
Abstract
In the silent realm of decomposition, where time obscures truth and scavengers leave deceptive marks, distinguishing antemortem trauma from postmortem artefacts becomes a formidable challenge. This case unravels a chilling forensic mystery—a severely decomposed male body discovered abandoned and extensively scavenged, with its disfigured state suggesting postmortem animal activity. Yet, something did not add up. X-rays performed before autopsy revealed a suspicious cluster of radiopaque densities in the cranio-cervical region, demanding closer scrutiny. Guided by these unexpected findings, meticulous dissection uncovered multiple metallic projectiles aligned in a ballistic path, exposing a concealed shotgun injury. This case illustrates the indispensable role of radiological examination in detecting covert trauma in decomposed remains and urges its integration into standard autopsy protocols, especially when scavenging artefacts blur the line between decomposition and foul play.
Introduction
Accurate differentiation between antemortem injuries and postmortem artefacts remains a cornerstone of forensic pathology, particularly in decomposed bodies where tissue degradation and animal scavenging may mimic vital trauma. 1 Misinterpretation may critically affect medicolegal conclusions. Radiological evaluation, especially conventional X-rays, assists in detecting foreign bodies, reconstructing projectile trajectories and clarifying obscured wound patterns.2, 3
Whole-body radiography prior to autopsy has proven invaluable in identifying concealed ballistic trauma. Gouda and Mestri documented the role of piecemeal radiography in firearm fatalities, demonstrating detection of retained pellets not evident externally. 4 Additional regional studies emphasise medicolegal implications of firearm injuries in India, reinforcing the need for systematic radiological evaluation. 5 Shotgun injuries present further diagnostic difficulty due to pellet dispersion, atypical entry defects and concealed ballistic tracks.6–8
Several forensic reports have highlighted how radiology uncovers firearm injuries in severely decomposed bodies, preventing misclassification of the manner of death.9, 10 We present a unique case where high-density radiopaque clusters on screening X-ray revealed a hidden shotgun injury initially mistaken for animal scavenging, ultimately proving homicide.
Case Report
Brief History
A 27-year-old male, employed as a private car driver, went missing after completing a transport assignment to a neighbouring district. He remained in contact until the same evening, after which communication suddenly ceased. Approximately 24 hours later, his partially decomposed body was discovered lying amidst dense shrubbery near a canal embankment on a hot summer day. Identification was established through an Aadhaar card recovered at the scene. A cash amount of ₹20,000 was missing, and his vehicle, a Maruti Swift car, had been looted, raising strong suspicion of robbery followed by homicide. An FIR was registered under relevant sections relating to murder and concealment of evidence.
Crime Scene Findings
The body was found in a right lateral position exhibiting advanced decomposition, generalised bloating and extensive maggot infestation (Figure 1). The face was unrecognisable. Distinct scavenging defects were present over the buttocks, thighs and nape of the neck. Soft tissue destruction was initially attributed to postmortem animal activity.
The Decomposed Male Body is Discovered in the Right Lateral Position, Amidst Roadside Bushes in an Abandoned Place. The Clothes are Displaced and Torn. Advanced Bloating with Maggot Activity is Present. The Situation and Body’s Position Raised Suspicion of Foul Play.

Autopsy Findings
The deceased was clothed in a blue shirt, grey trousers and torn blue underwear, all displaced and heavily soiled. The body measured 185 cm in length and had an estimated antemortem weight of 85 kg. Extensive putrefaction with dense maggot activity was present.
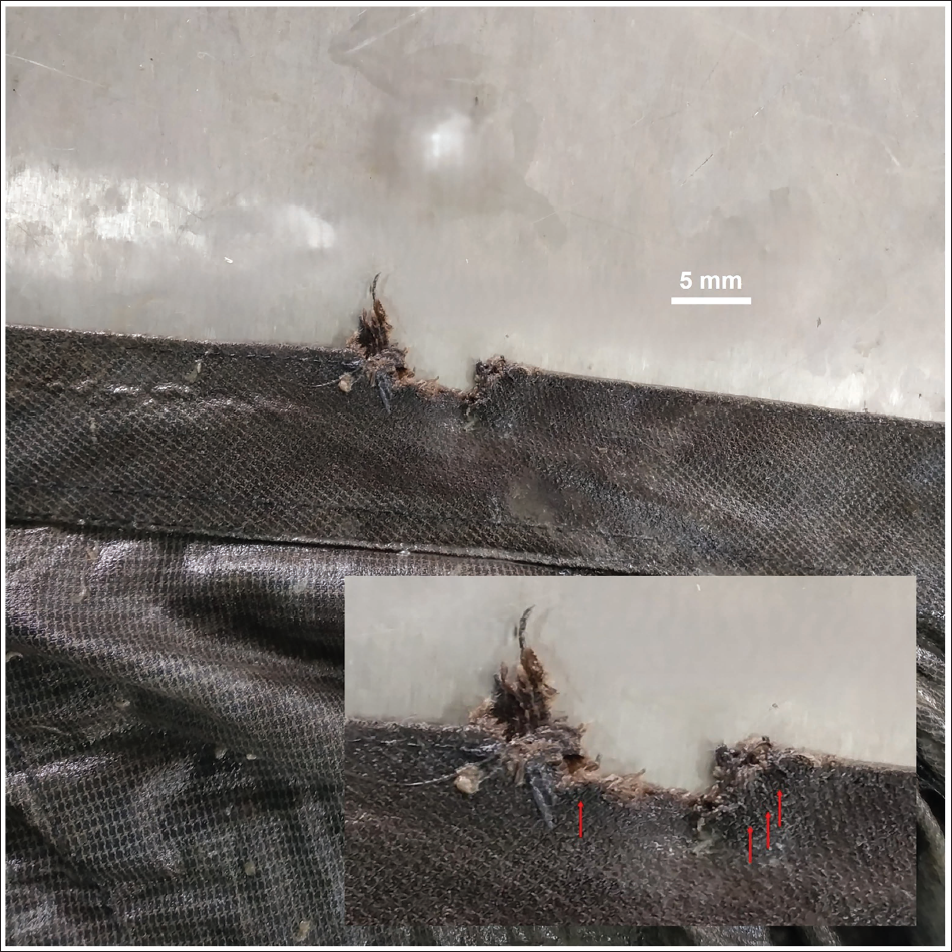
A 2 × 0.5 cm irregular tear with a punched-out defect was noted on the upper back collar of the shirt, showing frayed margins and surrounding blackening and searing (Figure 2). A faint burnt odour was perceptible on close inspection.
Outer Aspect of the Shirt’s Collar, Showing an Irregular Defect and Tear with Tattered Margins, Suggesting Garment Damage from a Gunshot Blast. Inset Shows a Circumscribed Band of Blackening and Searing Around the Defect (Arrows).
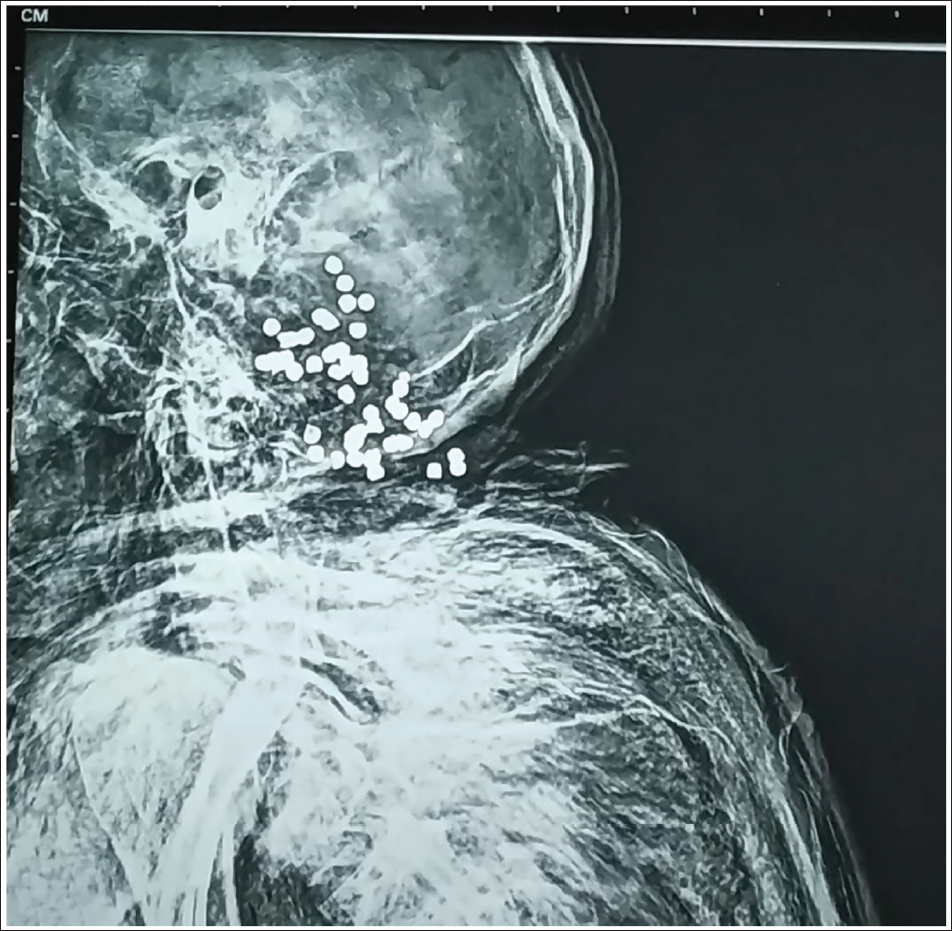
Comprehensive whole-body postmortem radiography was conducted using a stationary digital radiography system (500 mA). Two whole-body images, AP and lateral projections, were acquired, which revealed multiple clustered, rounded radiopaque pellets in the posterior cranial fossa and cervical region, confirming a shotgun injury (Figure 3).
X-ray Image Showing Clusters of Shotgun Pellets in the Nape of Neck and Occipital Region.
A 3.0 × 2.5 cm D-shaped defect with scalloped margins and satellite puncture abrasions was identified over the nape of the neck, 3 cm below the external occipital protuberance, straddling the midline (Figure 4). The wound was directed upward, forward and medially.
D-shaped Shotgun Wound Defect Over the Nape of the Neck, Exhibiting Crenulated Margins, Right Sided Bevelling and Surrounding Satellite Lesions from Individual Pellets.

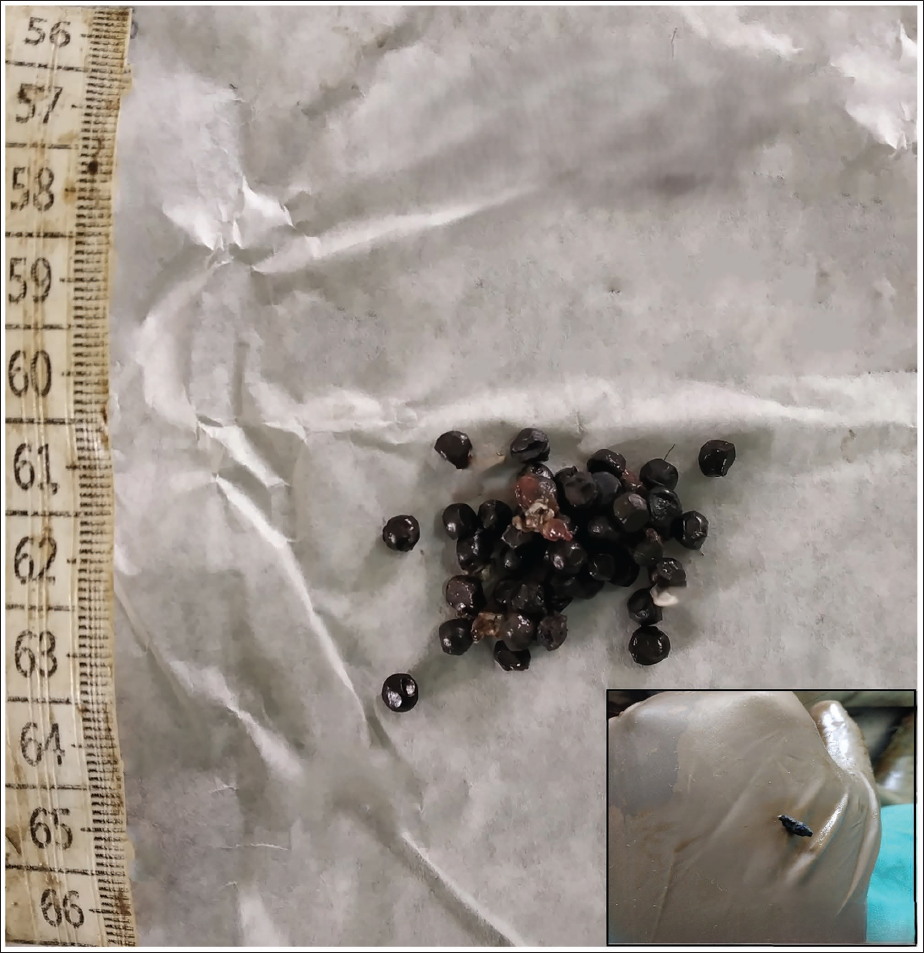
Layer-by-layer dissection revealed ecchymosis, a ballistic cavity extending into the cervical region, and multiple embedded metallic pellets (Figure 5), white plastic fragments and black sponge-like wad components consistent with a close-range shotgun discharge (Figure 6).
Multiple Pellets Recovered from the Successive Layers of Subcutaneous Tissues (Encircled).

Multiple Pellets Recovered from the Wound Track (Displayed on a White Paper). Inset: A Fragmented Sponge-like Wad Remnant Retrieved from the Ballistic Channel, Displayed on the Glove.
Two pellets were lodged in the C1–C2 disc space, with others dispersed within liquefied cranial tissue. The cranio-cervical junction was haemorrhagic and disrupted, although vertebrae remained intact. The spinal cord was pulped. No other injuries were identified. Scavenged areas showed no vital reaction. Chemical analysis detected no poisons. Integrating the autopsy findings with the available case history and situational circumstances, the postmortem interval was assessed to be in the range of three to five days.
Discussion
Radiographic imaging plays a critical role in detecting and localising retained projectiles, assessing trajectories and differentiating firearm injuries from postmortem artefacts, particularly in decomposed or burnt bodies where classical signs such as soot, tattooing or cavitation may be absent.11–15 Warmer climates accelerate putrefaction, often obscuring vital trauma and complicating the interpretation of injuries. 15 The earliest radiographic demonstration of shotgun pellets was published in 1896 and guided successful pellet removal, highlighting the long-standing value of radiology in firearm trauma. 12
In the present case, radiology proved decisive in uncovering a concealed shotgun injury that had initially been mistaken for animal scavenging. The clustered nature of the radiopaque pellets visible on whole-body radiography strongly indicated a ballistic mechanism rather than postmortem destruction. Similar diagnostic value has been demonstrated in earlier forensic cases.4–10, 16, 17
Regional case studies from India have emphasised the medicolegal importance of radiology in interpreting firearm injuries and preventing erroneous conclusions.4–7, 10 In particular, Pradeep and Shashikanth described a fatal homicidal shotgun wound at an atypical location, highlighting the diagnostic challenges posed by shotgun trauma. 6 Pinheiro et al. reported a case in which radiography revealed an intracranial pellet cloud in a body initially suspected of road traffic trauma, thereby excluding accidental causation and confirming fatal shotgun injury. 10
Atypical presentations of ballistic trauma may lead to misinterpretation. Buchade et al. described a series of cases demonstrating misleading ballistic patterns requiring careful radiological assessment for accurate medicolegal interpretation. 8 The present case similarly underscores the forensic value of radiology in identifying retained pellets and reconstructing projectile paths where external indicators have been lost due to decomposition or scavenging.
Radiological detection of metallic fragments aids in confirming firearm injuries and may reveal prior firearm-related trauma.18, 19
Beyond shotgun wounds, analyses of bullet trajectories with skeletal involvement—such as the keyhole fracture described by Harada et al. and the cranial disintegration in a Krönlein shot reported by Gupta and Tiwari—underscore the capacity of bone to preserve ballistic signatures.20, 21
Postmortem animal predation may simulate firearm defects, complicating interpretation. In such scenarios, forensic radiology—particularly micro-CT—can identify retained projectiles and gunshot residues even in decomposed remains.22, 23
In the present case, scalloped wound margins, satellite pellet defects, and recovery of wad-like fragments indicated a close-range shotgun discharge. These findings were corroborated by examination of the shirt, although wound characteristics may vary with weapon modification and test-firing results. 24
Conclusion
Differentiating scavenging artefacts from true trauma in decomposed remains a significant forensic challenge.
Radiology proved essential in detecting metallic pellets and guiding autopsy interpretation, confirming a concealed shotgun injury that may otherwise have been misclassified as postmortem animal activity.
Routine integration of whole-body radiography and, where feasible, postmortem CT should be considered standard practice in decomposed or artefact-laden cases.
Enhanced collaboration between forensic pathologists and radiologists improves diagnostic accuracy and strengthens medicolegal reliability.
Embedding forensic radiology within routine autopsy workflow improves scientific precision and strengthens justice by preventing misclassification of covert firearm deaths.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Not applicable.