethnomedicine or modern medicine.
A mother of a 3-week-old neonate said,
I fed my baby first with castor oil and jaggery/sugar water on early mornings subsequently to complete defecation of meconium and inuntil the faecal turns to yellow which was seriously advised by my TBA and elderly female family members. So, within three days green faecal (meconium) stopped and came yellow, then only I breastfeed my newborn. (Interview)
Then, 85.0% of newborns were not given colostrum. The primary belief was that it looks dense and also stops the excretion of meconium that leads to indigestion. Due to this reason, the neonates were not fed with colostrum/first milk. The second belief is that the Parengi Porja new mothers discarded colostrum in the name of sacrifice to ancestors/evil spirits who afflict the neonates with illnesses. After probing into this, based on the birth timing of the newborn, the colostrum was discarded in different mediums in the name of sacrifice. That is, colostrum discarded on the cloth when the baby was born in the early morning; on the jackfruit/mango leaves when the neonate is born in the day hours; discarded in a cowshed when the birth occurred in evening hours and discarded on the broomstick for the childbirths that occurred in the midnight.
A TBA told
‘The feeding of colostrum would not help neonate to survive. If alive then will grow into an unproductive adult as a person takes less food due to the indigestion problem that ultimately gives less strength’ (Interview).
Only 32.4% of newborns were breastfed within 3 days from the day the child was born. The rest of them (67.6%) were breastfed after 3 days from childbirth. All the mothers who delivered in the hospital had given colostrum within 30 minutes from childbirth, as doctors/nurses have given them tablets after which they felt heavy in breasts and then breastfed the neonate.
A mother of a 1-week-old neonate said,
‘I am feeding my baby today, as I was constantly insisted by mother-in-law as not to feed within three days from childbirth. She constantly threatened me as separating me from my husband, if feed so’ (Interview).
The feeding of pre-lacteals and colostrum discarding should be discouraged by providing awareness of its effects on the child. The mothers who had reported their newborn death due after feeding colostrum, their antenatal care and morbidities should be rechecked to confirm that colostrum does not cause death.
Thermal Regulation Care
Newborns are vulnerable to change in temperature and should avoid exposure to cold and circulation of overheat in the body. The Parengi Porja tribe try multiple ways to keep newborns’ warm, confirming that it is important to give thermal care to avoid exposure to cough and cold and boils. On perceived benefits of thermal care, the newborns’ were being massaged with warm coconut oil all over the body to remove excess heat in the body (Figure 4). They also apply garlic oil, that is, 3–4 garlic cloves popped in castor oil, on the chest region to avoid phlegm formation and exposure to cold and cough. Then the newborns’ are always found wrapped in woollen clothes during cold and rainy hours. The newborn is found to be kept clean. The child nappies (made from cotton sarees) are washed with hot water regularly, whereas the mattresses and woollen clothes are washed in streams every 3 days (Figure 5).
A Postpartum Mother Smeared Her Palm with Niger oil and Warming it on Slowburning Charcoal to Give Warm Compressions to the Newborn.

A Postpartum Mother Washing Her Sleeping Mat, Clothes and theNewborn’sClothes in the Stream

About 15–20 mothers, whose neonates were not exposed to any illnesses, said,
‘Wrapping with PROPER warm clothes and warm oil compression on the neonate are most important to be away from cold bodies to fever, cold, cough and dryness of the skin’ (FGD).
In the study, giving utmost importance to thermal regulation care for newborns is an encouraging finding. Then the practising of massages with different oils to remove excess heat and cold signifies that the knowledge should be appreciable.
Immunisation Practices
Immunisation of children is essential to prevent childhood illness, morbidity and mortality. Immunisation is a way of protecting the child from infectious diseases (Ventola, 2016). Under the mandate of the Government of India, the health workers of the respective village had recorded the sex, time, weight, height and head circumferences in the duty register and submitted the same to the regional ICDS office. The newborns were vaccinated with the first dose of BCG+ Hepatitis-A+ DTap+ OPV by the ANM within2–4 days from childbirth. All the Anganwadi workers are successfully informing the ANM through phone calls soon after the child is born in the villages. The ANMs are sincerely advising the pregnant mother and her family members to get their children vaccinated as per their age. It was observed that the mothers hide their newborns to avoid injections from ANM. But when they find newborns are weak, then they search ANM to get vaccinated.
A mother of a 2-week-old neonate said,
‘I hidden in the backyard to avoid vaccination, but soon after my newborn was respire like snoring and groaning then I had informed my Anganwadi worker who suggested taking injections. So, I have only contacted ANM for vaccination during her visit to the village’ (Interview).
Overall, all the newborns were found vaccinated (100%) without fail, which is an encouraging finding. Many of them reported that they were frightened to care for the newborn during and after vaccination.
Newborn Purification Rites and Reasons for Adherence
The Parengi Porja tribe observe a series of purification rites on the third, fifth, sixth and 10th or 11th day after childbirth. The first purification ceremony is andidharbai/satrengchigalbar that takes place on the third day of childbirth. The disari(local medicine man-cum-priest) performs the ceremony at home, which signifies that the mother and child are ‘purified’ from their past sense of life and are integrating into society. In this process, at first, they erected a threshold with a grass plant, namely satreng (Figure 6), which was collected by the newborn’s father’s parallel cousins. This is erected near the heaps of cow dung termed as a sacred place in the respective homes. After lighting the camphor by the disari, the newborn’s family passed through this threshold, which marks that the child is welcomed into the society. Following this, the disari had thrown away the threshold in the backward direction without bringing it to the front.
The Preparatory Ground for First Purification Rite SatrengaChigalbar.

On the third day itself, the second purification rite is performed, which signifies that the newborns should grow into strong and healthy adults. In this, the newborn girls were dressed in headwear or turban made out of cotton cloth only after touching it to water pot or firewood; in the case of boys, the turban was touched to oxen yoke and water carrying pole. On the fifth day, the purification was performed at the streams for jala or pathalakamminidumma (Figure 7) in their village to avert diseases like diarrhoea. After this rite, the natal kins of the new mothers come to see the newborn with choul and sol thoppa (rice and ragi sweets, respectively) and the sum of ₹300 to ₹500.
On the Fifth Day, the Second Purification Rite is Performed at the Streams (for Jala or Pathalakamminidumma).

On the sixth day, they perform banaborbaur (Figure 8) by lighting the wild camphor in the crossroads for begetting the ancestors blessing on the child to grow out of deformities, which isalso a welcome call for the village members for the feast. Following this, in the afternoon, the mother with the newborn was made to sit outside the house under one corner of the roof. This rite is called antadhori, that is, putting the pelvic thread on the newborn. This ritual is intended to avoid the supernatural afflictions that surround in and around the house. After this, they performed another ritual mandumma to invoke the ancestors to safeguard the newborns from evil afflictions. On the 10th or 11th day, the prayers were offered to the ancestral deity (pidhordevatha—Figures 9a and 9b) in the form of sacrifices, only after which the child is dressed in the new clothes gifted by the kins and the kith.
On the Sixth Day, They Perform Banaborbaur toGetAncestors’ Blessings to Ensure ChildGrowswithoutDeformities, and also a Sign of Welcoming the Village Members for the Feast.

Ancestral Deity Pidhordevatha.
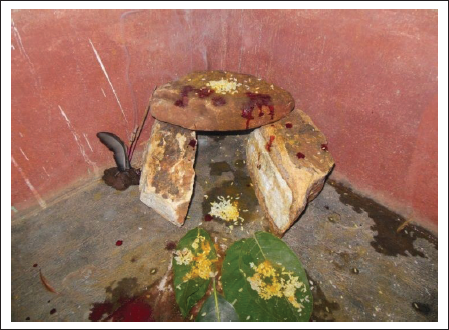
The Fowl Offerings Made to the Ancestral Deity were in an Earthen Pot on the Hearth, which will be Shared by Members of the Same Lineage Name of the Newborns’Family.

A mother of a 4-week-old neonate said,
Until the purifications rites are performed, we are not allowed in the kitchen, not to go out of the home, and not given salt, red and green chilies, green vegetables, goat’s meat, and chicken muscle and bones… Breeching these practices, expose us to postpartum illnesses, reduces milk supply in mother, and trouble in uterine retention. (Interview)
With the experience of elderly women and TBAs advice, the new mothers adhere to these cultural practices.
Identifying the Danger Signs
The recognition of neonatal illnesses confirming as danger signs by the community members and their corresponding health-seeking behaviour was also documented in the study.
A mother in an interview said, ‘I found my child’s body turning into blue and black colour with cold temperature then I confirmed it as breathlessness’.
Likewise, a majority of mothers identified the danger signs at the earliest with the help of their elderly female family members and cousins, which is an encouraging finding. The severity of illnesses varies depending on symptom types. Irrespective of the high or low degree of severity, they sought both ethnomedicines and modern medical care treatments based on the increased severity.
Treatment-seeking Behaviour of Neonatal Illness
The recognition of warning signs and appropriate treatment could be life-saving. Almost all the maternal mothers, local birth attendants and caregivers seemed to have a certain kind of knowledge in managing the risk factors of newborn danger signs.
A TBA told,
We strictly suggest mother wrap neonate in warm clothes after massaging body with warm oil. Also, advice gives breastmilk in baby spatula when the baby is unable to suckle in the earliest few weeks. By wrapping baby properly will avoid dangers of cold bodies, cold and cough, fevers; then massaging neonate with warm oils will avoid skin pustules, watering of eyes as it removes excess heat in the body; giving breastmilk in baby spatula can avoid baby starvation, not expose the child to eclampsia/fits, increases bodily movements and also clears up any dust in the throat by that baby can inhale and exhale properly. Only a few are following these precautionary steps.
Most of the illness episodes were cured with ethnomedicines. The modern medicine treatments were sought when the situation demanded it due to the severity of illness, was an encouraging find. Studies have reported that adequate healthcare-seeking from skilled healthcare providers leads to fewer deaths and relief from morbidities. There has been a record of 77 deaths per 1,000 live births in the Parengi Porja neonatal mortality rate, because of not giving modern medical-based care for fits- and fever-affected neonates. The families with poor socio-economic status are found unable to seek treatments from healthcare institutions. It is also a widespread belief that until the umbilical cord falls off, the neonates should not go out of the threshold. Due to this reason, most of the neonates were not taken to treatments in healthcare institutions like PHC and private clinics despite the neonate’s severe health condition, which needs to be discouraged.
Conclusion
The traditional healthcare practices have highly impacted the lives of Parengi Porja tribe due to their existence and continuity in their socio-cultural pattern. But time and resources had changed a lot, and due to this, it is important to intensify community-based newborn care strategies and make strong linkages between health facilities and the home to effectively handle risk factors that often lead to deaths. This calls for the immediate strengthening of focussed health education on newborn care practices, especially during prenatal care, to mitigate all health problems.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.