
Abstract
The current focus on the transmission of COVID-19 infection all over the world may probably distract public attention from psychosocial consequences of the outbreak in the affected individuals and in the general population. However, there is limited empirical information about its psychological impact on the people of diverse regions and nationalities. Hence, the study aims to understand the psychological impacts of COVID-19 and associated pandemic distress on the demographically diverse Indian population and the ways people are adopting to cope with them. A total of 261 respondents aged 18−73 years, representing more than 17 states of India, filled an electronic survey questionnaire. Survey research methodology following the mixed-method approach adopting both qualitative and quantitative methodologies was adopted. Results of the first phase of the study indicated significant psychological impacts of the COVID-19 pandemic on respondents during the first three weeks of lockdown, especially the pandemic anxiety and social isolation. Physical health, fitness, self-care, family connect, learning of the new skill sets and self-growth opportunity were found to be some of the functional ways to cope with pandemic in this phase, whereas passive acceptance was expressed as a dysfunctional strategy to cope with pandemic coupled with negative emotions such as fear, anxiety, frustration and irritability for others. However, phase two of the study with 20% of respondents in the sixth week of lockdown revealed the exhaustion of the learning phase, limited efforts for self-growth and increasing anxiety and frustration. A great proportion of respondents expressed fear of losing global business scenario and its direct or indirect impact on them. A need for consistent and dedicated mental health care was recommended.
Introduction
Multiple challenges keep pushing themselves on people, ranging from personal to professional. One such challenge engrossing the entire world in its clutches is the COVID-19 outbreak which was declared by World Health Organization as pandemic, raising widespread panic and causing increased anxiety and distress in the minds of people. The novel coronavirus (2019-nCoV), believed to have been originated in a wet market in Wuhan, Hubei province, China, has gained attention nationwide and globally (Xiang et al., 2020), creating a worldwide physical health emergency, along with likely impacts on global mental health across almost all age groups. Global media, local and international health organisations (including World Health Organization), epidemiologists, virologists and opinion makers put out information, recommendations and updates on COVID-19 and its lethality. Unpredicted negative events like pandemic are very challenging for people in general, making it difficult to keep them to remain afloat. Loss of jobs, confinement and increased physical space between people have exposed many of them to the risk of entrapment in a loop of negative emotions. Media coverage has highlighted COVID-19 as a unique threat, which further exaggerates the panic, stress and the potential for hysteric reactions (Kim & Su, 2020). Although people are adapting to a new normal lifestyle to keep themselves physically safe from the impact of virus on physical health, little is empirically known about its psychological impact in terms of distress, anxiety and depression (Wang et al., 2020). Nevertheless, the burden of this infection on global mental health is currently being neglected by policymakers and health organisations (Torales et al., 2020).
Uncertainty and Associated Psychological Issues
The virus successfully infiltrated the life of every person with or without infecting them. The increasing number of patients and suspected cases, combined with the increasing number of outbreak-affected provinces and countries, has elicited public worry about becoming infected. The current focus on the transmission of COVID-19 infection may distract public attention from psychosocial consequences of the outbreak. The unpredictable future of this epidemic has been exacerbated by myths and misinformation, often driven by erroneous news/social media reports and the public’s misunderstanding of health messages, thus causing irrational fears among the population (Bao et al., 2020). The uncertainty and low predictability of COVID-19 not only threatens people’s physical health with restricted mobility, but also affects mental health, especially in terms of emotions and cognition (Li et al., 2020). The emerging mental health issues related to this global event may evolve into long-lasting health problems, isolation and stigma. Hence, calls for global health measures to address psychosocial stressors, particularly related to isolation/quarantine, fear and vulnerability are imperative (Torales et al., 2020). The dramatic increases of public fears and decrease in social and economic activities may trigger psychosocial sequelae (Kim & Su, 2020).
Social Confinement and Mental Health
As the medical community is continuously attempting for a breakthrough, the consensus has been that the only way to protect people from this virus is to limit the social exposure. With the continuing spur in the numbers of fatalities, various health authorities have advised the public not to step out and stay at home as a basic means of limiting people’s exposure to the virus. This sudden restriction on movement has imbibed stress in people and disrupted their lifestyle and physical health (Chen et al., 2020). The immediate confinement as a precautionary measure has left everyone in a state of fear and uncertainty. Quarantine has put a hold on the human touch and face-to-face connectivity between people. Fear of death and falling sick has triggered an upsetting scenario. Patients with confirmed or suspected 2019-nCoV may experience fear of the consequences of infection; those in quarantine might experience boredom, loneliness and anger. The indirect consequences of lockdown have led to a slowdown in the economy, with many people across the world losing their livelihoods. Human confinement has put a question mark on the longevity of large restrictions on movement. Social distancing norms have increased the physical boundaries and impacted the way humans behave in social spheres, with direct implications on daily life and mental health (Ornell et al., 2020). In the absence of peer support, regular reporting of fatalities has shot up the anxiety levels. The situation could be a little forgiving for those who prefer to keep their human engagements to bare minimal; however, it is quite challenging to those who thrived socially. Therefore, it is possible to have a varied attitude and feelings on this scenario. Despite this progressive grim divulgence, people are increasingly finding ways to keeping themselves motivated and afloat. These psychological changes can be monitored through emotional and cognitive indicators such as social risk judgement and life satisfaction (Li et al., 2020).
Somato-psychic and Psycho-somatic Outcomes
In any biological disaster, themes of fear, uncertainty and stigmatisation are common and may act as barriers to appropriate medical and mental health interventions (Xiang et al., 2020). With the fatal nature of the virus coupled with increasing number of confirmed cases and deaths, the outbreak threatens the mental health of the population. A large number of people had emotional breakdowns, felt helplessness, fear, anxiety, depression, guilt and nervousness (Zhou, 2020). Faced with potential disease threat, people tend to develop avoidant behaviours (e.g., avoid contact with people who have pneumonia-like symptoms) and obey social norms strictly (e.g., conformity) (Li et al., 2020). Furthermore, symptoms of the infection, such as fever, hypoxia and cough, as well as adverse effects of treatment, such as insomnia caused by corticosteroids, could lead to worsening anxiety and mental distress (Xiang et al., 2020). Rajkumar (2020) explored the literature associated with mental health issues in COVID-19 and found that symptoms of anxiety and depression (16%–28%) and self-reported stress (8%) were common psychological reactions to the COVID-19 pandemic along with sleep disturbances.
Lifestyle Management Through Resilience
Coronavirus has challenged the world in a way where survival has become the biggest question; interventions to build resilience and provide support to each other are strongly desirable. The novelty of the virus and its sudden emergence has caused heightened incidents of panic, fear and stress among people across the globe. Confinement, loss of usual routine and reduced social and physical contact with others were frequently shown to cause boredom, frustration and a sense of isolation from the rest of the world (Brooks et al., 2020). The spur of negativity fuelled by forms of media can lead one falling into a chasm of negative thoughts that is further fuelled by changes in the lifestyle. Although many people are taking up a hobby and utilising this time in a productive way, it still is challenging to stay afloat. There is an immediate need to seek and build psychological resilience as cases are piling up every day, leading to more people slipping into anxiety. With little help available due to the norms of physical distancing, there lies multiple challenges for us.
This pandemic has two faces, having both functional and dysfunctional impacts on people. It might take a longer time to assess the actual physical impacts of the COVID-19 pandemic, but the assessment of perceived psychological impact is still necessary to safeguard people from further distress.
Hence, this study empirically explores the psychological impact of the COVID-19 pandemic, associated distress and functional/dysfunctional strategies adopted by people to cope with it across the demographically diverse population of India. It also analyses the way people of diverse age groups are using their available time for different activities during this phase of social confinement to cope with pandemic-induced stress with a special focus on gender-based analysis.
Materials and Methods
Sample
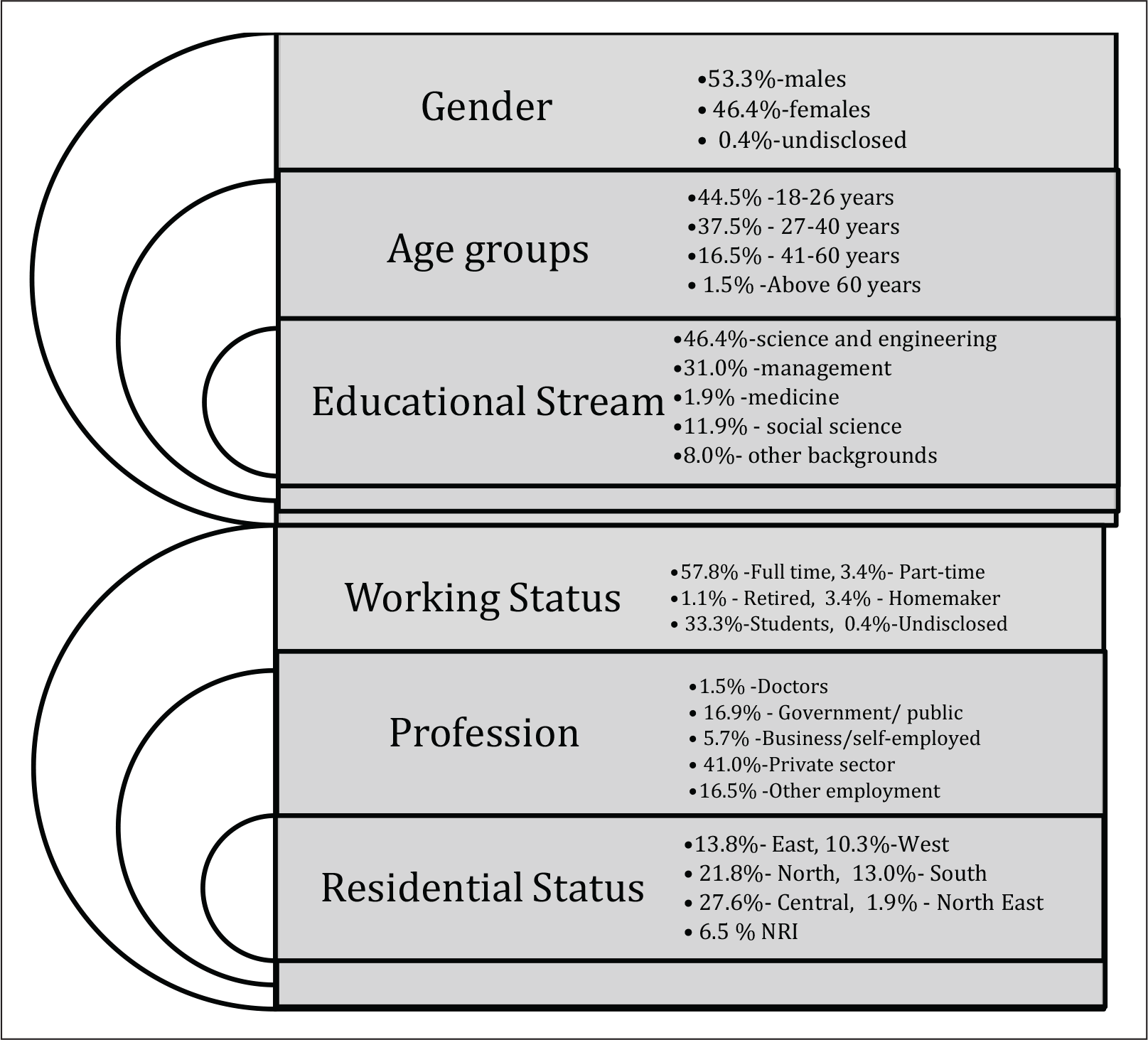
A total of 261 respondents, representing diverse geographical zones of India, according to the State Reorganisation Act, 1956, filled an electronic survey to best describe how people across different socio-demographic dimensions are perceiving the impact of current pandemic stress/anxiety and strategies to cope with the situation amidst COVID-19. Respondents were approached with personalised invites inclusive of the web link to the semi-structured comprehensive electronic questionnaire through social media and digital platforms such as emails and WhatsApp. The snowball sampling technique was used for the study, encouraging respondents to roll out the survey to as many people as possible, over a specific period between weeks one and four of April 2020, when India, as a country, was observing national lockdown to curb the spread of the COVID-19 pandemic. The socio-demographic variables included age, gender, qualification, nationality, zones of India and type of employment. All the participants were between 18 and 73 years of age. Sampling details are given in Figure 1.
As the psychological impacts of pandemic and associated lockdown are likely to change with time, phase two of the study was also planned in which 20% of the respondents were approached electronically with a follow-up survey to report their subsequent mental state based on structured questions which were subjected to qualitative analysis.
Tools
A comprehensive electronic survey tool ‘Pandemic Distress & Coping Scale’ was especially designed for this study. The scale was having 25 items for assessing different areas with reference to the pandemic, that is, psychological impact of pandemic stress and analysis of functional and dysfunctional coping strategies. Multiple response formats including open-ended, multiple choice and 5-point Likert-type rating scale format were used. Both qualitative and quantitative analyses were carried out using content analysis and SPSS 20 to analyse the obtained data. The reliability coefficient through Cronbach’s α was found to be 0.776.
Results and Discussion
Responses were electronically collected from 276 individuals, out of which 15 were invalid, and eventually 261 respondents were included in the final qualitative and quantitative analyses (acceptable response rate: 94.56%). The obtained data were coded and analysed using SPSS 20 statistical software and NVivo for qualitative analysis. The demographic profiles of the sample are given in Figure 2 as mentioned in the sampling section.
Gender-based Analysis in Managing Time
Gender discrimination largely becomes a source of conflict in work division among working couples at the time of pandemic when everyone is going through anxious mental state, and household support is either unavailable or considered unsafe. Respondents were asked a set of questions regarding how they are spending their daily time during the lockdown phase and resulting social confinement when physical mobility and social interactions outside family were constrained.
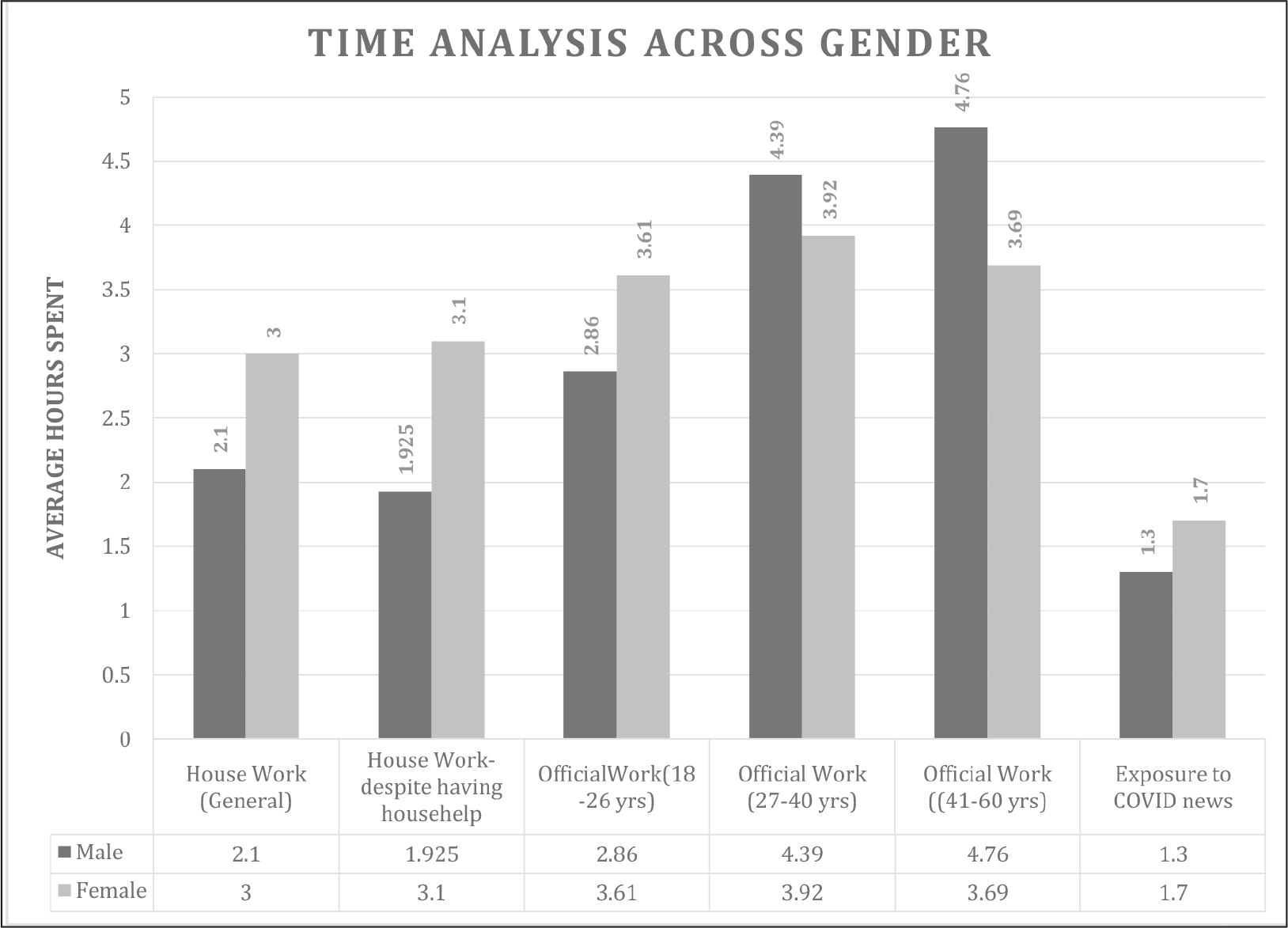
Results indicated that in the absence of any external support during lockdown, on average, females were spending 42.86% more time on household management than males, showing visible gender discrimination in the distribution of household work across all population groups. Even when house help or any other kind of support for housework was available, females were still spending 61.04% more time on household work than males, which is double stress, especially for women working from home.
Dhar et al. (2019) suggested the need for a strong policy framework to address the issues of gender equality in developing countries and to improve the status of women by creating conducive working conditions at home and workplace. Contemporary studies also found that women have to bear a larger share than men for household work in China and United States, in spite of the fact that these developed countries have gone through a transition from social and legal support for male supremacy to legislation against gender discrimination. However, uncertainty still prevails regarding how long this gender-based division of household work will continue (Zhang & Farley, 1995). Further, even though Millennium Development Goal 3 focuses on the riddance of gender discrimination in education by 2015, the dream of gender equity still remains unrealised (Singh & Mukherjee, 2018).
Although analysing the differences across gender in different age groups involved in work/study from home, the average number of hours spent on official work/study for the age group of 18−26 years were found to be 26.22% more for females than males. For the age group of 27−40 and 41−60 years, average hours spent on official work/study were 11.99% more in 27−40 years’ age group and 29% more in the case of 41−60 years’ age group. In addition, average working hours in the case of males show a linear increasing trend with age groups.
It was the common observation during early stages of lockdown that people were anxious and hooked to media for pandemic-linked information. Regarding time spent on COVID news/information, it was 26.77% more in females than in males. On average, young females (18−26 years) spent 30.76% more time chatting with people close to them than males in the similar age group. However, it shows a decreasing trend with an increasing age. Besides, males spent 10.43% more time than females in pursuing their hobbies and other personal interest activities, may be because of their limited contribution in household responsibilities. The senior citizens (>60 years) spent 85.95% more time than the younger generation (18−26 years) in meditation/introspection and religious pursuits. Bergan and McConatha (2001) also found that levels of religious affiliation and religious devotion increase with age. Pandey et al. (2020) affirmed that religious intent, values and corresponding actions help to cope with the threat created by COVID-19. These values ranged from love to gratitude, goodness, humanism, sacrifice, self-control, commitment and transcendence.
Functional and Dysfunctional Coping Strategies
Perceived Positive and Negative Impacts of COVID-19.
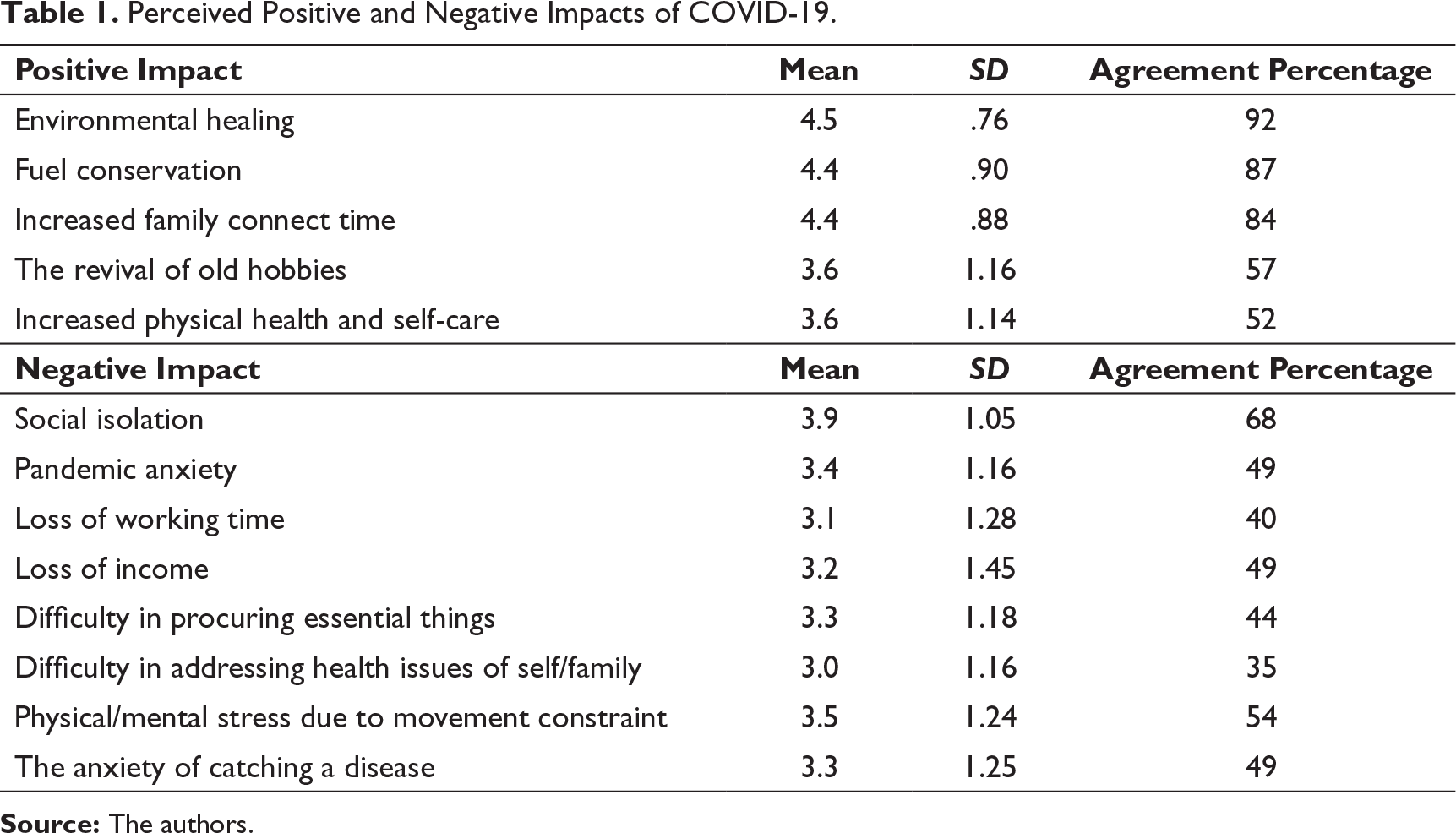
The mean score of the positive impact variables ranged from 3.6 to 4.5, and the mean score of negative impact variables ranged from 3.0 to 3.9. The highest mean in the positive impact of COVID-19 was of environmental healing (M = 4.5), followed by fuel conservation (M = 4.4) and increased family connect time (M = 4.4). More than 80% of the respondents agreed to these positive impacts of COVID-19 in initial few weeks of lockdown. The highest mean in the negative impact of COVID-19 was of social isolation (M = 3.9), followed by physical/mental stress due to movement constraint (M = 3.5) perceived by 68% and 58% of the respondents, respectively. The percentage distribution of the respondents across impacts is depicted in Table 1.
Armitage and Nellums (2020) stated that lockdown-induced social isolation is going to be a serious public health issue among elderly who are already at a higher risk of cardiovascular, autoimmune, neurocognitive and mental health problems, especially depression and anxiety. 1 Further, Nitschke et al. (2020) also reported a major role of social connectedness in promoting resilience as it acts like a buffer against negative physical and mental health outcomes, especially at the times of adverse situation like the COVID-19 pandemic.
Pollution levels in India have always been quite high due to population, heavy traffics and polluting industries, leading to poor quality of air in all major cities. Obtained results in regard to environmental healing and fuel conservation, especially during the early phase of lockdown can be substantiated by results of Tahir and Batool (2020) who stated that global confinement due to COVID-19 and resulting limited transportation is a step ahead towards a greener world with a 0.3% drop in the global emission of CO2 primarily due to limited oil consumption. Lokhandwala and Gautam (2020) also proclaimed that after the declaration of lockdown due to COVID-19, quality of air has shown signs of improvement along with other environmental parameters and substantiated the findings of this study.
Psychological Impacts: Distress and Coping
Mean, SD and Agreement Percentages of Coping with Pandemic Stress.
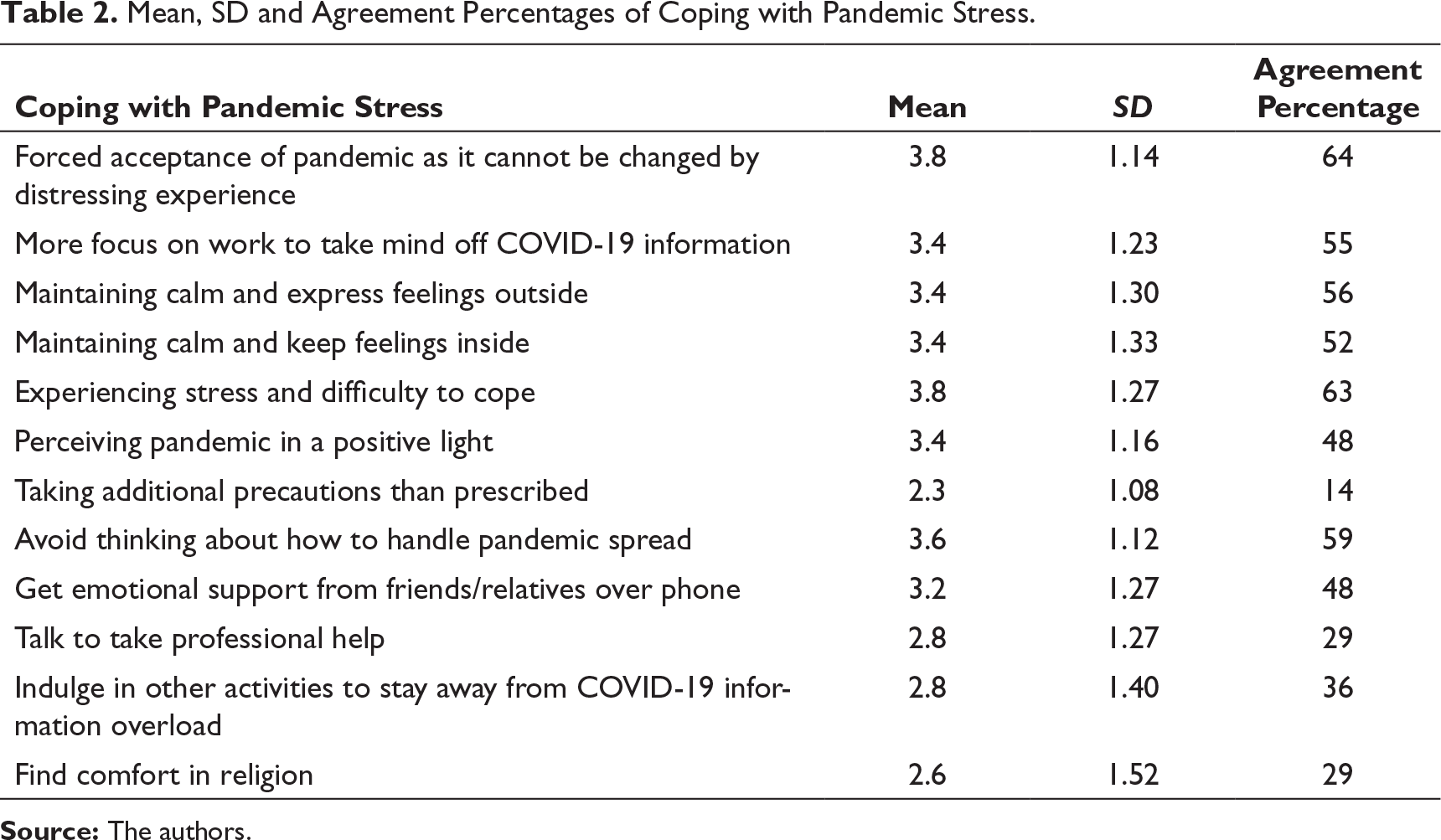
From the individual scores of the respondents for the coping with pandemic stress variables, quartiles were calculated. Of the 261 respondents, 84.3% females reported moderate to high pandemic-associated distress, whereas 74.8% males reported the same; there was no gender-specific differences in coping threshold. About age differences, moderate to high stress was found in 86% of the respondents in the age group of 27−40 years, followed by 41−60 and 18−26 years, and least in the above 60 years category. The coping potential was found to be best in the age group of 41−60 years where 85% had moderate to high coping threshold, which was followed by 41−60 years, with young adults and senior citizens being almost at the similar front. The mean score of coping with pandemic stress ranges from 2.3 to 3.8. The highest mean was found for the forced acceptance of existence of pandemic, as it cannot be changed by distressing experience along with distressing experience and difficulty to cope. A significant observation from the above results is that only 14% of the respondents agree to take additional precautions than prescribed for COVID-19 as opposed to 62% who do not.
In a study by Park et al. (2020), 37% of the respondents reported increased symptoms of post-traumatic stress disorder, and about half of them reported significant changes in their daily lifestyle and functioning, primarily in social interactions, physical activity and time spent on working during the pandemic phase. Hence, there is a need to manage distress and address mental health issues seriously during this phase of uncertainty as increasing levels of stress can cause maladaptive behaviours, posing difficulty to cope with stress and anxiety.1 Another study on Indian population by Jacob et al. (2020) revealed a good percentage of students experienced stress and anxiety about their study and spread of infection. Rosso et al. (2020) in a study conducted on Italian population found the incidence of high perceived stress, insomnia and adjustment disorder which were primarily associated with quarantine and other recent COVID-related stressful life events. Grover et al. (2020) also reported the moderate level of stress by 74.1% of the participants, whereas 71.7% reported poor well-being in Indian respondents.
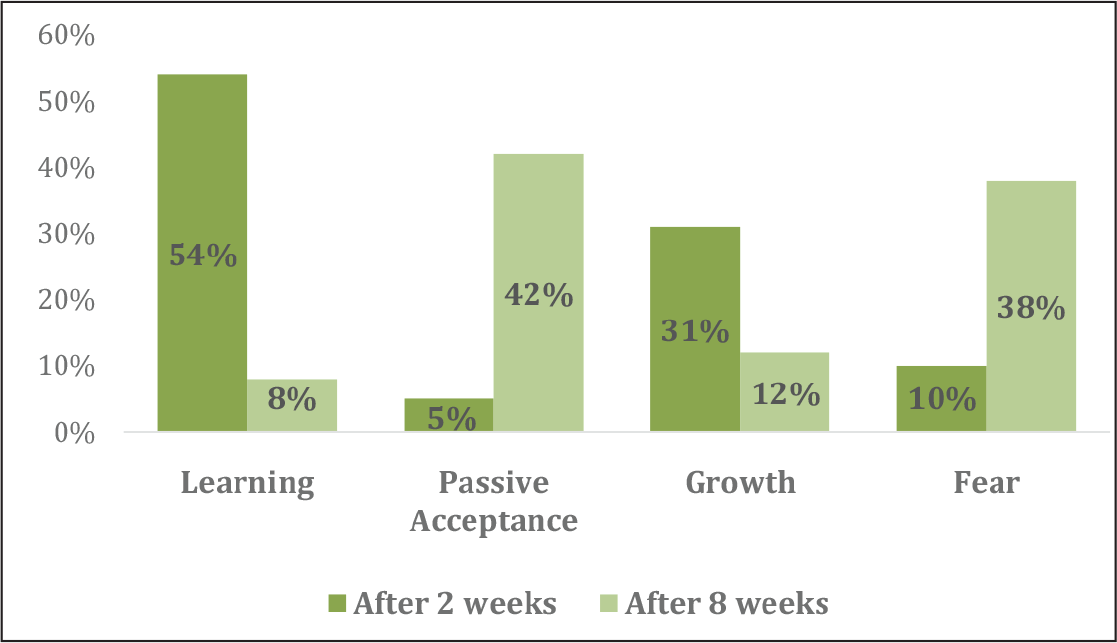
With respect to coping behaviour due to COVID-19-imposed lockdown, 54% of the respondents functionally coped by learning new skill sets through online courses and picking up old hobbies. Almost all respondents made an active effort to cope with this scenario during the first two weeks of lockdown as only 5% respondents passively accepted the situation, by not ascribing any active and functional coping mechanism and spent their time scrolling through social media platforms or sleeping and resting to pass the abundantly available time. Total 31% of the respondents responded optimistically about the change with active functional coping in the form of spending time with family members and reconnecting with old friends, whereas 10% coped with this scenario through negative emotions such as fear, anxiety, frustration and irritability like fear of the unknown future and isolating themselves. Some common responses that could be observed were social isolation, following a fixed routine, strengthening family bonds, being cautious, patient and positive. Some unique responses observed were creative collaboration with peers, documenting the present situation and showing gratitude to front-line workers.
Qualitative Analysis
The electronic survey tool included few open-ended questions to obtain the in-depth information about their psychological state, perceived distress, impacts of pandemic and the efforts they are making to cope with stress. On the basis of obtained responses, people were classified into four major zones as follows:
People simultaneously operate in all the zones during different phases of confinement and pandemic as per their current psychological state. However, there is a likelihood of consistency to have the dominant zone of operation, which will decide how a person is likely to cope with pandemic in a functional/dysfunctional manner and his/her consequent state of mental health and well-being. The key findings of qualitative analysis are given below.
With respect to functionally coping with coronavirus-imposed lockdown, 41% of the respondents were learning a new skill and picking up a hobby which ranged from cooking to gardening to learning a language and reading books. Total 14% of respondents had passively accepted the situation, 42% of the respondents had responded optimistically about the change with the responses like there is a lot of time to rebuilt lost connections and pay attention to one’s hygiene etc., whereas only 3% showed negative emotions such as fear, anxiety and irritability during the first two weeks of lockdown when the responses were taken. The highest frequency of responses mentioned an increased time for relationship building, followed by more of self-introspection and sleeping. There were some unique responses such as low crime rates, spiritual growth and increased productivity during work from home. Gupta et al. (2020), in their study in Nepal, also reported predominant anxiety and depression among participants, due to lockdown and the prevailing COVID-19 pandemic, and suggested a need of expanding the mental health services on a priority basis to provide psychological first aid.
Follow-up Analysis of Psychological State
Follow-up analysis of psychological state of mind during the COVID-19 outbreak was conducted between the sixth and eighth weeks of lockdown in India. All the respondents were electronically approached to respond to the follow-up survey questions.
Total 25% of the respondents reverted to the follow-up questions (N = 65) of which 77.27% of respondents reported change in their perspective regarding functional impacts of social confinement and only 13.63% of respondents’ reported that their perception was almost the same as during the first two weeks of social confinement; a very limited percentage was unsure of any change. On the scale of 10, the self-reported anxiety during the ongoing pandemic phase was found to be 5.44; the index for the likelihood for a mental health issue was 7.16 and the counselling acceptability level was 5.79. Respondents accepted that remaining in social confinement along with pandemic stress was taking a toll on their psychological state of mind, which had seriously affected the mental well-being of people. Behavioural fatigue accumulates with increasing period of lockdown as people get tired of self-regulating, and with such changes, it is seen that there is an increase in boredom and loneliness (Brodeur et al., 2020).
Further, the follow-up survey revealed the exhaustion of the learning phase, limited efforts for self-growth, increasing anxiety and frustration. They also expressed concern for the livelihood of marginalised people and those who were suffering while being stranded at different places, concern for people suffering due to disease, increased fear of catching the disease for self or elderly loved ones in the family, and the stage of hopelessness and despair about how losing a string of economy across the globe. The anxiety about when the situation will improve across the globe and when they will be able to regain the lost freedom to move and interact personally with their colleagues, friends and family was also expressed. A great proportion of respondents expressed fear of losing global business and its impacts. Overall, irrational fears were observed with obsessive concerns and compulsive responses about health and hygiene issues. People who were otherwise learning and goal-oriented in the first two weeks of lockdown showed irrational and fearful behaviour (Figure 3).
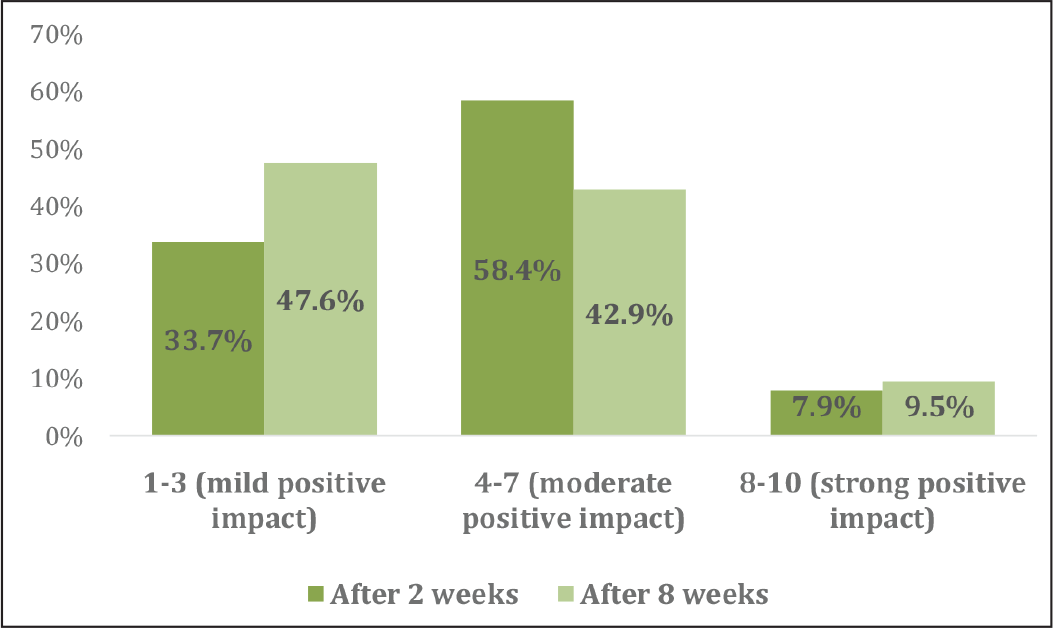
Analysis reveals how the perception of respondents changed over a span of six weeks. Rating 1−3 depicts a mild positive impact which changed from 33.7% to 47.6%; rating 4−7 depicts moderate positive impact which changed from 58.4% to 42.9%, whereas 8−10 depicts strong positive impact which changed from 7.9% to 9.5% (Figure 4).
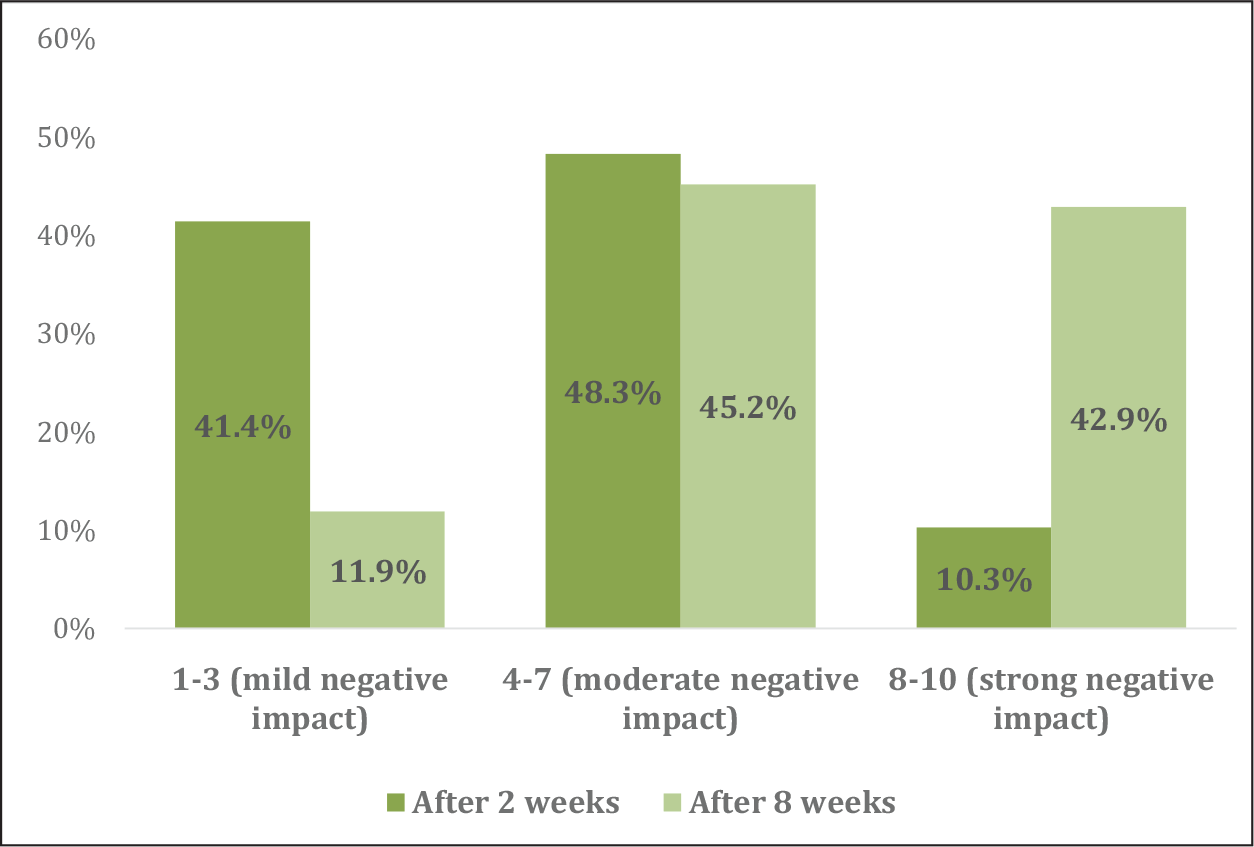
Similarly, for negative impact ratings, the mild negative impact has changed from 41.4% to 11.9%, moderate negative impact changed from 48.3% to 45.2%, whereas strong negative/dysfunctional impact has changed from 10.3% to 42.9%, indicating that perceived negative impact of COVID-19 and associated social confinement increased with time, making it more stressful and difficult to cope for almost everyone (Figure 5).
Conclusion
Coronavirus-imposed lockdown has caused changes in our daily routines. It was observed that women did a larger percentage of housework. There was an increasing linear trend for working hours of men with increase in age. Women seem to fear the consequences of COVID-19 more as evident from spending more average time on COVID news. Social isolation and the resulting physical and mental stress were emphasised by most of the respondents. Senior citizens felt less socially isolated than younger generation, probably due to more family time and being accustomed to limited mobility. Since the younger generation is accustomed to more socialising, social confinement caused them greater stress. However, majority of respondents believed that environmental healing, fuel conservation, increasing family time, revival of old hobbies and increased physical health and self-care were some major positive impacts of this pandemic. Hence, policymakers and public health officials should take into consideration the strategies relating to the pandemic, integrating the issues of psychological well-being, along with physical health (Nilima et al., 2020).
The perception of respondents on positive and negative impacts of COVID-19 changing in a span of six weeks somewhat shows that being in lockdown during the initial period was not as difficult as it started turning during the later phases of lockdown. Although people have found positive and innovative mechanisms to cope with the situation, irrational fears were observed with obsessive concerns and compulsive responses on health and hygiene issues coupled with irrational behavioural tendencies among people who were learning and growth oriented in the first two weeks of lockdown. The way perception change occurred with the increased period of social confinement, a dire need for consistent and dedicated mental health care was observed.
Footnotes
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship and/or publication of this article.