
Abstract
Age estimation plays a vital role in forensic science as it helps in reconstructing the biological profile of a missing person. Cranial suture obliteration is one of the methods used for age estimation. However, the varying accuracy of age assessment through cranial suture obliteration has been found in various populations. The present study aims to generate population-specific regression models by assessing cranial suture obliteration in 3D CT scan images for the estimation of age in the Bengali population of Eastern India using the Acsádi and Nemeskéri method. This study included 221 female and 192 male Bengali individuals of Kolkata, who underwent a 3D CT scan using the DSCT SOMATOM CT scan instrument. Significant correlation (p < .05) found between age and cranial suture obliteration score. 44%–46.2% of estimated age showed higher accuracy (±2.5 years of actual age) in males with age groups of 1–9 years and 50–59 years, when estimated age was calculated through sagittal suture obliteration score. In females, 43.8% of estimated age showed higher accuracy (±2.5 years of actual age) among the age group (40–59 years), when estimated age was calculated through the coronal suture. The Acsádi and Nemeskéri method is an effective method to estimate age in the Bengali population from cranial suture obliteration, with some error due to adaptive response against intrinsic and extrinsic factors.
Introduction
Age estimation holds great importance in forensic science as it helps in identifying individuals along with biological traits such as sex, ancestry and stature. It has a vital role in the identification of missing persons in disasters through matches from databases of missing persons. 1 The estimated age of the deceased person also helps the investigating officer accumulate the sequence of events and circumstances surrounding the case by revealing the time of death. In situations where the alleged offender’s age is in doubt, an accurate assessment of the offender’s age is essential because it affects the legal process and possible outcomes. 2 Forensic scientists, especially forensic anthropologists, use various methods of age estimation, which rely on different biological indicators such as dental eruption, skeletal maturation, and cranial suture fusion.3–6 Acsádi and Nemeskéri method based on combinations of skeletal maturation and skeletal degeneration using four skeletal elements, such as endocranial suture closure, changes in the pubic symphyseal surface, structural changes in the proximal humerus and proximal femur for age estimation. 7 Cranial sutures are the fibrous joints connecting skull bones. It is critical for skull expansion throughout development. 8 Cranial sutures close gradually with age, and this can be indicative of the age range of an individual. However, age is not the only factor that contributes to the closure of sutures. Intrinsic factors like genetics may have an influence on suture closure. The effect of extrinsic or environmental factors has also been evident in suture closure. 9 The conventional evaluation of cranial sutures entails the visual inspection of ecto and endocranial sutures, necessitating the excision of skin, temporal muscles, and epicranial aponeurosis from the cranial bones. 1 3D computerized tomography (CT) scans are better alternatives to evaluate cranial sutures in living and deceased individuals without tissue removal. 10 This method effectively assesses the fusion process of the skull suture with advanced age. 11
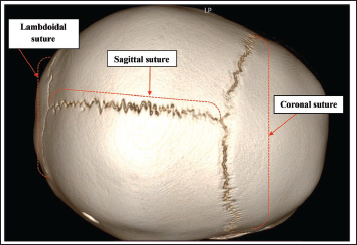
Various studies have already been done on the ectocranial and endocranial skull suture closure with advanced age in different populations, like Thai, 3 Han, 12 Egyptian, 13 and Indian populations. 10 Key cranial sutures like sagittal, coronal, lambdoidal suture have been (Figure 1) used in age estimation. 3 Sagittal suture runs along the mid-sagittal plane and forms the articulation between the right and left parietal bones. The sagittal suture begins to close in the third decade of life and gradually fuses throughout the course of the fourth decade. 3 The coronal suture forms the articulation between the frontal bone and parietal bones. 3 It extends across the skull from one side to the other, forming a transverse line. The coronal suture initiates closure in the third decade of life and typically completes fusion in the fourth decade. Lambdoidal suture forms the articulation between the occipital bone and the parietal bones. 14 The lambdoidal suture typically begins to close in the late twenties with other sutures. Acsádi and Nemeskéri method is used to mark the progress of age by assigning scores based on ectocranial sutural fusion.7, 15, 16 This method has resurrected cranial suture as an accurate indicator of age.12, 15, 17 However, the inaccuracy of age assessment through cranial suture obliteration has been found in various populations due to intrinsic and extrinsic factors. 13 To reduce the inaccuracy of age estimation, population-specific reference standards for age estimation must be required. Therefore, the objective of the study is to generate regression models by assessing cranial suture obliteration in 3D CT scan images for the estimation of age in the Bengali population of Eastern India using Acsádi and Nemeskéri method.
Three-dimensional CT Image of the Skull, Including Suture Closure.
Materials and Methods
The present study was conducted on 413 individuals (221 female and 192 male) of the Bengali population. 3D CT scan images were collected from Bangur Institute of Neurosciences, Kolkata and Apex Club of Bally, Howrah. Data on actual age and sex have been collected from hospital records. Informed consent was obtained from the adult participant prior to data collection. In the case of children, consent was obtained from their parents. Ethical clearance was obtained from the institutional ethical committee. The purposive sampling method was used for selecting the participants, following the inclusion and exclusion criteria.
Inclusion criteria
Participants range in age from a minimum of 1 year to a maximum of 84 years. Patients who underwent a CT scan of the head for diagnostic purposes. Clear CT scan images of the participant’s head.
Exclusion criteria
Blur CT scan images of the participant’s head. Patients with skeletal malformation or deformity, nutritional deficiency, endocrine disorders, skeletal or cranial pathology, or old, healed fractures.
DSCT SOMATOM CT scan instrument was used for scanning. The scanning parameters were 60 slices and an SSAVE type. RadiAnt DICOM Viewer (2024.1) software was used for examining as well as converting a 2D CT image into a 3D CT image using the volume rendering process. After conversion, the resolution of 3D CT images ranged between 210 and 250 pixels per inch. Different views of the skull (norma frontalis, norma lateralis, norma verticalis, norma occipitalis) were examined. Sagittal, coronal and lambdoidal suture obliteration was studied ectocranially by applying Acsádi and Nemeskéri’s (1970) 4-stage scoring system.16, 18
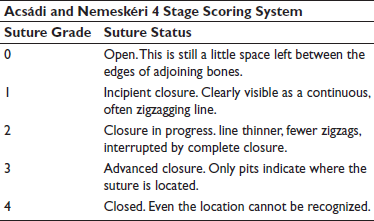
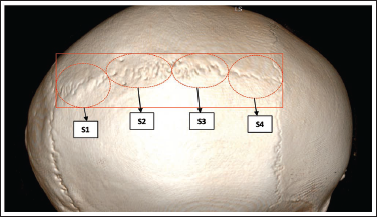
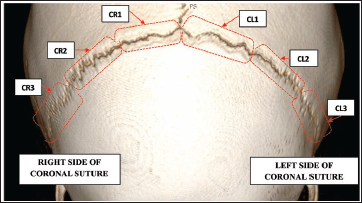
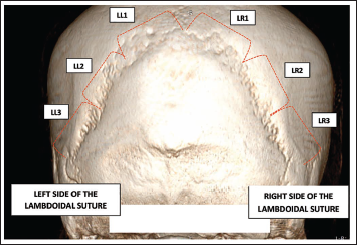
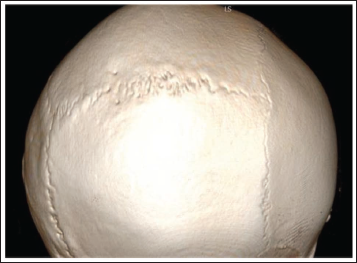
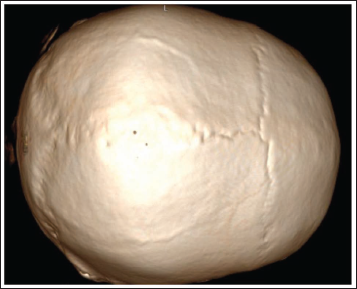
The sutures were divided into three segments: anterior, middle, and posterior. Furthermore, the sagittal suture was divided into four parts: SS1, SS2, SS3, and SS4 (Figure 2). The coronal suture was divided into three parts from the left side of the bregma, CL1, CL2, CL3 and 3 parts from the right side of bregma, CR1, CR2, CR3 (Figure 3). The lambdoidal suture was divided into three parts from the left side of lambda LL1, LL2, LL3 and 3 parts from the right side of lambda LR1, LR2, LR3 (Figure 4). The degree of obliteration was measured by the Acsádi and Nemeskéri 4-stage scoring method 16 (Figures 5–9). The mean score of suture obliteration was calculated by using this formula (sum of segments of suture/total number of segments).
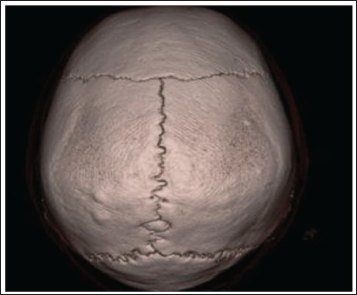
Division of Sagittal Suture (S1, S2, S3, S4). S1: Sagittal Suture Part 1, S2: Sagittal Suture Part 2, S3: Sagittal Suture Part 3, S4: Sagittal Suture Part 4.
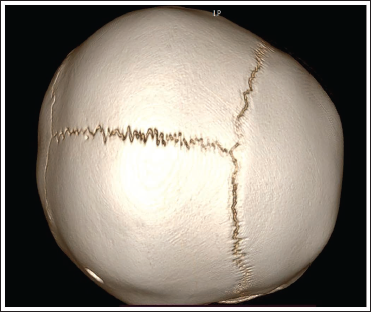
Division of Coronal Suture on the Left Side (CL1, CL2, CL3) and Division of Coronal Suture (CR1, CR2, CR3) on the Right Side. CL1: Coronal Suture Left Side Part 1, CL2: Coronal Suture Left Side Part 2, CL3: Coronal Suture Left Side Part 3, CR1: Coronal Suture Right Side Part 1, CR2: Coronal Suture Right Side Part 2, CR3: Coronal Suture Right Side Part 3.
Division of Lambdoidal Suture on the Left Side (LL1, LL2, LL3) and Division of Lambdoidal Suture (LR1, LR2, LR3) on the Right Side. LL1: Lambdoidal Suture Left Side Part 1, LL2: Lambdoidal Suture Left Side Part 2, LL3: Lambdoidal Suture Left Side Part 3, LR1: Lambdoidal Suture Right Side Part 1, LR2: Lambdoidal Suture Right Side Part 2, LR3: Lambdoidal Suture Right Side Part 3.
Score 0, Open. This Is Still a Little Space Left Between the Edges of Adjoining Bones.
Score 1, Incipient Closure. Clearly Visible as a Continuous, Often Zigzagging Line.
Score 2, Closure in Progress Line Thinner, Less Zigzags, Interrupted by Complete Closure.
Score 3, Advanced Closure. Only Pits Indicate Where the Suture Is Located.
Score 4, Closed. Even Location Cannot Be Recognized. Acsádi and Nemeskéri 4-stage Scoring Method.
Data Analysis
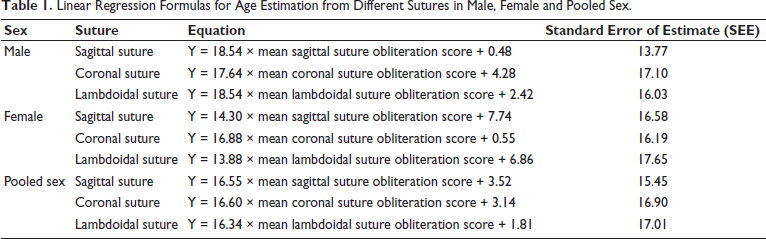
The reliability of measurements was tested among 200 samples for intra- and inter-observer repeatability analysis of the Acsádi and Nemeskéri (1970) method. The same observer examined these skulls one more time after a month had passed since the first examination. Additionally, a different observer performed an inter-observer accuracy test using the same procedure. The analysis of intra- and inter-observer agreements was done using Cohen’s kappa. The Shapiro-Wilk test was performed to check the normality of the variables. Variables were not normally distributed. Non-parametric test (Spearman’s rank correlation) was performed to assess the degree of correlation between age and suture obliteration score. For the male, female, and overall study population, simple linear regression models were developed (Table 1) utilizing the obliteration scores of each of the cranial sutures examined in this study to estimate age. The accuracy of estimated age was evaluated by predicting age falls within ±2.5, ±5, ±7.5, ±10, ±15, ±25, and ±35 years of their actual age. The overall inaccuracy and the overall bias of the complex method were calculated for male, female and pooled sex. Inaccuracy and bias were calculated using the standard formula. 19 All the statistical tests were computed using Statistical Package for the Social Sciences (IBM-SPSS) Statistics version 25.
Linear Regression Formulas for Age Estimation from Different Sutures in Male, Female and Pooled Sex.
Results
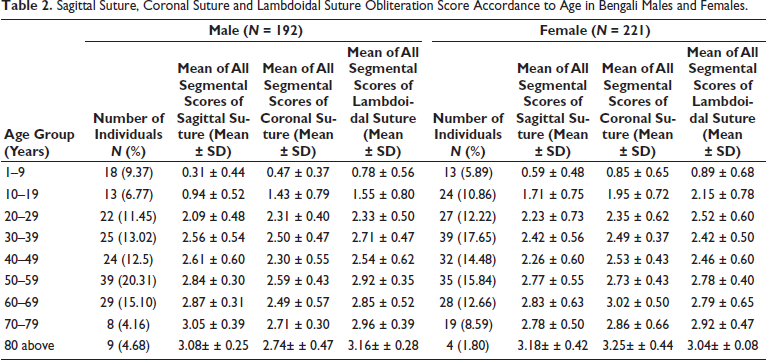
The pattern of ectocranial sagittal, coronal, and lambdoidal suture obliteration accordance to age was observed in Bengali males and females (Table 2). Lambdoidal suture was obliterated faster than coronal and sagittal suture accordance to age in both sexes.
Sagittal Suture, Coronal Suture and Lambdoidal Suture Obliteration Score Accordance to Age in Bengali Males and Females.
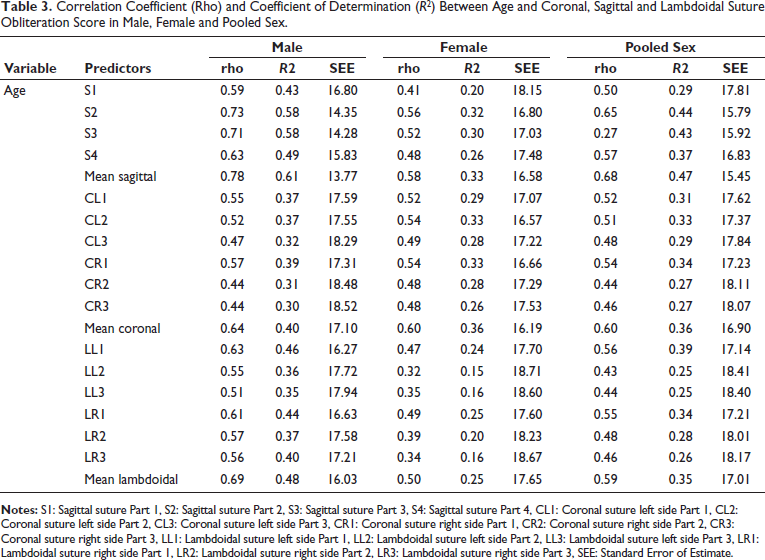
The highest correlation (rho = 0.785, p < .05) was found between age and mean sagittal suture obliteration score in males (Table 3), which was also envisaged best predictor of coefficient of determination (R2 = 0.61). On the other hand, highest correlation was found between age and mean coronal suture obliteration score (rho = 0.607, p < .05) in Females (Table 3), which was also envisaged best predictor of coefficient of determination (R2 = 0.36). Significant correlation was also found (p < .05) between age and mean coronal suture obliteration score (rho = 0.640) (Table 3) and mean lambdoidal suture (rho = 0.693) in males (Table 3). Similarly, significant correlation (p < .05) was found between age and mean sagittal suture obliteration score (rho = 0.582, p < .05) (Table 3) and mean lambdoidal suture obliteration score (r = 0.500, p < .05) in females (Table 3). In case of pooled sex, highest correlation (rho = 0.665, p < .05) was found between age and mean sagittal suture obliteration score and a significant correlation was found between age and mean coronal suture obliteration score (r = 0.516, p < .05) and mean lambdoidal suture obliteration score (r = 0.565, p < .05).
Correlation Coefficient (Rho) and Coefficient of Determination (R2) Between Age and Coronal, Sagittal and Lambdoidal Suture Obliteration Score in Male, Female and Pooled Sex.
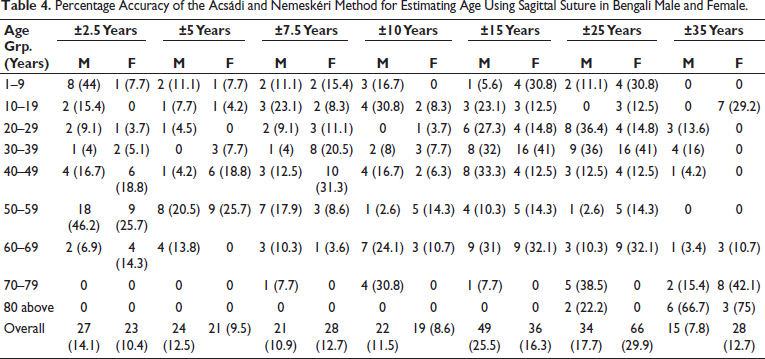
Percentage accuracy of correct age estimation in males and females through the sagittal suture obliteration score is demonstrated in Table 4. Accuracy percentage of estimated age calculated through sagittal suture obliteration was higher in males than in females for overall ages. Accuracy percentage of estimated age was considerably higher in the age group (50–59 years and 1–9 years) among males. In females, accuracy percentage of estimated age was higher in the age groups (50–59 years and 40–49 years).
Percentage Accuracy of the Acsádi and Nemeskéri Method for Estimating Age Using Sagittal Suture in Bengali Male and Female.
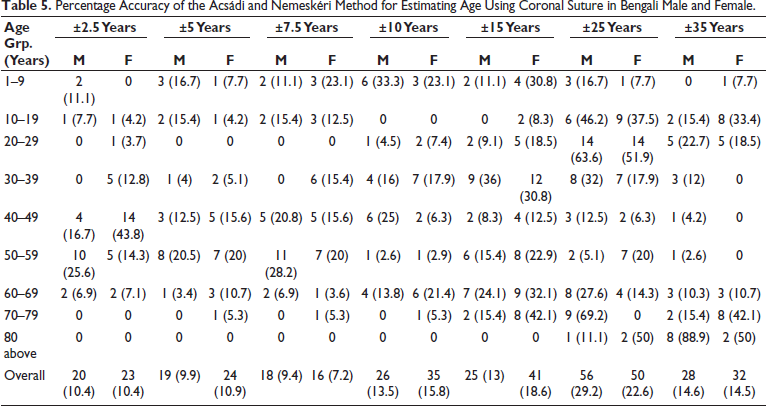
The percentage accuracy of correct age estimation in males and females through coronal suture obliteration score is demonstrated in Table 5. Percentage accuracy of the Ascrdi and Nemeskari method for estimating age using coronal suture in Bengali males and females. Accuracy percentage of estimated age through coronal suture obliteration was higher in females than in males for overall ages. The accuracy percentage of estimated age was considerably higher in age groups (50–59 and 40–49 years above) of both sexes.
Percentage Accuracy of the Acsádi and Nemeskéri Method for Estimating Age Using Coronal Suture in Bengali Male and Female.
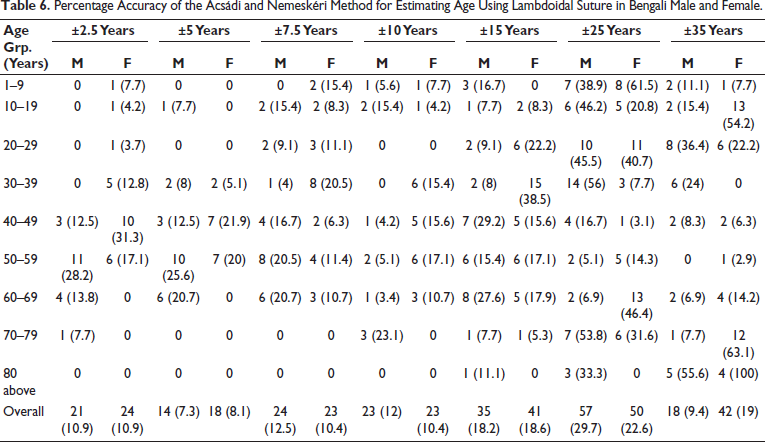
The percentage accuracy of correct age estimation in males and females through the lambdoidal suture obliteration score is demonstrated in Table 6. The accuracy percentage of estimated age through lambdoidal suture obliteration was higher in females than in males for overall ages. The accuracy percentage of estimated age was considerably higher in age groups (50–59 and 60–69 years). In females, accuracy percentage of estimated age was higher in the age groups (40–49 and 50–59 years).
Percentage Accuracy of the Acsádi and Nemeskéri Method for Estimating Age Using Lambdoidal Suture in Bengali Male and Female.
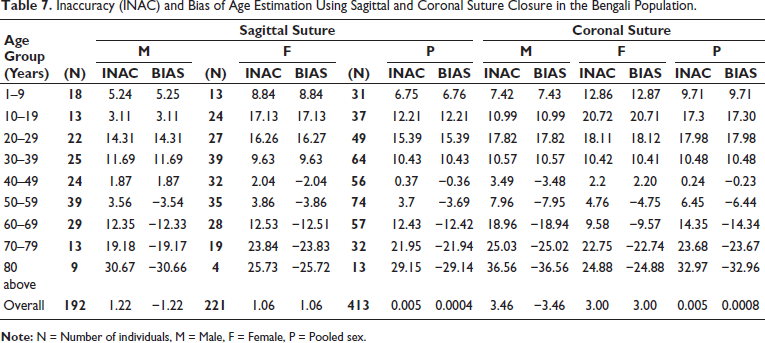
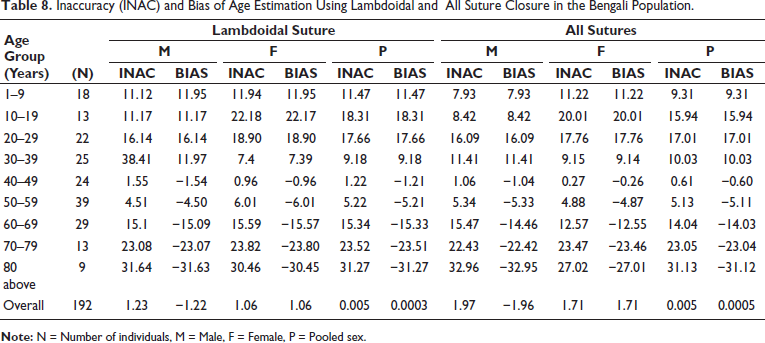
These results were corroborated by the inaccuracy and bias calculated for sagittal suture, coronal suture and lambdoidal suture as well as the sum of all sutures (sagittal, coronal, and lambdoidal sutures) in male, female and pooled sex (Tables 7 and 8). Lowest inaccuracy and bias were obtained in male (inaccuracy = 1.22, bias = −1.22), female (inaccuracy = 1.06, bias = 1.06), when the estimated age was calculated through mean sagittal suture obliteration score. Similar findings were found in male (inaccuracy = 1.23, bias = −1.22) and female (inaccuracy = 1.06, bias = 1.06), when estimated age was calculated through the mean lambdoidal suture obliteration score. On the other hand, highest inaccuracy and bias were found in estimated age calculated through coronal suture among males (inaccuracy = 3.36, bias = −3.46) and females (inaccuracy = 3, bias = 3.00). Inaccuracy and bias were (1.97 and −1.96) in males and (1.71 and 1.71) in females, when estimated age was calculated through sum of all sutures (SS, CS, LS). No inaccuracy and bias were found in pool sex, when estimated age was calculated through mean sagittal, coronal, and lambdoidal sutures and sum of all sutures (SS, CS, LS). Inaccuracy and bias as per age group revealed that the complex method overestimates younger ages and underestimates older ages through sagittal, coronal and lambdoidal suture in male, female and pooled sex. However, the degree of inaccuracy and bias varied between male, female and pooled sex in terms of age group, sagittal suture, coronal suture and lambdoidal suture. Bias values were very minimal in all categories among the age group (40–59 years). Bias was also very less in estimated age calculated through sagittal suture obliteration score among males aged between 1 and 19 years. In contrast, bias was increased in all categories among the age groups (1–39 years) and (60–80 years and above).
Inaccuracy (INAC) and Bias of Age Estimation Using Sagittal and Coronal Suture Closure in the Bengali Population.
Inaccuracy (INAC) and Bias of Age Estimation Using Lambdoidal and All Suture Closure in the Bengali Population.
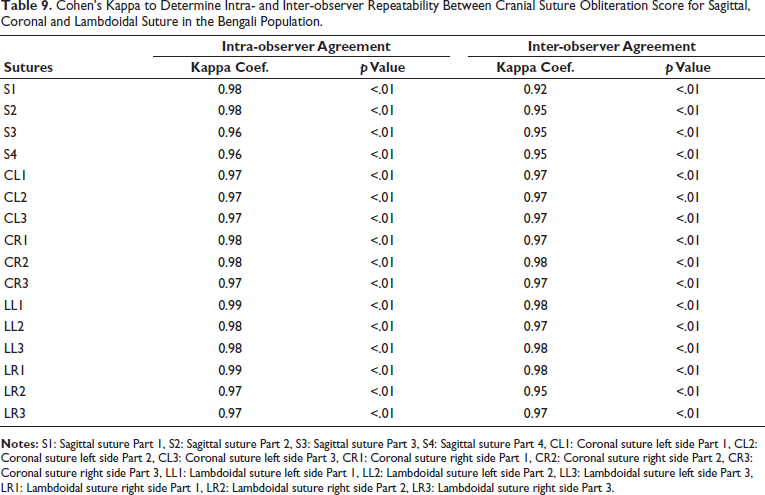
Perfect intra-observer agreement was found for all segments of sagittal suture (Cohen’s kappa S1, S2 = 0.98, S3, S4 = 0.96), coronal suture (Cohen’s kappa CL1, CL2, CL3 = 0.97, CR1, CR2 = 0.98, CR3 = 0.97) and lambdoidal suture (Cohen’s kappa LL1 = 0.99, LL2, LL3 = 0.98, LR1 = 0.99, LR2, LR3 = 0.97) (Table 9). Inter-observer agreement was slightly lower than intra-observer agreement for all segments of sagittal suture (Cohen’s kappa S1 = 0.92, S2, S3, S4 = 0.95), some segments of coronal suture (Cohen’s kappa CR1 = 0.97) and lambdoidal suture (Cohen’s kappa LL1 = 0.98, LL2 = 0.97, LR1 = 0.98, LR2 = 0.95).
Cohen’s Kappa to Determine Intra- and Inter-observer Repeatability Between Cranial Suture Obliteration Score for Sagittal, Coronal and Lambdoidal Suture in the Bengali Population.
Discussion
Cranial suture obliteration is an effective method of age estimation after 21 years of age, when all teeth have erupted, and epiphyses have fused. 20 The degree of cranial suture obliteration was measured by Acsádi and Nemeskéri (1970) by assigning scores. 16 The efficiency and reproducibility of the Acsádi and Nemeskéri method have been questioned by several studies.20–22 The present work tried to estimate the age of living Bengali individuals of Eastern India through ectocranial suture closure in 3D CT scan images of skull using Acsádi and Nemeskéri method and evaluate the accuracy, reproducibility of method. Ascadi and Nemeskéri method requires detailed observation of cranial sutures, which were visualized through high-resolution (210–250 ppi) 3D CT scan images. This imaging approach is used for increased applicability of the Ascadi and Nemseskeri method, where only CT data are available, such as living individuals or forensic cases where remains cannot be disturbed.16, 23 Apart from this, the study population was divided into 10-year age cohorts instead of 5-year age cohorts to improve the accuracy of method.
Studies on cranial suture ossification revealed inconsistent findings about sexual differences as well as different patterns in cranial suture closure.24–28 The pattern of cranial suture closure in Bengali men and women is not in accordance with Negroes and whites suture closure pattern, where the sagittal suture obliterates faster than coronal and lambdoidal suture. 29 Sagittal, coronal, and lambdoidal suture closure occurs more rapidly in Bengali women than in Bengali men until 29 years, which agrees with earlier works in the Chinese population. 1 Bengali men supersede Bengali women in terms of suture closure after 29 years of age. Closure of sutures is influenced by bone metabolism and regulated by osteoblast-osteoclast cooperation. Estrogen is one of the factors affecting bone metabolism. 1 There is a potential role of estrogen level for these gender differences. The estrogen level is relatively lower in males than in females till adulthood. In females, estrogen levels fluctuate throughout the reproductive age (20–40 years) and decline from the late 40s due to menopause.30–32
For age estimation, ectocranial sagittal suture closure is most effective in Bengali males and the pooled sex category. On the other hand, ectocranial coronal suture closure is most effective for estimating age in Bengali Females. Similar findings were observed in the Chinese male population 1 and Egyptian population, 13 where multi-detector CT images of the skull were used for analysis. However, the magnitude of effectiveness of cranial suture closure for estimated age varied in these populations from the studied population. On the contrary, suture closure is not useful to estimate age in both genders of Europeans. 33 Similar findings were reported in other populations like Kannadigas of Karnataka, 34 Northwest Indian population, 29 Hungarian population, 35 and Polish males. 31 The regression formula was deduced from the mean sagittal, coronal and lambdoidal suture obliteration score (Table 1) to estimate age in male, female and pooled sex. Through calculation of bias, the suture obliteration score overestimates age in younger individuals (1–39 years) and underestimates age in older individuals (50 and above) of the Bengali population. The inaccuracy and bias were minimal in the age group of 40–49 years. This finding corroborates earlier studies in the Hungarian population, 35 Thai population 2 and South African population. 15 However, the cutoff points of underestimation and overestimation of age were found to be different2, 15, 35 from the studied population. The error of age estimation through cranial suture closure might be caused by several factors, like genetic, biochemical stress, diet and nutrition, 36 environment and culture, and individual health. 2 msh homeobox 1 (MSX1): rs3821947 genetic polymorphism has a significant association with suture obliteration. 37 Apart from genetic factors, biochemical factors present in calvaria and tensional forces arising in cranial base are responsible for suture regulation. 38 Both factors might affect the rate of suture obliteration accordance to age, which causes inaccuracies in age estimation.
Apart from accuracy, the reproducibility of the Acsádi and Nemeskéri method has been tested through Cohen’s kappa statistics. Perfect intra- and inter-observer agreement was found for obliteration score in all segments of sagittal, coronal and lambdoidal suture.
Conclusion
Age estimation of the Bengali population has been done efficiently through a generated regression model by assessing cranial suture obliteration in 3D CT scan images of the skull using Acsádi and Nemeskéri’s method. Significant correlation was found between age and cranial suture (Sagittal, coronal and lambdoidal) obliteration score. However, the accuracy of age estimation through the regression model was varied in terms of suture, sex and actual age group. Higher accuracy of age estimation was found to be evident in males with actual age groups of (1–9 years and 50–59 years), when the estimated age was calculated through the sagittal suture obliteration score. In females, higher accuracy of age estimation was found to be evident with the actual age group (40–59 years), when estimated age was calculated through coronal suture. Because suture status was the most predictable and least variable in the mentioned age groups. Intermediate ages showed more variability, which reduces accuracy. 39
Therefore, the Acsádi and Nemeskéri method is an effective method to estimate age in the Bengali population from cranial suture obliteration observed in 3D CT scan (210–250 ppi) images of the skull, with some error due to adaptive response against intrinsic and extrinsic factors. This method should be optimized, including the effect of these factors like genetics, tensile forces and muscle stresses.
Limitations
The present study has some limitations due to the use of hospital-based CT scan data, which introduces potential bias and cannot be a general reflection of the mass population. In the results, considering R2 values, only the male sagittal suture is showing >0.6, which can be said to have fair predictive power. The others have R2 between 0.3 and 0.5, showing moderate predictive power. Apart from that, other limitations such as a small number of elderly group participants (more than 80 years old), the absence of external validation and CT slice thickness variability.
Footnotes
Acknowledgements
The authors are grateful to the participants. Authors are also thankful to the Apex Club of Bally for the necessary support.
Data Availability
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The present study was approved by the ethical clearance committee of Institute of Post Graduate Medical Education and Research (Memo No. IPGME&R/IEC/2023/1076).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was obtained from the adult participant prior to data collection. In the case of children, consent was obtained from their parents.