
Abstract
This article examines how ethical innovations of community-based organizations (CBOs) contrast with profit-maximizing healthcare models. Through a multiple case study approach analysing Health in Harmony (Indonesia), Buurtzorg India and Health Center Cecosesola (Venezuela), we identify four key characteristics enabling these organizations to prioritize healthcare access and quality: (a) prioritization of needs, (b) organizational openness and participatory governance, (c) creation of autonomy-supportive environments and (d) trust-building and relationship development. The featured organizations demonstrate how ethical innovation can drive access to quality healthcare. The CBO models provide tested patterns applicable across economic sectors for organizations seeking to become socially responsible agents.
Introduction
The Anthropocene is driven by prioritizing material growth and profit over human and non-human well-being. Despite having the technical capabilities to meet everyone’s basic needs while using far fewer resources, billions remain deprived of necessities while life-supporting ecosystems face accelerating destruction (Hickel & Sullivan, 2024). As powerful actors in the Anthropocene, business organizations significantly contribute to social and ecological ills through extractive models that privatize environmental and social capital while externalizing costs (Marquis, 2024).
The 2023 Universal Health Coverage Global Monitoring Report indicates stagnated access to critical healthcare and rising out-of-pocket costs for people with low incomes. Over half of the global population—4.5 billion—lacks access to basic health services. Since 2015, health service coverage for infectious and noncommunicable diseases has barely increased, with out-of-pocket costs pushing 1.3 billion people into poverty, including 344 million extremely poor (WHO & World Bank, 2023).
Healthcare systems worldwide have different approaches to balancing access, cost and quality. The Beveridge model in the United Kingdom, Spain and New Zealand offers universal care financed through taxation. The Bismarck model in Germany, France, the United States, Switzerland and Japan employs insurance systems funded by employer–employee contributions, often with private providers. Out-of-pocket models in Africa, India, China and South America reflect economic limitations, leaving many without access to care (Osorio-González et al., 2020).
Even relatively well-financed Western healthcare systems face significant challenges, such as pharmaceutical interventions that have shown limited efficacy in addressing chronic diseases and driving unsustainable cost increases (Miles & Asbridge, 2014). Fragmentation stands at the heart of healthcare’s ineffectiveness (Stange, 2009), adversely impacting quality, cost and outcomes (Enthoven, 2009). This systemic fragmentation, embedded in the history and culture of medicine, has created healthcare systems designed around commodities that can be quantified and incentivized rather than relationships that foster trust, hope and healing (Stange, 2009). As McKeown (1979) notes, medical science and services can be misdirected by relying on the erroneous assumption that health primarily depends on internal intervention, leading to indifference towards external influences and personal behaviour, which are the predominant determinants of health. Furthermore, Engel (1977) highlights how medicine’s crisis stems from defining disease solely in terms of somatic parameters, causing physicians to disregard psychosocial issues outside medicine’s perceived responsibility. Systemic issues such as rising avoidable error rates, frequent care scandals and dehumanizing experiences (Miles & Asbridge, 2014) call for a fundamental transformation of healthcare delivery models beyond mere technical solutions.
Vulnerability in healthcare access arises from interactions between individual circumstances, social determinants and systemic factors (Mechanic & Tanner, 2007). Studies link minority racial status, low socioeconomic status and lack of insurance with poor healthcare access (Shi & Stevens, 2005). These vulnerabilities cluster, creating gradient effects where individuals facing multiple risks experience worse outcomes. In the current article, it is argued that profit-maximizing healthcare models are ill-suited to better healthcare access and quality, but community-based models provide tested and well-functioning patterns of solutions.
Community engagement has emerged as a promising approach to providing quality healthcare. Evidence shows that meaningful participation can significantly improve health outcomes among disadvantaged populations (Cyril et al., 2015; Haldane et al., 2019). Effective community engagement involves a complex political process of power negotiation between healthcare providers and recipients, leading to more equitable health systems (Allotey et al., 2019, p. 66).
This article posits that community-based organizations (CBOs) drive ethical innovation in healthcare delivery. CBOs prioritize access to healthcare over profit, create supportive environments and build trust through reciprocal relationships.
The article examines how CBOs deliver accessible and quality healthcare through a multiple case study of three CBOs in diverse contexts—Health in Harmony (HH) (Indonesia), Buurtzorg India (BI) and Health Center Cecosesola (HCC) (Venezuela). We address two key questions: How do healthcare CBOs prioritize accessibility and quality? What organizational characteristics enable this approach?
The analysis reveals distinctive organizational characteristics that allow CBOs to prioritize access to quality healthcare over profit-maximizing. Four key factors have been identified: (a) prioritization of needs, (b) organizational openness and participatory governance, (c) creation of autonomy-supportive environments and (d) trust-building and relationship development.
The article proceeds as follows: First, I describe the methodology and introduce the three case organizations. Then, I analyse the distinctive characteristics of community-based healthcare models, drawing on evidence from the cases. Finally, I discuss implications for broader business transformation, highlighting how these models might inform more ethical approaches across sectors.
Methodology
The study employed a qualitative multi-case approach, analysing three CBOs operating in the healthcare sector but in different geographical and cultural contexts. A purposive sampling strategy was applied to identify CBOs demonstrating a clear commitment to prioritizing access and quality in healthcare.
Primary data collection involved semi-structured interviews with key representatives from each organization, averaging 60 minutes. The interviews explored how CBOs focus on basic needs over profit maximization and build governance structures supporting community control.
Secondary data sources included organizational documents, websites, published studies and archival materials. This supplementary evidence helped validate and contextualize interview findings.
The analysis followed an iterative process, moving between empirical data and theoretical frameworks. Interview transcripts were coded using NVivo software.
Several steps enhanced research validity:
Multiple coders analysed initial interviews to establish a consistent interpretation. Findings were triangulated across different data sources. Results were situated within the existing literature on community economies and organizational change.
Key limitations included:
Single interview per organization limiting perspective. Restricted opportunities for direct observation due to COVID-19. Cross-sectional rather than longitudinal data collection.
Description of the Featured Cases
Health in Harmony: Regenerating Rainforests Through Healthcare
(HH is a non-profit organization collaborating with Indonesian partner Alam Sehat Lestari to operate health clinics in Indonesia, Brazil and Madagascar. Its primary goal is rainforest conservation, achieved by addressing the root causes of deforestation while providing accessible healthcare services (Webb, 2021).
HH employs ‘Radical Listening’ through village meetings to understand drivers of illegal logging. Sessions revealed that locals resort to logging for healthcare expenses, with limited alternatives available despite recognizing the negative environmental impacts.
To tackle these interconnected issues, HH established health clinics offering services at low prices or through non-monetary contributions. The cost of care is about one-third of the previous options (Interviewee 8). A distinctive aspect of HH’s model is that locals design the conditions for healthcare access, monitoring systems and programmes to help households transition from logging. Community members, knowledgeable about the local context, monitor reduced logging activities, a system developed through Radical Listening. Weekly open meetings foster community involvement, and HH employs and trains locals to ensure deep integration into the community. Notable innovations include the Chainsaw Buyback program, organic farming initiatives and the Goats for Widows programme (Webb, 2021).
HH’s commitment to the link between nature and health is reflected in its clinics’ design, which feature national park views and utilize locally sourced, eco-friendly materials. Local labourers, particularly former loggers, are employed for construction, providing them with income and new skills.
In Indonesia, HH’s collaboration with local communities has led to a 90% reduction in households reliant on logging for income and a 67% decrease in infant mortality among the 120,000 people served by its medical centre (Jones et al., 2020). As a women-led organization, HH has empowered local women, exemplified by a community health worker who became the first female village chief after saving many lives (Webb, 2021).
Despite its successes, HH faces challenges. Local tribal leaders can significantly influence the adoption of non-logging livelihoods, and HH has limited leverage when loggers resist transitioning away from forest exploitation. Additionally, financial dependence on donors poses a vulnerability. HH has effectively expanded its model from Indonesia to new implementations in Madagascar and Brazil.
Buurtzorg India: High-quality and Accessible Healthcare
The Buurtzorg model, established in the Netherlands in 2006, introduced a nurse-led approach to holistic care, transforming community healthcare. It achieved high client satisfaction, staff commitment and significant financial savings, generating approximately 40% savings for the Dutch healthcare system. The model empowers nurses to provide comprehensive care, reducing hours while enhancing care quality (Buurtzorg website, 2024).
Central to Buurtzorg is the principle of ‘humanity over bureaucracy’, implemented through two strategies. First, it emphasizes holistic, person-centred nursing that advocates for patient autonomy, continuity of care and community resource connections. Second, it organizes independent, self-managing teams of up to 12 nurses, supported by regional coaches and a small administrative back-office (Hegedüs et al., 2022).
In India, Buurtzorg adapted its model to address the cultural context where elderly care is typically familial. BI provides home healthcare services to anyone needing professional care, responding to the challenges of a private healthcare system that often leaves many without access. Healthcare costs can lead families into debt, compounded by a shortage of trained nurses (Interviewee BI).
BI collaborates with EduGreen to train primarily women as caregivers, offering affordable healthcare in rural areas. These caregivers learn essential non-invasive tasks, covering about 80% of nursing needs, including medicine management and personal support. BI forms teams of 12, typically comprising three market-hired nurses and nine EduGreen-trained caregivers, creating dual benefits of empowering rural women and enhancing healthcare access. BI helps to communicate and translate between physicians and the patient. Patients are treated at home at one-tenth of the cost of hospital-based treatment (Interviewee BI; Buurtzorg India, 2020).
The COVID-19 pandemic exposed vulnerabilities in the BI model, as many families lost income and struggled to afford healthcare. Although BI reduced prices, low purchasing power and a lack of widespread insurance in India continue to pose significant challenges to healthcare accessibility (Interviewee BI).
Health Center Cecosesola, Venezuela: Communitarian Healthcare
HCC represents a distinctive approach to healthcare provision through a communitarian-cooperative model. The centre operates as part of Cecosesola, a cooperative network established in 1967 in Barquisimeto, Venezuela. Over decades, Cecosesola has evolved into an extensive network encompassing 40 cooperatives that operate across diverse sectors, including agricultural and agro-industrial production, funeral services, savings and loans, mutual aid funds, food distribution and healthcare (Rath, 2022).
The network’s substantial scale is evident in its 1,300 worker-owners who organize weekly markets serving approximately 100,000 customers. These market activities generate funding for initiatives like HCC, which required an investment of several million USD. This funding approach exemplifies how community-based financial models can support the development of significant healthcare infrastructure without relying on profit-maximizing arrangements (Rath, 2022).
HCC currently operates six cooperative clinics in popular sectors of Barquisimeto alongside a Comprehensive Cooperative Health Center. The communitarian approach manifests through several key features (Rath, 2022):
A non-profit orientation that prioritizes person-to-person encounters Emphasis on patient co-responsibility in the healing process Replacement of ‘medical orders’ with reflective invitations for patients to become active participants in their health Integration of allopathic methods with complementary approaches, including acupuncture, hydrotherapy, music therapy, yoga and respectful natural childbirth Creation of community spaces characterized by respectful treatment, participation invitations, mutual listening and accessibility for people with low incomes
The physical environment at HCC reflects these values through building designs that emphasize harmony with nature, utilizing natural light and ventilation throughout rooms and hallways. The centre provides open spaces and occasions where individuals can receive care and participate in collective management if desired (Interviewee HCC).
HCC faces several significant obstacles. One internal challenge stems from the elitist self-conception of many doctors, who perceive themselves as superior based on their expertise, thereby resisting the dialogue-based approach. External challenges include the persistence of domination-based relationships in everyday life, including patriarchy, racism and hierarchical arrangements, which create ongoing difficulties both within Cecosesola and in its external relations. Additionally, a tax regulation introduced in 2018 pushed Cecosesola into significant financial insecurity, requiring responses through civil disobedience actions (Interviewee HCC).
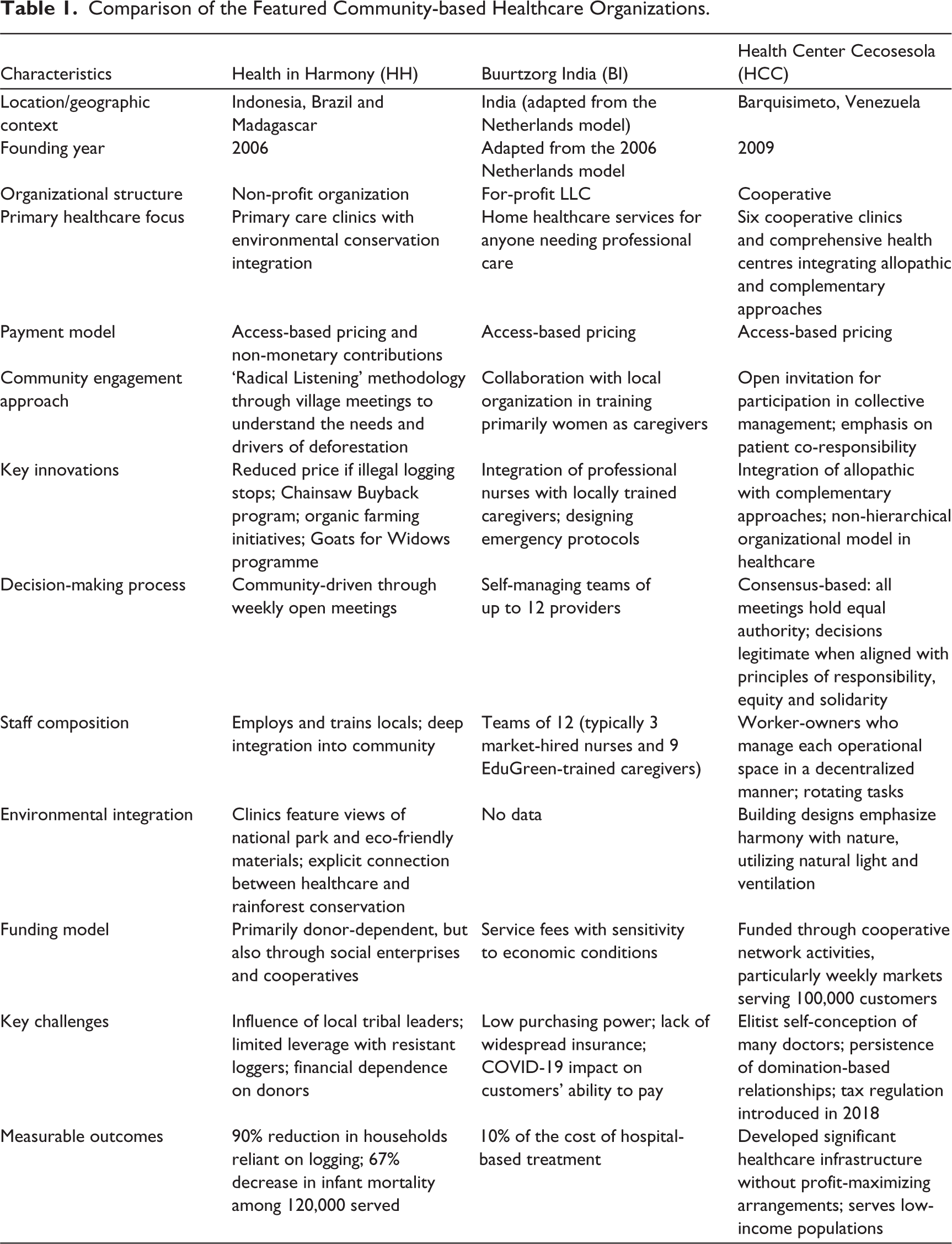
Table 1 summarizes the three community-based healthcare organizations’ key characteristics, highlighting their distinctive healthcare delivery approaches while revealing common patterns of ethical innovation.
Comparison of the Featured Community-based Healthcare Organizations.
Community-based Healthcare Model
Prioritizing Needs
The contrast between profit-maximizing healthcare systems and CBOs reveals fundamentally different approaches to healthcare delivery. While profit-maximizing systems prioritize financial returns, CBOs place the fulfilment of basic health needs at the centre of their operations, leading to more accessible and quality care.
Profit maximization in healthcare often raises costs without corresponding improvements in quality, pushing individuals into debt while benefiting select stakeholders (The Economist, 2023). The United States exemplifies this dynamic, spending $12,742 per person on healthcare in 2022—significantly higher than other wealthy nations, as the average for OECD countries (excluding the United States) was just $6,850. Despite this extraordinary spending, US health outcomes consistently lag behind other developed nations across life expectancy, infant mortality and maternal health (Peterson Foundation, 2024).
The opioid crisis further illustrates the dangers of profit-prioritization in healthcare. Companies like Purdue Pharma created networks among health workers, advocacy groups and policymakers to expand opioid use beyond cancer patients, downplay addiction risks and dismiss physician concerns. This strategy resulted in hundreds of thousands of deaths and trillions in societal costs (Marks, 2020).
In contrast, the CBOs studied demonstrate how prioritizing needs transforms healthcare delivery. At HH, this appears in their flexible payment systems, which allow for significant discounts through various non-monetary contributions. Patients can access healthcare services by contributing to forest regeneration through planting seedlings, providing manure, doing odd jobs around the clinic or contributing food. This system makes healthcare services accessible for those unable to pay, with costs approximately one-third of previously available options (Webb, 2021).
BI similarly demonstrates sensitivity to local economic conditions in its pricing models. While operating primarily through monetary transactions, they continuously monitor social and economic circumstances to ensure accessibility. When COVID hit, BI recognized this and adjusted the prices to allow those in need access to healthcare services (Interviewee BI).
Furthermore, BI developed its own IT system, which helps with the self-coordination and knowledge sharing of the caregiving teams. By relying on the knowledge and experience of a local NGO, EduGreen, BI is working on an emergency protocol (a highly unregulated space in India) by developing a curriculum for emergency medical technicians (Interviewee BI).
In HCC, during Venezuela’s 2019 economic crisis, when general power outages combined with hyperinflation, member-owners decided to continue providing health services without requiring immediate payment. After the crisis subsided, patients who had received care during this period paid for the services (Interviewee HCC). This illustrates how prioritizing healthcare access over immediate financial considerations creates resilient systems capable of serving communities even in extreme circumstances.
In each case, the organizations demonstrate a ‘mystique of wanting to serve’ (Interviewee HCC) that manifests in selecting locations in poorer areas, creating flexible payment systems and adapting to economic realities—all in service of ensuring healthcare reaches those who need it most, regardless of their ability to pay.
Organizational Openness and Participatory Governance
The healthcare CBOs studied exhibit a notable characteristic of organizational openness, allowing stakeholders to participate in decision-making processes actively. This openness helps organizations remain connected to local contexts and be capable of responding to local issues through fostering participation.
HCC exemplifies radical organizational openness, lacking traditional governing bodies, managerial roles or command chains. Worker-owners operate within integrated cooperatives, managing decentralized operational spaces without fixed positions and rotating tasks. Decision-making is inclusive, with policies affecting the organization—such as pricing and financing—determined by consensus. No hierarchy exists; all meetings hold equal authority and decisions are deemed legitimate when they align with principles of responsibility, equity and solidarity, regardless of their source (Interviewee HCC).
The HCC payment system differentiates between doctors and non-doctors, with medical practitioners earning based on activities performed, while other members receive a uniform fixed income (Interviewee HCC).
HH employs a ‘radical listening’ methodology to institutionalize organizational openness, creating formal avenues for community input in programme design and implementation. This approach revealed that healthcare costs contributed to illegal logging, prompting the development of solutions based on community-identified needs. Locals design the conditions for healthcare access, monitoring systems and programmes to help households transition from logging (Interviewee HH).
The locally created monitoring system exemplifies how organizational openness fosters contextually relevant solutions. ‘Forest Guardians’, local villagers familiar with their community’s realities, monitor compliance with illegal logging regulations to qualify for lower-cost healthcare services. This system effectively pressures logging villages to reduce illegal logging (Interviewee HH).
Autonomy-supportive Environments
The case organizations demonstrate how autonomy-supportive environments foster prosocial behaviour and enhance healthcare delivery. Self-determination theory suggests that autonomy encourages prosocial tendencies, while controlling environments can lead to antisocial actions (Donald et al., 2021). Beyond autonomy, two additional factors—relatedness and competence—promote prosocial behaviour. Relatedness emphasizes giving and receiving care, evident in the relationship-centred approaches of these organizations. Competence involves engaging in activities that create a sense of adequacy and positive impact (Weinstein & Ryan, 2010 cited in Donald et al., 2021).
These CBOs demonstrate a ‘crowding-in’ of ethical motivations and practices that extends beyond incentives and rewards. This phenomenon involves positive feedback mechanisms, including prioritizing needs, supporting autonomy, recognizing diverse values, maintaining organizational openness, encouraging self-monitoring and building trust. As Bowles (2016) notes, crowding-in connects moral messages to formal enforcement and peer pressure, creating environments where prosocial behaviour becomes self-reinforcing.
The autonomy observed in these cases aligns with Sen’s (2008) capabilities approach, highlighting the importance of meaningful actions for oneself and society. CBOs foster cultural contexts conducive to ethical social practices by providing spaces where one can contribute to the betterment of his or her personal well-being while contributing to the betterment of the community.
To foster self-reliance, community members identified three key needs: enhanced education for healthcare providers, fish-farming training and access to water filters (Webb, 2021). HH promotes autonomy for staff and the communities it serves. One initiative, the Chainsaw Buyback program, helps loggers transition to sustainable livelihoods by purchasing their chainsaws for around $200 and offering up to $450 in financial support for alternative ventures like shops, organic farming or beekeeping. This programme acts as an angel investor scheme without interest charges, allowing households to move away from destructive practices and gain economic freedom. Recently, the initiative has expanded to upcycle chainsaw parts into tools for organic farming, showcasing innovative environmental solutions (Health in Harmony, 2024).
In response to community needs, HH provides organic farming training, teaching locals to grow food with no or minimal chemicals and produce organic fertilizers. Local community members lead these sessions, emphasizing the importance of organic farming in regenerating previously neglected or over-exploited land. As a local cooperative leader noted, the ability to create organic fertilizers has allowed some members to profit enough to completely shift away from logging (Webb, 2021).
Another initiative, the Goats for Widows programme, supports disadvantaged women by providing them with a mated pair of goats. Each woman is expected to ‘pay forward’ one baby goat to another widow and contribute goat manure to local farmers. This generates a steady income that enables recipients to afford educational expenses for their children or grandchildren (Webb, 2021).
BI exemplifies high team autonomy, maintaining a low management overhead of 8% compared to the industry standard of 25%. The organization prioritizes patient well-being over profit, focusing on educating patients and families about self-care and facilitating communication with physicians. Home-based treatments cost significantly less than hospital care (Interviewee BI; Buurtzorg India, 2020).
HCC adopts an even more radical approach to worker autonomy, lacking fixed labour positions or traditional supervisory roles. Authority arises from contributions rather than formal titles, fostering a culture of conversation that guides self-organization (Interviewee HCC). Participants noted that this structure dilutes power over others, transforming it into the power to act. This environment encourages all individuals—regardless of their roles—to work as equals, promoting creativity, holistic well-being, solidarity and a sense of belonging (Interviewee HCC).
While this autonomy-centred and community-oriented design of HCC may slow response times, it allows for a healthcare approach adaptable to diverse needs and expectations. The organization actively engages politically, emphasizing dignity and community-oriented strategies (Rath, 2022).
Trust-building and Relationship Development
Healthcare CBOs prioritize trust and relationships as fundamental to effective healthcare delivery. They emphasize connections beyond clinical encounters, fostering dignity, reciprocity and mutual care. HCC exemplifies this by framing its approach as a ‘cooperative-community process’, aiming to build relationships based on responsibility and trust rather than exploitation and indifference.
HH adopts a similar relational model, establishing reciprocity agreements with the communities it serves. Leaders emphasize recognizing local villagers as equal partners, acknowledging their role as guardians of the rainforest and the potential for mutual benefit (Interviewee HH). This contrasts with traditional philanthropic models that can create dependency and negative feelings among recipients (Zamagni, 2022). Instead, CBOs promote arrangements that allow all stakeholders to contribute meaningfully, fostering a sense of agency and community involvement.
BI’s model further illustrates the importance of relationships through its holistic, person-centred care approach. It focuses on building trust within neighbourhoods and connecting patients to community resources, resulting in low staff turnover and abuse rates. Staff enjoy stable wages and respect from patients and families, enhancing the overall care environment. Trust extends to business relationships, as seen when BI streamlined a formal agreement with Buurtzorg Netherlands, emphasizing mutual trust over complex documentation (Interviewee BI).
Conclusions and Implications for Business Transformation
This study sought to answer two critical questions: How do healthcare CBOs prioritize accessibility and quality, and what organizational characteristics enable this approach? Through our examination of HH, BI and HCC, we have identified four key characteristics that enable these organizations to prioritize healthcare access and quality over profit maximization: (a) needs prioritization, (b) organizational openness and participatory governance, (c) creation of autonomy-supportive environments and (d) trust-building and relationship development. These interlinked and interdependent pillars form the foundation for a transformative approach to healthcare provisioning that offers valuable lessons for business transformation across sectors.
Healthcare CBOs prioritize accessibility and quality by orienting their core purpose toward meeting genuine health needs and avoiding profit maximization. The case organizations accomplish this through innovative approaches to pricing and payment (e.g., flexible payment systems, non-monetary contributions and price adjustments during livelihood crises) and integrative approaches to treatment and infrastructure development. These approaches result in significantly lower costs for patients while maintaining or enhancing the locally accessible quality of care.
The second essential step involves restructuring governance to incorporate genuine stakeholder participation. Healthcare organizations should establish formal channels for patient and community input. This participatory approach supports services to remain aligned with community needs while fostering accountability and transparency.
Third, organizations must create autonomy-supportive work environments that empower healthcare providers to exercise professional judgment and creativity. Buurtzorg’s self-managing team model demonstrates how reducing profit-maximizing bureaucratic control can improve care quality and provider and patient satisfaction. Organizations should remove the bureaucratic or market obstacles that hinder healthcare professionals from providing the best available care to those in need.
The fourth pillar—building trust-based relationships—requires a fundamental shift in how healthcare organizations interact with patients, communities and their own staff. Organizations should implement relationship-centred care models that prioritize continuity and personal connection. They should also establish fair labour practices and create mechanisms for staff to contribute to organizational decisions, fostering internal trust that extends to external relationships. Healthcare professionals should have the time and capabilities to support patients in becoming engaged with their healing process.
Frey and Osterloh (2004) posit that organizations face fundamental social dilemmas arising from intensive interdependencies among self-interested individuals. These dilemmas manifest as three key problems: the tendency to free-ride, the exploitation of information asymmetries and underinvestment in firm-specific resources. These social dilemmas are at the heart of firms’ activities, occurring when ‘the actions of self-interested individuals do not lead to socially desirable common pools’ (Frey & Osterloh, 2004, p. 100). To overcome these challenges, they propose a framework that emphasizes fiduciary roles throughout the organization, investment in firm-specific knowledge and—most critically—the cultivation of prosocial intrinsic motivation fostered by appropriate governance structures.
The evolutionary framework outlined by Wilson et al. (2013) and derived from Ostrom’s (1990) work identifies several critical design principles that help protect against exploitation, free-riding and other social dilemmas that commonly undermine collective action. These principles are evident in our case organizations: clearly defined boundaries of the cooperative group, proportionality between costs and benefits, stakeholder participation in rulemaking, low-cost methods for conflict resolution and polycentric governance with distributed authority.
The case studies demonstrate that maintaining these arrangements require deliberate organizing practices where self-organization, self-enforcement, monitoring, participatory rule-making and gradual conflict resolution are central features. The cases show that protecting the core mission of CBOs—prioritizing basic needs and maintaining openness to stakeholder voice and participation—requires intentional institutional design and ongoing nurturing.
CBOs represent viable patterns for business transformation across various sectors. For instance, the Mietshäuser Syndikat model in housing allows residents to collectively own and manage living spaces, ensuring affordability and community control. In the energy sector, EWS Schönau illustrates how community-owned cooperatives can transition to renewable energy while maintaining democratic governance. The Mobility Factory addresses mobility needs through community e-car sharing systems, promoting resource efficiency and accessibility. In finance, cooperative banking models like ZEF prioritize community needs over profit maximization.
Business organizations aiming to operate socially responsibly should be engaged in trust-building, relationship development and autonomy-supportive environments that nurture prosocial motivations rather than reinforcing self-interested behaviour. Most importantly, they should have the core mission of prioritizing basic needs and supporting them with deliberate organizational design, with specific attention to governance processes that promote cooperation and limit opportunities for exploitation.
Footnotes
Acknowledgements
I thank the interviewees for their time and energy in answering my questions.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Informed Consent
This research was conducted in accordance with ethical standards for studies involving human participants. All interviewees were fully informed about the aim of the research and provided their consent to record the interviews and use the data for research purposes. Institutional ethical approval was not required.
Funding
The author received no financial support for the research, authorship and/or publication of this article.