
Abstract
Dental age estimation is an integral component of forensic identification and medico-legal investigations. Kvaal’s method, based on the radiographic assessment of regressive dental changes, is widely used in adults; however, its accuracy varies across populations and age groups. To evaluate the accuracy and reliability of Kvaal’s dental age estimation method in an Indian adult population and to assess its performance across different age groups and sexes. A cross-sectional study was conducted at Jawaharlal Nehru Medical College, Belagavi, from August 2023 to August 2024. The study included 200 adults (100 males and 100 females) aged 20–80 years. Digital periapical radiographs of permanent maxillary central incisors were analysed using Kvaal’s method, focusing on pulp-to-tooth measurements reflecting secondary dentin deposition. Estimated ages were compared with chronological ages using descriptive statistics, paired t-tests, intraclass correlation coefficients and Lin’s concordance correlation coefficient. The mean chronological age was 48.7 ± 14.5 years, while the mean estimated age was 46.5 ± 12.3 years, showing an overall underestimation of −2.65 years. Higher accuracy was observed in the 20–50-year age group, with significant underestimation in individuals above 60 years. The Lin’s concordance correlation coefficient demonstrated good agreement overall (0.82), with higher reliability in males (0.84) compared to females (0.81). Kvaal’s method provides reliable age estimation in younger and middle-aged Indian adults but demonstrates reduced accuracy in elderly individuals. Population-specific modifications and integration of advanced imaging and analytical techniques may improve age estimation in older age groups.
Introduction
Dental age estimation is a cornerstone of forensic science, aiding human identification and age verification in medico-legal contexts, including cases involving unaccompanied minors and asylum seekers. 1 Although widely applied, the accuracy of dental age estimation varies across age groups and is often reduced in older individuals due to complex and less predictable age-related dental changes.2, 3 Kvaal’s method, introduced in 1995, is a non-invasive radiographic technique based on regressive dental changes such as pulp chamber reduction and secondary dentin deposition. 4 Dental regression is influenced by genetic, nutritional and environmental factors, making population-specific validation essential, particularly in a genetically and socio-culturally diverse country like India.5, 6 Studies conducted in Brazilian and Serbian populations have reported acceptable accuracy of Kvaal’s method in younger adults but increased estimation errors beyond 50 years of age.2, 3 However, comparable comprehensive data from Indian adult populations remain limited, highlighting the need for contextual evaluation. 7 Recent advances in forensic odontology, including cone beam computed tomography (CBCT) and artificial intelligence (AI)-based analytical models, have demonstrated the potential to improve age estimation by enabling three-dimensional assessment and advanced predictive analysis.8, 9 These developments are especially relevant in forensic scenarios involving advanced decomposition, burning or fragmentation, where dental structures may remain the only reliable means of identification.10, 11 Accordingly, the present study evaluates the accuracy of Kvaal’s dental age estimation method across different age groups in an Indian adult population and explores the need for methodological refinement to enhance forensic applicability.
Materials and Methods
Study Design and Setting
This cross-sectional observational study was conducted at Jawaharlal Nehru Medical College, Belagavi, Karnataka, from August 2023 to August 2024. The study was approved by the Institutional Ethics Committee and was carried out in accordance with the Declaration of Helsinki, ICMR guidelines and ICMJE recommendations. Written informed consent was obtained from all participants, and confidentiality was strictly maintained.
Sample Size and Sampling Strategy
The study included 200 adults (100 males and 100 females) aged 20–80 years. The sample size was selected based on feasibility and consistency with earlier validation studies of Kvaal’s method that used similar sample sizes to assess age-related accuracy. Participants were recruited through consecutive convenience sampling from patients attending the institutional dental outpatient clinic during the study period, ensuring balanced representation across sex and adult age groups.
Inclusion and Exclusion Criteria
Participants with high-quality digital periapical radiographs taken for routine diagnostic purposes within the previous one year and having intact permanent maxillary central incisors (number 11 or number 21) were included. Individuals were excluded if the selected teeth showed caries, restorations, crowns, endodontic treatment, periapical pathology, developmental anomalies or poor radiographic quality (Figure 1). Subjects with a history of orthodontic treatment involving maxillary incisors or systemic conditions known to affect dentin deposition were also excluded to minimise confounding. As the sample was drawn from a single geographic region, regional variation in dental morphology was considered uniform.
Panoramic Radiograph (OPG) Depicting Maxillary and Mandibular Structures for Age Estimation Analysis.

Radiographic Protocol
Standardised digital periapical radiographs were obtained using a digital intraoral X-ray unit. Images were acquired using the paralleling technique with position-indicating devices to minimise distortion. Exposure parameters were kept consistent (60–70 kVp, 7–8 mA, exposure time 0.2–0.4 seconds). Magnification errors were controlled by using calibrated digital software, and all measurements were expressed as ratios rather than absolute values.
Dental Measurements and Application of Kvaal’s Method
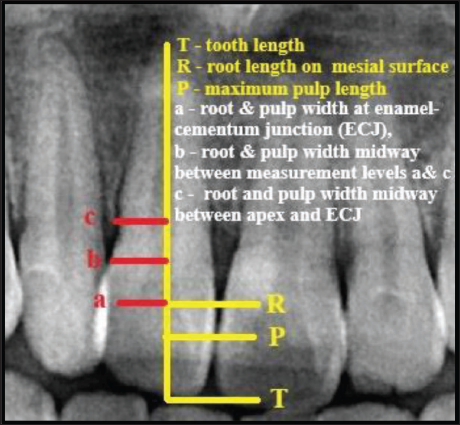
Radiographic assessment focused on regressive dental changes, particularly pulp chamber reduction and secondary dentin deposition. Measurements included total tooth length, root length, pulp length and pulp and root widths measured at three predefined levels. Pulp-to-tooth and pulp-to-root ratios were calculated and substituted into Kvaal’s regression equations (Figure 2). The estimated age was derived by applying regression coefficients to these ratios, based on the principle that pulp dimensions decrease progressively with age due to secondary dentin deposition.
Graphical Depiction of the Measures Conducted in this Research.
Observer Reliability and Bias Control
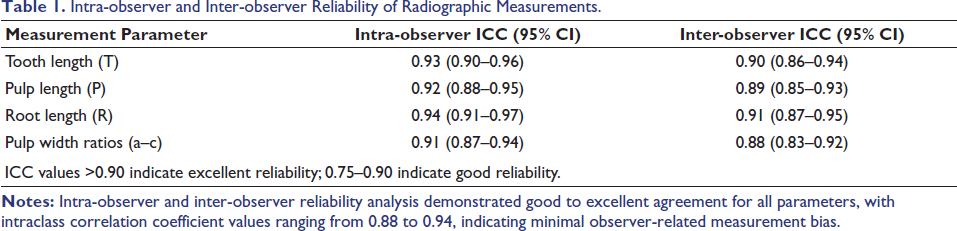
All measurements were performed independently by two trained examiners who were blinded to the chronological age of the participants. Prior calibration was undertaken to standardise measurement techniques. To assess reliability, 20% of radiographs were re-evaluated after a two-week interval. Intra-observer and inter-observer reliability were assessed using intraclass correlation coefficients, with values exceeding 0.90 indicating excellent agreement. These findings are presented in the results section (Table 1).
Intra-observer and Inter-observer Reliability of Radiographic Measurements.
Statistical Analysis
Data were analysed using SPSS version 20.0 and jamovi version 2.4 (2023). Descriptive statistics were calculated for chronological and estimated ages. Normality was assessed using the Kolmogorov–Smirnov test (Table 2). Agreement between estimated and chronological ages was evaluated using paired t-tests and Lin’s concordance correlation coefficient. Stratified and regression analyses were performed to assess age-group-wise accuracy. A p value < .05 was considered statistically significant.
Quantified Data Normalcy in the Current Study.

Results
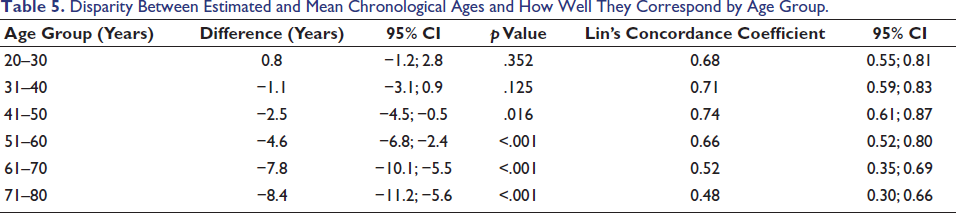
The analysis of 200 radiographs (equal male–female distribution; age range 20–80 years) demonstrated a significant difference between estimated and chronological age using Kvaal’s method. The study population comprised 200 participants with equal sex representation, including 100 males (50.0%) and 100 females (50.0%). Participants were aged between 20 and 80 years, with a relatively uniform distribution across age groups. The highest representation was observed in the 41–50 years and 51–60 years age groups (each 20.0%), followed by individuals aged 31–40 years and 61–70 years (each 17.5%). Participants in the youngest (20–30 years) and oldest (71–80 years) age groups each constituted 12.5% of the study population, ensuring adequate representation across adult age decades. Regarding tooth selection for radiographic analysis, the permanent maxillary right central incisor (FDI tooth number 11) was evaluated in 115 participants (57.5%), while the permanent maxillary left central incisor (FDI tooth number 21) was assessed in 85 participants (42.5%). The inclusion of both maxillary central incisors provided balanced representation and ensured consistency in applying Kvaal’s dental age estimation method. The mean estimated age (46.5 ± 12.3 years) was significantly lower than the mean chronological age (48.7 ± 14.5 years), indicating an overall underestimation of −2.65 years (p < .001). Age-stratified analysis showed good agreement in individuals aged 20–50 years, while statistically significant underestimation was observed in participants aged above 60 years (p < .001), reflecting reduced accuracy in older age groups. Overall agreement between estimated and chronological age was good, with a Lin’s concordance correlation coefficient of 0.82. Sex-wise analysis revealed slightly higher concordance in males (0.84) compared to females (0.81), though agreement remained statistically significant in both groups. Measurement reliability was high, with intra-observer and inter-observer intraclass correlation coefficients ranging from 0.88 to 0.94, confirming minimal observer-related bias (Tables 3 to 5.
Dispersion and Central Tendency Values for Continuous Variables.

Disparity and Rates of Concordance Between Estimated and Chronological Ages.

Disparity Between Estimated and Mean Chronological Ages and How Well They Correspond by Age Group.
Discussion
Comparison with Previous Studies
Age estimation is a fundamental component of forensic practice, as chronological age does not always correspond with biological or dental age due to interindividual variability influenced by genetic, environmental and lifestyle factors. In forensic odontology, dental age estimation seeks to bridge this gap by correlating regressive dental changes with chronological age. 6
The present study demonstrated that Kvaal’s dental age estimation method performs reliably in younger and middle-aged adults (20–50 years) but shows a significant decline in accuracy in older age groups (61–80 years). This trend is consistent with observations from Brazilian populations, where increased estimation errors beyond 50 years were attributed to variability in secondary dentin deposition with advancing age. 2 Similar underestimation patterns have also been reported in Serbian adult populations using Kvaal’s method. 3
Sex-wise analysis in the present study showed good concordance in both males and females, with slightly higher agreement in males, which is in accordance with findings from Indian studies reporting reliable age estimation when standardised measurement protocols are followed. 7 Collectively, these findings indicate that while Kvaal’s method is reproducible and dependable in younger adults, age-related morphological complexity limits its precision in elderly individuals across populations.
Strengths
A major strength of this study is the balanced sex distribution and wide adult age range, which allowed meaningful age-stratified analysis. The use of standardised digital periapical radiographs and ratio-based measurements minimised magnification-related errors and improved reproducibility. High intra-observer and inter-observer reliability further confirmed that measurement bias had minimal influence on the results.
Another important strength is the population-specific evaluation in an Indian cohort, addressing a significant gap in the literature. Given India’s ethnic, nutritional and socio-environmental diversity, validation of dental age estimation methods within local populations is essential for medico-legal reliability.5, 6
Limitations
This study has certain limitations that must be acknowledged. Being a single-centre study, regional variations in dental morphology across different Indian populations could not be assessed. Although confounding factors such as orthodontic history and systemic diseases affecting dentin deposition were excluded, subtle individual biological variations in dental aging could not be eliminated.
Additionally, reliance on two-dimensional periapical radiographs limits the assessment of three-dimensional pulp changes, particularly in elderly individuals, which may partly explain the reduced accuracy observed in advanced age groups.
Future Directions and Technological Integration
The declining accuracy of Kvaal’s method in older age groups highlights the need for methodological refinement. CBCT enables the three-dimensional assessment of pulp volume and dentin deposition, providing more precise morphological information than conventional radiographs.8, 12 AI-based approaches further enhance age estimation by integrating multiple dental variables and modelling non-linear age-related changes, thereby improving predictive accuracy across age groups. 9
From a practical standpoint, Kvaal’s method using periapical radiographs remains highly feasible for routine medico-legal age estimation in most Indian institutions due to its low cost, non-invasive nature and wide availability. 5 However, implementation of CBCT and AI-based systems may face challenges such as limited availability of CBCT units, higher costs, radiation considerations and the need for trained personnel.
Despite these hurdles, selective use of CBCT and AI-assisted analysis in disputed or high-stakes medico-legal cases—particularly involving elderly individuals—may be justified, as studies consistently report improved accuracy and concordance compared to conventional methods.8, 9 Development of population-specific regression models and AI algorithms tailored to Indian demographics would further enhance reliability and legal defensibility. 6
Overall Implications
Kvaal’s dental age estimation method remains a reliable and reproducible tool for younger and middle-aged adults; however, its limitations in elderly populations must be recognised. The present study reinforces the importance of population-specific validation and supports a hybrid approach combining conventional radiographic techniques with advanced imaging and AI to enhance accuracy and medico-legal credibility in the Indian context. 6
In the Indian medico-legal setting, periapical radiograph-based age estimation remains practical and widely applicable across institutions owing to low cost, ease of availability and minimal radiation exposure; however, its accuracy declines with advancing age, underscoring the need for complementary approaches in disputed or high-stakes cases. 13
Conclusion
This study demonstrates that the Kvaal’s dental age estimation method is a reliable and reproducible tool for estimating age in younger and middle-aged Indian adults, with excellent intra- and inter-observer agreement when standardised protocols are followed. However, its accuracy declines significantly in individuals above 60 years of age, reflecting the complex and variable nature of age-related dental changes in the elderly.
For routine medico-legal age estimation, Kvaal’s method remains practical due to its non-invasive nature, low cost and wide availability. To improve accuracy in older age groups, especially in disputed or high-stakes cases, integration with advanced techniques such as CBCT and AI is recommended. Hybrid approaches that combine conventional radiographic methods with three-dimensional imaging and data-driven models, along with population-specific validation, are likely to enhance precision and medico-legal reliability.
Overall, the study fulfils its objective by validating the applicability of Kvaal’s method in an Indian adult population while highlighting the need for targeted methodological refinement to meet contemporary forensic demands.
Footnotes
Acknowledgements
I express my gratitude to all my respected professors for their constant support and guidance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
A prior approval was obtained from the Institutional Ethics and Research Committee. (Ref: MDC/DOME/385; dated 22 June 2023).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written informed consent was obtained from all participants prior to enrolment in the study after explaining the purpose and procedures of the research. Confidentiality and anonymity of participant data were strictly maintained throughout the study.