
Abstract
This comparative research looked at the causes of the variance in provincial response to COVID-19 in Pakistan using the policy capacity framework. Pakistan decentralised its policymaking in 2010 and granted autonomy to its provinces to mitigate the crisis, control law and order, generate resources and reform their institutions. There were serious concerns that the small provinces lacking the required policy competencies will not be able to deal with a crisis such as COVID-19. Using process tracing and inductive mixed methods, this research finds that the relationship with the centre, effective networking with international agencies, non-state actors and China-Pakistan Economic Corridor (CPEC) are the key factors that improved the policy competency of the small provinces, whereas the weak steering ability of the state machinery, complacent and negligent behaviour of the political and administrative institutions and tension with the centre adversely impacted the analytical, operational and political competencies of the two large provinces of Punjab and Sindh, resulting in the spread of COVID-19 cases in these provinces.
Keywords
Introduction
Policy capacity is defined as the state and actor’s ability to govern, coordinate and implement policy choices (Bullock et al., 2001; Fukuyama, 2013; Painter & Pierre, 2005). It is considered a necessary pre-condition for governance success especially in times of crisis. Davis (2000) defined it as the ability of the government to efficiently implement preferred choices of action as well as decide upon them and linked it to successful implementation of the policies. In the case of COVID-19, the conceptual uncertainties surrounding the crisis initially made it very difficult to accurately determine the state’s policy capacity. Past experience, pre-existing ideological perspectives and beliefs of the government’s key administrative and law enforcing institutions primarily defined any state’s initial response to the pandemic. Asian experience and strict implementation of policies like the exhorting lockdowns, quarantine, physical (or social) distancing, proactive testing and tracing measures managed to satisfactorily offset the economic and social impact of the pandemic. Successful implementation of these policies, therefore, became the critical determinant to evaluate and compare a state’s policy capacity (Rosella et al., 2013; You, 2020).
In Pakistan, the first confirmed case of COVID-19 was reported as early as 29 February 2020. In a televised news conference, the special assistant to the Prime Minister on health, Zafar Mirza, formally announced that the infected person entered the country undetected at the Taftan border in the province of Baluchistan, after returning from a religious pilgrimage from Qom, Iran. He went to his home in the southern province of Sindh and reported in a local hospital in Karachi when the symptoms appeared. The first fatality due to COVID-19 in Pakistan, however, was reported on 18 March 2020, in the northern province of Khyber-Pakhtunkhwa (KP). Preliminary research looking at the individual province’s response to novel COVID-19 looked at the province-wise distribution of the first 100 cases and fatalities with the National Emergency Operation Centre (NEOC), and National Institute of Health (NIH), Islamabad collected by the COVID-19 surveillance and rapid response teams. The data showed that initially the highest number of cases (approximately 44%) were reported in the province of Khyber-Pakhtunkhwa (KP), Sindh stood second with 22% of the cases, and Gilgit-Baltistan (GB) third with 12% of the cases. Whereas cases recorded in Punjab, Baluchistan and Federal Capital Territory were 9%, 8% and 5% respectively. Now (as of 5 October 2020) the Government of Pakistan’s (GoP) national scoreboard shows a very different picture. The national score board show a total of 356,351 confirmed COVID-19 cases (6,517 fatalities) in Pakistan. The province of Sindh stands at the top with 43.88% of confirmed cases (38.68% total fatalities), and Punjab follows with 31.7% of confirmed cases (34.37% total fatalities). KP, which was at the top initially, has dropped to the third position with 12.08% confirmed cases (19.36% total fatalities), followed by the federally administered territory with 5.33% cases (2.80% total fatalities), Baluchistan with 4.88% cases (2.24% total fatalities), GB, which initially stood third, has dropped to the last with only 1.22% recorded cases (1.36% total fatalities; see Figure 1).
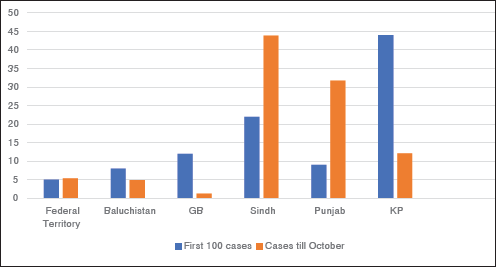
Figure 1 shows a significant difference in the initial and final provincial response to COVID-19. This variance is significant because, in April 2010, Pakistan implemented the 18th Constitutional Amendment. The constitutional amendment granted full autonomy to the constituent provinces to make their own policies, control their law and order agencies and when required to generate their own resources (The Gazette of Pakistan, 2010). Thus, this observed variance in the provincial response to COVID-19 provides a good opportunity to study the policy capacity of Pakistan’s individual provinces. The abrupt implementation of 18th Constitutional amendment in 2010 had raised serious concerns over the unequal policy capacity of the provinces (Burki & Ziring, 2019). It was argued that the provinces of KP, GB and Baluchistan, unlike the provinces of Punjab and Sindh, lacked the required resources and capacity to deal with a crisis like that of novel COVID-19. This was because historically Pakistan has used the population scale for the distribution of resources to its provinces. Due to the population advantage the provinces of Punjab and Sindh had always bagged more resources. More resources and population in turn had allowed for better training and experience for their administrative and law and order institutions. The provincial standing in the COVID-19 national scoreboard, however, with time negated these concerns. Notwithstanding higher percentages of the initial cases the provinces of KP, GB and Baluchistan fared much better in controlling the spread of the pandemic. This paradoxical behaviour sets the premise for this comparative study. This research will use the policy capacity framework to evaluate and compare the causes of variance in the policy capacity of Pakistan’s five provinces’ namely, Punjab, Sindh, Baluchistan, KP and GB, towards controlling the COVID-19 pandemic. The research also aims to understand why the provinces which were hitherto considered weaker had performed better, during the crisis, than the provinces with more resources and stronger policy capacity. Since the implementation of the 18th constitutional amendment, a gap exists in the comparative study of the provincial capacities. Thus, this study will also contribute towards filling this gap and can be used as an important benchmark for future comparative analysis of Pakistan’s provincial government’s policy capacity.
Policy and governance-based scholarship on the COVID-19 crisis is still evolving. Scholars from geographical east and west have analysed the state’s policy capacity during the pandemic vis-a-vis institutional, organisational and network arrangements and capacities (Capano et al., 2020; Nicholls, 2020; Rozell & Wilcox, 2020; You, 2020). In this slim scholarship, a gap exists in analysing the policy capacity of the South Asian states vis-à-vis COVID-19. The South Asian scholarship on governance highlights the political hostility between the ruling party and the opposition political parties as the key factor contributing towards local government crisis in Bangladesh (Fariduddin, 2017). Kumar and Rani (2019) studied the variance in the social development index (SDI) and human development index between 28 states and 7 union territories (UTs) of India. The study only ranked the states according to the disparities in SDI and did not elaborate on the factors contributing towards these disparities. This comparative research focusing on the South Asian state of Pakistan will be contributing towards these broader scholarships.
Theoretical Framework
Policy capacity has both skills and resources components. Polidano (1999) stresses a skill-based definition of policy capacity that looks for the necessary skills to structure the decision-making process, coordinate it throughout the government, feed informed analysis into it and ensure that the analysis is taken seriously. Pierre and Painter (2004) highlight resources as a key determinant of policy capacity; ‘the ability to marshal the necessary resources to make intelligent collective choices’, and ‘to set strategic directions for the allocation of scarce resources to public ends’ (p. 45). Parsons (2004) emphasised the systematic and strategic use of knowledge, collected via both instrumental and non-instrumental approaches to building a coherent, holistic, networked and integrated policy capacity. Political support, both from above and below, is another key factor for sustaining policy capacity. Even promising policies from the federal perspective get under-delivered due to capacity issues and resistance (Howlett, 1999). The agencies and managers must be considered legitimate by policy subjects and get continued support from their authorising institutions and constituencies (Pierre & Painter, 2004). The popularity of the regime and its relations with its societal actors also contribute towards building policy capacity (Richardson, 1982).
In the decentralised and de-regulated regimes, the collaborative and network-oriented patterns of governance and the ‘New Public Management’ (NPM) model, allowing those working on behalf of the government to manage or steer, had also directly impacted the determinants of state’s policy capacity (Giddens, 1996; Hajer & Wagenaar, 2003; Hood, 1991; Osborne & Brown, 2005; Osborne & Gaebler, 1992). Such a transformation had considerably altered the traditional hierarchal approach to service delivery and introduced new forms of accountability and transparency of the state agencies (Howlett & Tosun, 2018; Knill, 1999; Painter & Pierre, 2005; Richardson, 1982). The multiplicity of actors and complex decision-making processes makes it difficult to determine who is in-charge, has weakened the accountability mechanism available to the state and taking necessary actions to achieve the policy goals has also became difficult (Keast et al., 2006). Fukuyama (2013) offers solution by granting greater autonomy to the government servants. Thus, in addition to the decision-making styles, and the administrative structures of the regime and of the individual provincial governments, autonomy available to the institutional decision makers, the patterns of interactions between the regimes and the lead government agencies at the federal and provincial levels and with the stakeholders also became the critical determinants of the policy outcome (Howlett & Ramesh, 2014; Panitch, 1977; Whitaker et al., 2012). Overall, while looking at the decentralised regimes, multiple factors like the state’s steering ability, the effectiveness of the regulatory agencies, state of social trust, rule of law, liaison with societal leadership, ability to frame options, effective use of communications and stakeholder management strategies, determining exact resources for building new associational structures, and additional skills for building a more coherent, holistic, networked and integrated policy capacity, must be taken into consideration (Howlett, 2002; Howlett & Ramesh, 2014; Parsons, 2004).
A comprehensive framework to evaluate policy capacity from these multiple and diverse variables was provided by Wu et al. (2017). The framework separately appraises three areas of policy competencies: analytical, operational and political. The analytical competency determines if the policy actions are technically sound and can play an instrumental role in the attainment of policy outcomes. Operation competency connotes that the available resources are aligned with the policy action to ensure successful implementation of the policy. Political competency determines if the implementing authorities enjoy the support necessary for sustaining the actions deemed critical for the achieving the optimal policy outcome (Wu et al., 2017, p. 5). For a particular policy action to succeed any one competency may acquire a critical value over another (Wu et al., 2017, p. 5). Similarly, one competency may become the principal vulnerability, impediment or ‘Achilles’ heel’ significantly impeding the optimal policy outcome (Howlett & Ramesh, 2016).
Methodology
This research has used process tracing and mix methods. Process tracing is strongly recommended for governance and policy intervention analysis when an explicit theoretical analytical framework is available, as it helps in increasing the inferential in complex within-case evaluation studies (Schmitt & Beach, 2015). Process tracing also allows for multiplicity of methods further helps in determining causality. Mix methods not only help to unfold the depth and breadth of complex real-world policy issues but also allow for triangulation and critically judging the evidence (Brannan, 2007; Bryman, 2006; Mahoney, 2012). Data were collected from GoP official websites like the national scoreboard which shared the surveillance data collected by NIH. Semi-structured interviews with provincial government officials, media representatives, businessmen and informed members of the public were conducted via telephone, email or messenger. Newspaper reports, published interviews, speeches and tweets of key government figures related to COVID-19 were also used. Other methods like public documents, archived research reports of credible international organisations like, CPEC, Agha Khan Foundation, etc. were also utilised for further validation and triangulation.
The next section on the historical background was structured following Mahoney’s (2015) advice on avoiding endless regression . The section, therefore, focuses on Pakistan’s transformation to deregulatory regime post 1971 only. The section is followed by sharing the research data and study of the three competencies linked to the policy capacity of the Federal Government, and the five provinces, namely Baluchistan, GB, KP, Sindh and Punjab. The last section provides a discussion and conclusion.
Brief History of Pakistan’s Deregulatory and Regulatory Regimes
Pakistan’s covert transformation to the free-market economy began in the 1980s during Zia-ul Haq’s regime (Baxter, 1985). The threat of weakening of the state that accompanies such a transformation was eliminated during this time by the strong presence of the elite cadre of Pakistan bureaucracy, headed by President Ghulam Ishaq Khan, who prepared the blueprint of the state transformation (Siddiqi, 2020). This privilege was, however, taken from their hands during Pakistan’s democratic transition of the 1990s. Not only the industrialist Nawaz Sharif had no interest in continuing with the nationalised economy, but Benazir Bhutto also decided to bid farewell to her father’s ideology and embraced the free market economy. The transition was not without conflict and the 1990s was marked by the desperate struggle between the state bureaucracy to maintain its hegemony over state transformation and the political supporters of the free market paradigm (Ahsan, 2012; Wilder, 2010). This imparted the continuous conflict also impermanence to Pakistan’s democratic transitions of the 1990s and raised threats of a failed state for the country.
In the first decade of 2000, the weakened state was considerably revived by the Musharraf regime’s policies, which introduced the regulatory bodies to ensure that it is the state and not the free market that remains on the steering seat (Cohen, 2002; Siddiqi, 2020). The end of the Musharraf regime and the renewal of the democratic process once again brought back the free market beneficiaries but the pressure of good governance from international agencies like the World Bank, Asian Development Bank (ADB) and International Monetary Fund (IMF) kept the bureaucracy and the regulatory setup functional (Husain, 2015). The good governance project also called for some kind of categorisation or prioritisation of the citizen groups threatening the previously established power structures. In these transforming times the asymmetry of Pakistan Federation, and the quota system for political representation and resource distribution which adopted provincial population as a scale led to the dominance of the Punjabis in the legislative and administrative institutions (Jalal, 1995; Babakail, 2016; Siddiqi, 2020). The interprovincial dissension led to the 18th constitutional amendment of 2010 which gave each province the autonomy to forward its own development programme, generate its own resources and create its own rule of law philosophy. The political uncertainty inherited in the democratic processes pushed those in power to design ways to push forward their own agenda for the redistribution of provincial resources and control the authorities that steered the process. Bargaining between the political players of both the political and administrative groups in each province came about (Abbas, 2019; Burki & Ziring, 2019; Siddiqi, 2020). New provincial laws, like the police laws, restructuring of the administrative districts, new mechanisms of rewards and punishments were devised to limit and control the discretion of the power groups. Key informants contacted for this research stated that the 30-year reign of the Pakistan Muslim League in Punjab and Pakistan People’s Party in Sindh was not without successful bargaining between the political and administrative actors in these two provinces. However, it is not empirically determined if these arrangements also improved the policy capacity or the individual analytical, operational and political competencies of these provincial governments.
Policy Capacity of the Federal Government vis-a-vis COVID-19
The first indicator of Federal government’s analytical competency was the ‘National Action Plan for Preparedness and Response to Corona Virus Disease (COVID-19) Pakistan’, which was presented by the Ministry of National Health, Services, Regulation and Coordination on 12th February 2020. The salient features of the ‘National Action Plan’ (NAP) included response to the outbreak in a timely and efficient manner, to prioritise financial resources and increase domestic and international investment in dealing with the emergency, and to ‘strengthen inter-sectoral collaboration’ between government sector, private sector and civil society for the successful implementation of the emergency action plan. Following this, the GoP also established a ‘National Command and Control Centre’ (NCOC) to ensure effective coordination between federal and provincial governments. The national coordination committee was chaired by the prime minister and included relevant federal ministers, chief ministers and health departments of all the provinces. The National Disaster Management Authority (NDMA) was mandated as the leading operational agency for the COVID-19 pandemic surveillance and control through rapid response. Government ministries/departments/organisations, armed forces, INGOs, NGOs and UN agencies were to work through the NDMA to conduct one window operations (NDMA, 2020). NDMA operated through three levels: the national level, the provincial level (PDMA) and the district level (DDMA) aiming to transfer the analytical and operational competencies of the federal government to the provinces. DDMA included members of district administration, police and members of local bodies. NDMA was also in direct contact with World Health Organisation (WHO) which positively impacted its analytical competency. All these measures indicated satisfactory analytical competence of the federal government. This research, however, finds that DDMA was the weakest link in the operations, as a result of which correct implementation of the national action plan for the control of COVID-19 at the district level could not be ensured.
The availability of adequate resources was the main handicap faced by the federal government initially. At the federal level, in addition to NDMA, the Ministry of Foreign Affairs also coordinated for international assistance and resources for controlling the COVID-19 pandemic. Initially, NDMA worked with 1.8 million masks, kits for testing 210,000 people, 36,000 pieces of protective clothing, essential medical equipment such as ventilators and forehead thermometers and personal protective equipment worth PKR 67 million, mostly acquired from China. In the federal capital territory, NDMA marked 19 public and private COVID-19 testing facilities. The Pakistan Institute of Medical Sciences (PIMS) was designated as the tertiary hospital for COVID-19 treatment, and an isolation ward of 10 beds was also set up in the hospital. In addition to this, a quarantine facility of 300 beds was created in the Hajj Complex, and 50 beds in Pak China Friendship Centre, Islamabad. Hotels and hostels were also marked if the cases increased beyond the capacity of the dedicated hospitals. Special websites and telephone helplines in seven local languages were also established to guide the citizens with the SOPs and for contact tracing (Waris et al., 2020). In April 2020 NDMA acquired a loan from Asian Bank to purchase additional resources including 2,000 testing kits, 50 mobile X-rays machines, 1 million KN-95 masks, 5 million medical masks, 10,000 surgical gowns, ICU ventilators and other goods (CPEC Info, 2020a). The additional resources helped the federal government not only to appropriately frame its response to the pandemic at the institutional level, but also gave it an uncommon latitude and capacity in terms of other policy choices. It announced a relief package of PKR 900 billion (US$5.66 billion) to combat the adverse effect of the lockdown. The relief package included PKR 200 billion (US$1.25 billion) for low-income groups, particularly labourers, PKR 280 billion (US$1.76 billion) for wheat procurement, apart from a significant reduction in petroleum prices.
These policies, in turn, helped improve the political competence of the federal government and played an instrumental role in improving public response to the crisis. Citizen response to the government directives and the law-enforcing institutions in the federal capital territory during the lockdown was observed. All the public places and roads were found empty during the lockdown. The public peacefully observed the lockdown, showed no retaliation to the government directives and followed the SOPs. Islamabad Capital Territory (ICT) police and Rangers patrolled the territory. Random officials patrolling the areas were questioned and they also noted that the public response was good and citizens posed no opposition to the government directives. Overall, the public responded well to the tracking, lockdowns and isolation policies which, in turn, helped achieve policy objectives. The success of the complete lockdown in the federal capital territory also indicate good political competence of the federal government. However, this was not the case in all the provinces, as will be discussed below.
The federal government kept revising its policies also. With the spread of the pandemic, the initial policy of screening travellers coming from the infected countries was revised to include travellers coming from all countries. Arrangements for COVID-19 screening were made at all points of entry including airports, land crossing and sea. More resources were mobilised to screen, isolate and track these cases. From 23 January 2020 to 20 March 2020, an estimated 1,102,562 passengers were screened (NDMA, 2020; OCHA, 2020). Similarly, initially (from 15 March to 31 May 2020) the federal government announced a countrywide complete lockdown. In this, all public gatherings, festivals and get-togethers were cancelled. Hotels and halls were banned from hosting any such events. No vehicle with more than two passengers was allowed on the roads and people were advised to come out only for very important chores. As the lockdown progressed, concerns about its adverse impact on a developing country’s economy dominated the government. ‘Complaints from business community and public was taken in due consideration’. 1 NCOC decided to eject the complete lockdown in favour of ‘smart lockdown’ which included quarantine only to those residential sectors/suburbs and ‘streets within the suburbs where a surge in the COVID-19 cases was reported. Revision of policies to make them sustainable also indicate a strong analytical competence of the federal government. Assistant Commissioner, Islamabad city, informed that to achieve optimal policy outcome special arrangements like the on-line ordering of essential daily provisions and medicines for the residents of the quarantined areas were also made by the Islamabad City Administration.
Provincial Policy Capacity vis-a-vis COVID-19
Baluchistan
Baluchistan is the largest province of Pakistan, constituting 44% of the country’s total land, but it is the least populated. Only a part of the province is under the administrative control of the state and the rest is a tribal area. According to the 2017 census, Baluchistan is divided into 32 districts (PBS, 2020). Since 1947, due to insurgencies and terrorist activities, the province had remained under the centre’s strong control. This arrangement especially made it easy for NDMA and PDMA to effectively implement their action plan in the province. Three factors directly threatened the spread of COVID-19 in Baluchistan: the Pak–Iran border, Afghan refugee villages and mega-scale CPEC project.
In February 2020, the first confirmed case of COVID-19 reported in Sindh had also entered Pakistan via Taftan border post in Baluchistan in February 2020. The provincial government’s initial response included imposing extra health checks on the borders. The infected travellers returning from Iran and entering Baluchistan were asked to self-quarantine for 2 weeks in their homes. Later, the provincial government also closed the Taftan border for 2 weeks (NEWS, 2020). The PDMA data showed limited availability of dedicated resources in the province. Ten tertiary care hospitals in five districts of the province were designated for COVID-19 cases, with 4 hospitals in Gwadar (GoP, 2020, p. 1). 14 hospitals with isolation wards facility were set in 11 districts (GoP, 2020, p. 1) and quarantine facilities in 8 districts with a total of 5,897 beds only (GoP, 2020, p. 1). Furthermore, this research finds there were only five testing facilities for the province; two in the provincial capital Quetta, one at the CPEC hub in Gwadar, one in Khuzdar and one mobile diagnostic unit at Taftan border (GoP, 2020, p. 3).
The provincial government managed to increase its operational competency considerably by collaborating with CPEC and international organisations like the United Nations High Commission for Refugees (UNHCR). CPEC flagship projects operating at Gwadar and Baluchistan helped the Baluchistan government to bring in CPEC stakeholders like the China Overseas Ports Holding Company (COPHC), the company that runs Gwadar port, and others. These companies also invested resources and experts to cope with the province fragile health sector’s capacity and in creating awareness among the members of the CPEC project teams located at various locations in Baluchistan (CPEC Info, 2020b). ‘The awareness trickled down to the public of these localities, which also contributed in controlling the spread of the pandemic in the rural parts of the province’. 2 UNHCR was the other key actor that augmented the policy capacity of Baluchistan. According to the UNHCR, 82% of the total Afghan Refugees in Pakistan reside in KP and Baluchistan only. According to data on 31 August 2020, about 325,905 Afghan refugees resided in Baluchistan. With the support of UNHCR, a communication task force was developed in Baluchistan. Information, Education and Communication material in the local languages of Dari and Pushto was developed, which was distributed in all refugee villages to control the spread of COVID-19 (OCHA, 2020). The state, CPEC and UNHCR working in sync contributed towards building the political competence of the provincial government. The administrative and police institutions of Baluchistan faced no problem in implementing the policy choices, which markedly controlled the spread of the disease in the province.
Gilgit-Baltistan
The province of GB was formed in 2009 under the Gilgit-Baltistan Empowerment and Self Governance Order (GBESGO). GB’s provincial assembly was constituted in 2018 and all powers for legislation in GB were transferred to it (Khan, 2020). However, it lacked a proper democratic process and the people of GB had appealed in the Supreme Court for the enaction of Election Act of 2017 before the end of the term of the GB provincial government, due in June 2020. The promulgation of the Act was already delayed at the parliament and further delayed due to the COVID-19 pandemic. Thus, at the time of the COVID-19 crisis, GB was under the centre’s control which gave NDMA greater latitude to convene federal policy choices vis-a-vis the COVID-19 crisis in GB easily. This research finds that there was also a problem with the availability of administrative machinery in GB districts. This was because GB initially had 10 districts later, in June 2019, four new districts were carved out, bringing the total to 14. This addition, however, was for the political purpose only and no new administrative, revenue and police divisions were added in these districts (Abbas, 2019). As a result, the newly formed province lacked both the capacity and experience to deal with the crisis.
This research finds resources dedicated in the province were also insufficient. It included four designated tertiary hospitals (GoP, 2020, p. 1), 21 hospitals with dedicated isolation wards and 126 beds only (GoP, 2020, p. 5) and three COVID-19 testing facilities (GoP, 2020, p. 3). However, the number of quarantine centres was increased to 972, by marking a number of guests houses and hotels for the purpose (GoP, 2020, p. 4). The first case of COVID-19 was reported on 3 March 2020 in GB. Key informant, information secretary GB, said the person had also returned from Iran after a religious pilgrimage.
Initially, 12% of the total COVID-19 cases in Pakistan were reported in GB but by October this number dropped to 1.22%. In October 2020 the national scoreboard showed 4,000 confirmed cases in GB, with 3,702 recoveries and only 90 deaths (GoP, 2020). This research finds that, in addition to the freedom enjoyed by NDMAs to implement the policy choices of the centre networking with international organisations like the Agha Khan Foundation and with China, it greatly enhanced the operational competency of GB.
Agha Khan Foundation and Agha Khan Health Services (AKHS), a company corporate by guarantee, networked with Global Affairs Canada, European Civil Protection and Humanitarian Aid (ECHO) to establish six rapid response centres for COVID-19 in ‘remote areas’ of Gilgit, Mastuj, Alibad, Singal, Gramchamsa and Booni (AKHS & AKAH, 2020). Together these centres provided 150 beds and medical services to treat COVID-19 patients in far-off districts without existing administrative setups (AGHS, 2020).
The other factor that significantly improved the resources and operational competency of GB was its close business ties with China. All cargos coming from China pass the Khunjerab Pass to reach the first dry port- customs port located at Sust, GB. Under the 1985 border protocol, this border remains closed during the winter from November to April and opens in May each year and remains open till the end of November. As the number of COVID-19 cases started increasing in GB, the provincial government requested the federal government to delay the opening of Khunjerab Pass. The key informant informed that the GB’s importers and exporters association appealed directly to the Prime Minister to keep the borders open. There was also pressure from China. ‘The unity of intent to keep the trade route open led weight to the appeal’. Considering the serious economic implication for a developing country like Pakistan and on CPEC projects, the prime minister announced to open the Khunjerab pass, from 29 July 2020 till 10 August 2020 to facilitate the flow of goods only (Dawn, 2020). The situation also resulted in an increased level of co-operation from the Government of China. On 27 March 2020, the Chinese Embassy in Pakistan announced that China would hand over two tons of masks, test kits, ventilators, medical protective clothing worth 67 million rupees at Khunjerab, augmenting GB’s resources to control the spread of disease.
Khyber Pakhtunkhwa
The northern province of KP is the third province that managed to control the spread of disease due to its close ties and follow up with the central government at Islamabad and strategic use of its resources. Like GB, the operational competencies of the KP administration were also adversely impacted by the addition of a number of districts without any corresponding addition in administrative and law enforcing agencies. Archived research shows that during the democratic transition of the 1990s, many districts were added to increase the political influence of powerful families. Sixteen of the 34 districts in KP were formed after the 1980s, without any proper synchronisation of resources or administrative apparatus (Babakhel, 2018). After the 25th Amendment, FATA’s seven agencies were also incorporated in five administrative divisions of KP, and eight districts were added in the Malakand division but all this without assessing any potential revenue, rescue response infrastructure or even a police department (Babakhel, 2016). The absence of properly functioning district administration was expected to adversely impact the operational competence of the KP provincial government to control COVID-19.
At NIH the first infected person in KP was documented as a pilgrim who had returned from Mecca, Saudi Arabia, after performing Umrah. Although he contracted the virus and fell ill while in Saudi Arabia, he did not disclose his illness in Saudi Arabia or at the time of arrival in Pakistan. He returned to his village in Mardan, KP, where he was greeted by a large number of family, friends and villagers (approximately 3,000 people). When the symptoms exacerbated, he was taken to a hospital in Nowshera, but he refused to be quarantined in the hospital. The informants believed that this case alone directly contributed to the outbreak of COVID-19 in the major cities of KP. By 16 March 2020, the health minister KP tweeted that 15 confirmed cases of COVID-19 were reported in the province. The first patient in KP died on 18 March 2020. On 29 March 2020, KP provincial government complied with the centre’s directives and closed all the public and private educational institutions until 31 May 2020. By April 2020, on the national score board, most fatalities (16) due to COVID-19 in Pakistan were reported in KP.
The analytical and operational competency of KP government can be gauged through its response to the first case. Understanding the critical value of the first case and its implication the KP government responded promptly and closed Outdoor Patient Departments (OPDs) in all tertiary hospitals, district headquarters hospitals and private clinics for 2 weeks throughout the province. Initially, only international passengers returning from the affected countries were screened. The Chief operating officer of Bacha Khan International Airport informed that after the first case and the realisation that a large number of international travellers were coming to KP through domestic flights, a team of 70 doctors, paramedics and nursing staff was deployed at the Bacha Khan Airport Peshawar, on 16 March 2020 to scan and quarantine all passengers coming from all international and domestic flights. KP government’s timely collaboration with the centre also helped the provincial government to release a relief package of Rs.100 million to deal with the COVID-19 crisis. On 26 March 2020, the KP government recruited 1,300 doctors on contractual basis across the province to help stem the spread of the cases. Secondary sources also confirmed that to increase its operational capacity the ‘Public Service Commission KP’ also approved the recruitment of 635 more doctors in the province health force (Shinwari, 2020). Medical teams were also dispatched for the Pak-Afghan border at Torkham and Bajur. Isolation wards for COVID-19 cases were also prepared in several hospitals at Torkam, Landikotal and Jamrud. Arrangements for testing for COVID-19 in all the districts and tehsils of the province were made. Most significant was the strategic use of the ‘Polio vaccination teams’. The chief secretary of KP, responsible for the operation, informed that the polio vaccination teams are well trained and reliable surveillance teams and have footprints throughout Pakistan. Due to the COVID-19 pandemic, the polio vaccination campaign had to be suspended temporarily, but these trained health workers became a valuable asset; to track down the COVID-19 cases, to spread awareness of safety protocols and for contact tracing, especially in rural areas.
A critical review of the NDMA data shows the concentration of resources in the major urban centres of KP. That is, out of 34 districts of KP, only 7 tertiary hospitals were dedicated for COVID-19, of which 4 were in the provincial capital, Peshawar only (GoP, 2020). Eighteen testing facilities were established in KP of which 8 were in the provincial capital Peshawar. One hundred and ten isolation wards with a total of 856 beds were set in almost all the districts (GoP, 2020, p. 1). Fifty-two quarantine facilities with 2,760 beds were set up mostly in densely populated cities like Peshawar, Nowshera, Dera Ismail Khan and in bordering posts of Torkham, Landikotal and Jamrud (GoP, 2020, p. 2). After permission by NCOC and to overcome the adverse economic effects of lockdown, the provincial government adopted the smart lockdowns strategy and used mobile rapid response teams in what they called the ‘hot spots’ for testing and contact tracing. Smart lockdowns were implemented in 9 cities including 8 ‘hot spots’ in Peshawar, 6 in Abbottabad, 11 in Swat, 5 in Mardan, 15 in Nowshera, 3 in Khyber, 7 in Battagram and 3 in Chitral and Malakand. In these cities public gatherings were banned, wedding halls, barbershops and markets were closed. Food and pharmacies were allowed to remain open, whereas restaurants were encouraged to offer ‘take-away’ food only. Another informant, Mr Shaukat Afridi, vice president of a private bank in Peshawar, informed that private organisations slashed office timings and employees above 50 were sent on paid leave. However, this information could not be cross-checked. KP police also played an important role in the surveillance and ensuring successful lockdown and adherence to SOP in urban centres and disease hot spots. Fines were collected from the violators of lockdown norms. According to the Deputy Commissioner (DC) Peshawar, the police watch helped to fine 400 to 500 violators in Peshawar city. At the time of this research approximately Rs. 800,000/- were collected as fine from the violators. This indicate satisfactory vigilance of the KP police force to achieve the policy objective.
KP provincial government did not limit its response on the federal directives and NDMA only. It also attempted to improve its analytical competence by using scientific methods and collecting evidence through surveys. A key government official informed that although testing in the province was free but as the province acquired more kits and its testing capacity increased the public’s willingness to take the tests decreased. Since, the public response to testing was voluntary people could not be forced to take the test. As a result, the true status of COVID-19 in the province could not be ascertained. To inform future strategy in the province it was decided to fund research conducted by Khyber Medical University, Peshawar, and Quaid-e-Azam University, Islamabad, to investigate the real reasons for this drop. The official added, ‘we could not afford to show any laxity in the matter’. This behaviour also indicated a strong desire of the provincial government to control the spread of pandemic and make policies based on scientific evidence.
Another factor that became prominent was the province relationship with the centre. KP had the PTI government which worked harmoniously with the PTI government in the centre. Because of this political support, both from above and below, a key factor for sustaining policy capacity was made available to the KP government. Furthermore, KP police, due to the many institutional reforms implemented from 2013 to 2017, enjoyed a good reputation. Together, these factors played an instrumental role in improving the political legitimacy of the provincial administrators and law enforcing agencies like KP police.
Overall harmonious relations with the centre, vigilant and reformed administrative and police department of KP, strategic use of existing resources like the polio surveillance team and desire to build its own analytical competence with the help of scientific data helped the KP government to control the fast spread of disease in the province.
Sindh
The province of Sindh has 29 administrative districts and the metropolitan city and the country’s business hub of Karachi, which has a population of 14,916,456 (PBS, 2017). Other key cities in Sindh are Hyderabad with a population of 1,734,309, Sukkar with 499,900 and Larkana with 490,508 (PBS, 2017). An estimated 4 million daily wagers work in Karachi alone compared to 4 million daily wagers working in the whole of the Punjab province (PBS, 2017; Gullup, 2014). According to the Asian Development Bank report, the impact of COVID-19 on Karachi alone is expected to result in a revenue loss of 380 billion rupees for Pakistan (Noreen et al., 2020). The case study of the first 100 cases and another epidemiology surveillance report issued by the NIH showed that in April 2020 25% of the cases reported in the country were reported in the city of Karachi, Sindh (NIH, 2020, p. 2). A key informant from Karachi, a businessman named Sohail Sarwar, explained that a number of micro, small and medium-size enterprises operated in Karachi. ‘Any disruption in the supply chain, in the daily transactions, unavailability of labour, raw materials, and transportation or insufficient resources, is disastrous for them. These enterprises were most vulnerable to the lockdowns. People associated with these enterprises were also unwilling to stay home during lockdowns. Thus, when the GoP imposed the lockdown on 22 March 2020, the lockdown failed in Sindh’. 3 Furthermore, the economic relief package for small businesses and daily wagers by the federal government was announced at the end of April 2020. It was further divided among all the provinces and, according to the informants, it was insufficient to resolve the problems of Karachi. The information was also cross-checked and a number of archived studies have supported it (Imran Nisar et al., 2020, p. 5; Shafi et al., 2020; SMEDA, 2020, p. 10; World Bank, 2020). Thus, the impact of the lockdown on the free market economy of Karachi was the main determinant for the failure in the successful implementation of government policies. At the same time, it points to the weak steering capacity of the Sindh government. The advisor to the Sindh Chief Minister, barrister Murtaza Wahab, talking to a national daily, also bluntly admitted that the lockdown in Sindh was not successful (Dawn, 2020). Starting from the country’s first reported case of COVID-19 reported in Karachi on 26 February 2020, the province continued to show the most reported cases and fatalities on the national scoreboard.
These factors also explain the concentration of the allocated resources in Karachi. For the 29 administrative districts of Sindh, only 4 tertiary hospitals were dedicated to the crisis, with 3 in the provincial capital Karachi only and one in Hyderabad. Two quarantine facilities in the whole province were established: one in Sukkar, of 2,000 beds and the other one at Doaba Hospital, Karachi with 100 beds only. Five medical Isolation wards with just 151 beds were set up in the urban centres of only four districts, namely Karachi, Jacobabad, Khairpur and Sukkar (GoP, 2020, p. 4). Out of the 32 testing facilities, 26 were operating in Karachi alone. Critical review of the list shows that of these 16 are owned by the private sector, one by public/private and the remaining nine by the public sector. One testing facility each is in Hyderabad, Sehwan, 4 Sukkar and Larkana (GoP, 2020, p. 2). Later, on the request of chief minister Murad Ali Shah, Pakistan military also helped the Sindh government to set up a separate quarantine facility of 10,000 beds at the EXPO centre Karachi to isolate and treat confirmed patients (The News, 2020). Overall, the inability to dedicate sufficient resources and the limited operational capacity point to a weak steering ability of the Sindh government.
The Sindh government, however, was able to extend its operational competence to the rural districts of Sindh, such as Tharparkar, Umerkot, Shangar and Thatta, which suffered from acute resource shortages, such as hospital capacity, availability of isolation wards and ventilators by networking with non-state actors like the Thar Education Alliance (TEA). Unlike the Agha Khan Foundation operating in GB, the NGO did not provide additional resources but worked with the rural communities, especially the women educating them; to follow the SOPs of hand hygiene and sanitation, to follow the norms of social distancing, not to shake hands, to avoid large gatherings like religious gatherings, weddings or festivals and to spend maximum time at home. TEA claims success in achieving its objectives and bringing about behavioural change (Qureshi, 2020).
Another factor that considerably contributed towards weakening the political competency of the Sindh government was the tension between the Sindh’s political government, presently with Pakistan People’s Party (PPP), and the centre. The basis of the conflict was the corruption cases against the party top leadership. In August 2020, right in the middle of the pandemic, PPP leadership first made a political alliance named ‘Pakistan Democratic Movement’ (PDM) with the Muslim League-Nawaz Group, mainly from Punjab, and launched a nation-wide protest movement (Shehzad, 2020). PDM urged the public to come on the streets and protest against the central government’s interference in Sindh’s affairs (The Nation, 2020). In the ongoing pandemic crisis, this political battle adversely affected the critical centre provincial coordination which had helped other provinces overcome their analytical, operational and political capacity deficits. This behaviour from Sindh’s key political party and its political government also directly impacted the legitimacy of its administrative and law-enforcing agencies for correct implementation of NDRM directives formulated for controlling the spread of disease and increased the risk for their supporters and the greater population of Sindh. According to one official, who did not want to share his identity, administrative agencies had no support from the provincial government to crack down on the violators of SOPs. He said, ‘We had no legitimacy left to check or control people when the government itself asked the public to come on street and protest’. Presently, on the national scoreboard, Sindh scores highest with 142,917 confirmed cases and 2,591 fatalities.
Punjab
According to the 2017 population census Punjab is the most populous province of Pakistan with a population of 110,017,465. On the national scoreboard presently, Punjab stands second with the most reported COVID-19 cases. Apart from the population problem, the story of the spread of COVID-19 in Punjab is of grave negligence by the political government and administrators of Punjab. According to NIH data, the first confirmed patient reported in the province had no travel history from outside Pakistan, but the spread of the disease in the province is attributed to one religious congregation. On 10 March 2020, the Tablighi Jamaat held its annual congregation in the city of Riwand, near the provincial capital of Lahore. Approximately 70,000 to 80,000 people attended the camp; of these 3,000 arrived from 40 countries before the international flights closed due to the pandemic. The Lahore Division Commissioner, District Inspector General Police (DIG) and Capital City Police Officer held meetings with the organisers to cancel the congregation. Although Punjab administrators and Punjab police are considered the most powerful and experienced, these officials ‘failed’ to convince the congregation organisers to comply with the GoP directives and cancel the congregation. Informants were of the opinion this was because the officials themselves did not believe in the gravity of the situation or failed to anticipate the problem it was likely to cause. What followed became an international embarrassment. ‘There were rumours that the congregation ended early mainly because of COVID-19 symptoms appearing in some members of the attending groups’. 5 On 13 March 2020, observers also saw a large number of attendees ‘freely leaving Riwand for their hometowns’ without any testing (IANS, 2020). Once again, the Punjab government and Lahore district administration which as per the NDRMA directives were required to detect, test, isolate, treat and contact trace every case, and take adequate measures to ensure that disease transmission was under control, failed to effectively isolate the attendees and track their movements.
Those who left the congregation also continued with the proselytising activities and became a catalyst in exasperating the situation not just within the province but also in other provinces of the country and outside Pakistan. After reports of negligence became public, the Punjab administration tested 10,263 members of the Tablighi Jamaat only, and, according to NIH, of these 539 results came out as positive and 404 of these were from the Riwand Markaz itself. Thirty-one were traced to ‘Hafizabad’, Punjab, four cases in Sindh, and a cluster was created due to the proselytising activities in the federal area of Barakhau, Islamabad District (NIH, 2020). Following the incident, from 5 April to 10 April, the cumulative reported cases in Punjab increased by 53%, and 49% of the cases registered in Pakistan (Abid et al., 2020; NIH, 2020). In interviews with the press various district administrators also admitted that the cases in their districts were traced to the Riwand congregation (Chaudhry, 2020; Dawn, 2020). Various international sources also traced COVID-19 cases back to the Riwand congregation including three cases reported in Gaza, Palestine, five in Nigeria and five in Kazighistan (Ahmed, 2020; Chaudhry, 2020; Hadid, 2020). Rd. Yasmeen Rashid, the health minister of Punjab, however, blamed the Tablighi groups and not the administrators or the law enforcers for the criminal negligence. A key informant from Lahore stated, ‘The political and administrative institutions in Punjab may be experienced but their preferences and priorities are political. Due to the political backing, Punjab administration and Punjab Police fear no one and have become complacent’.
Like Sindh, the resource allocation for COVID-19 in Punjab was again concentrated in its urban centres. NIH data showed that out of 36 districts of Punjab the quarantine facilities were only set up in six districts of Punjab. Six tertiary hospitals were dedicated to six major cities of the province, namely, Lahore, Rawalpindi, Multan, Sialkot, Faisalabad and Rahim Yar Khan (GoP, 2020, p. 1). Ten quarantine facilities of 948 beds were set up in six cities, namely, Lahore, Faisalabad, Multan, Sialkot, Bahawalpur and Dera Ghazi Khan (GoP, 2020, p. 2). A total of 48 testing facilities in 10 major cities were present, 27 of these were in the provincial capital Lahore (GoP, 2020, p. 1). In the rest of the province, isolation wards were established at 50 hospitals in 34 districts, but with 955 beds only (GoP, 2020, p. 3).
In June 2020 the government of Punjab changed its quarantine policy. All quarantine centres were closed in the provincial capital and other cities, including the one in Riwand (Hasnain, 2020). It also changed its policy for international travellers. Earlier travellers coming from abroad were tested and quarantined for 48 hours. After June this time was reduced to 24 hours and those with negative test results were allowed to go home. A national daily also quoted the Lahore Deputy Commissioner as saying that ‘Lahore already has 20,000 confirmed cases so what difference anyone returning from abroad with the virus would make’ (Hasnain, 2020). Earlier in the case of positive results, the traveller’s contact details were shared with the district administration. After June 2020, all passengers were allowed to go home even before receiving the test results and instructed to self-isolate themselves at their homes. If the test result came positive the travellers were asked to continue with self-quarantine and seek medication. However, the districts received no information on how many new infected cases entered the district, therefore they could not monitor them. Evidence before this research also indicates that the Punjab government’s decision not to track those tested positive with COVID-19 was driven by instrumental calculation of its own strategic and political interests more than the interests and well-being of the greater public. Transferring the blame to the religious workers worked as a veal to hide this incapacity. An important implication of this negligent behaviour was its direct impact on the GoP national scoreboard, correct resource allocation for the second wave of the pandemic, and future policies. It also casts serious doubts on Punjab standing on the national scoreboard, where Punjab presently shows 102,677 confirmed cases and 2,335 fatalities, closely following Sindh’s 143,836 confirmed cases and 2,598 fatalities, the highest in the country.
Another problem in Punjab was the tension with the centre. PML-N, Punjab’s key political party, presently sitting in the opposition, called the public to come out on the streets and demonstrate against Imran Khan’s government in the centre and against the accountability cases filed against PML-N key members. Processions were held in major cities as a show of strength, which were attended by hundreds of people. The conflict contributed towards aggravating the crisis and made it even easier for the negligent administration to sit back and relax.
The current study also found convincing evidence from primary and secondary sources that the smart lockdowns imposed during June–July 2020 in the urban centres of Punjab also failed. For example, in Faisalabad, the second most populated city in Punjab with a population of 7,874,790 (PBS, 2017), the district administration failed to make the smart lockdown a success (Daily Times, 2020). One district administrator from Faisalabad was also contacted via phone. He said, ‘WHO recommends 50,000 tests per day, we do not have this much capacity or resources. Besides we cannot make people follow something they do not believe in’. Similarly, smart lockdowns in the industrial district of Gujrat, Gujranwala, Multan and Sialkot were also not successful.
During the COVID-19 crisis, the Punjab government’s inability to stop the high-risk religious congregations before time and later control its spread to the rest of the province indicate its weak analytical and operational competence. The complacent behaviour of the provincial administration and law-enforcing agencies also contributed to the failure of smart lockdowns in the major cities of Punjab. Overall, even in the time of the COVID-19 crisis politics dominated the government and institutional behaviour in Punjab more than service delivery.
Analysis and Conclusion
This research used the policy capacity framework to understand the reason for the variance in Pakistan’s five provinces’ response to the COVID-19 pandemic. The evidence collected showed that while lack of resources remained the main problem for all the provinces of this South Asian developing country but strong relations with the centre, strategic use of existing resources, timely and effective networking and collaboration with international organisations and domestic NGOs, proper utilisation of the communication and coordination structures made by NDMA at all tiers of government helped the provinces of Baluchistan, GB and KP to markedly improve their limited operational competencies. Collaboration with organisations like Agha Khan Foundation, CPEC and UNHCR also increased the outreach to the rural areas. As a result, public confidence in the respective provincial governments increased. The public responded far more positively to the government’s request for lockdowns, social distancing and the prescribed SOPs were observed and the spread of the pandemic in these provinces was controlled.
Tension with the centre, free market economy, weak steering abilities of the individual provincial government and politics adversely impacted provincial capacity to control the spread of COVID-19 in Punjab and Sindh. The key issue in the province of Sindh was its densely populated urban centres, a large number of small-, medium- and large-scale enterprises, and the weak steering ability of the provincial governments. The resources available to the province were almost exhausted in its urban centres. In Punjab, sadly politics, and not service delivery, dominated decision making and overshadowed the analytical and operational competence of both its political and administrative institutions. Punjab’s capital city administration’s criminal negligence in not controlling, testing and tracking the attendees of the religious congregation resulted in exacerbating the situation in the rest of the province and became an embarrassment for the country. Together the complacent and negligent behaviour of Punjab administrative and law-enforcing agencies and the lack of public support for the announced policies aggravated the COVID-19 crisis in Punjab. The untimely call for protest by the key opposition parties in both these provinces made political support for the NDMA’s policy action and directives further difficult. While operational competence was a critical point of the Sindh government, political incompetency was the ‘Achilles’ heel’ of the Punjab government.
Overall, this comparative study revealed that the variance in the provincial response to COVID-19 in Pakistan was not determined by the past experience but by the variance in the analytical, operational and political competency of each province. Focus on improving analytical and operational competency in the time of crisis also helped in improving the political competency. In Pakistan, the provinces that proactively worked to build all these competencies fared much better in controlling the spread of COVID-19.