
Abstract
Age estimation is a critical aspect of forensic identification, particularly in adults, where traditional skeletal markers become less reliable. Cranial suture closure, though controversial, remains a valuable parameter, especially when population-specific standards are applied. This study aimed to assess the correlation between cranial suture closure and chronological age in the Gujarati population. A descriptive cross-sectional study was conducted on 100 medicolegal autopsy cases (50 males, 50 females) aged 13–78 years. Suture closure was assessed using the Acsadi-Nemeskeri scoring system across 16 defined cranial segments. Both endocranial and ectocranial surfaces were examined. In this study, Sagittal sutures closed earliest (30s), followed by coronal (40s), and lambdoid (50+), with near-complete fusion by 60 years. Endocranial closure demonstrated slightly higher accuracy (85%, MAE ± 4.2 years) compared to ectocranial (81%, MAE ± 4.8 years). Correlation with age was strongest for endocranial sagittal sutures (r = 0.946). No significant gender differences were observed. The findings indicate cranial suture closure, particularly endocranial sagittal fusion, is a reliable, gender-independent method for age estimation in the Gujarati population. It is most accurate in individuals aged 30–60 years and should be incorporated into forensic protocols alongside other age indicators.
Introduction
In forensic medicine, accurate age estimation plays a pivotal role in both civil and criminal contexts. From identifying unknown individuals in mass disasters or homicides to determining legal age in judicial proceedings, age estimation is fundamental to forensic identity. Among adults, traditional biological indicators of age, such as dentition or epiphyseal fusion, become less reliable after full skeletal maturity. Therefore, researchers have continuously investigated cranial sutures as a potential age marker, particularly in older adults. 1
The cranial sutures—fibrous joints connecting the bones of the skull—undergo a progressive closure process with age. This closure occurs as part of the natural remodeling and ossification processes of the skeleton, although it can be influenced by various biological, genetic, and environmental factors. As first noted by Krogman et al. 2 (1978), the fusion of cranial sutures follows a predictable endocranial-to-ectocranial pattern, beginning at the internal surfaces of the cranial vault and proceeding outward. 3 The major cranial sutures—sagittal, coronal, and lambdoid—have been extensively studied for their potential as age estimation tools, with researchers attempting to establish reliable correlations between suture closure patterns and chronological age. Despite being widely researched, cranial suture closure remains one of the most controversial indicators of adult age estimation. Studies dating back to the 19th century sought to classify closure sequences and timelines. 2
The challenge of establishing population-specific data for cranial suture closure has been recognized in multiple studies. The Indian subcontinent presents unique challenges for age estimation due to its diverse population genetics, environmental factors, and socioeconomic conditions. Kumar et al. 4 (2012) studied 70 autopsy cases aged 21–50 years and concluded that while endocranial fusion begins as early as 21–30 years, the correlation between suture closure and age is unreliable, making it unsuitable as a standalone parameter for age estimation. Oza et al. 5 (2019) examined 150 cases from Gujarat and found significant correlations between age and suture closure in the 21–40 year age group, with endocranial closure serving as a more reliable parameter than ectocranial examination. Parmar et al. 6 (2012) studied 220 cases aged 15–70 years and found that sagittal suture closure occurred between 50 and 60 years, with earlier closure in males than females.
The state of Gujarat, located in western India, represents a unique demographic and genetic population that may exhibit distinct patterns of cranial suture closure. The need for population-specific data for forensic age estimation has been emphasized in multiple studies, as genetic, environmental, and nutritional factors can significantly influence bone development and suture closure patterns. Understanding these regional variations is crucial for developing accurate forensic methodologies applicable to the local population.
Methodological considerations have evolved significantly in recent years, with the Acsadi-Nemeskeri scale becoming the standard for assessing suture closure. This scale grades closure from 0 (open) to 4 (completely closed) and allows for systematic comparison across studies. However, the interpretation of closure grades and their correlation with age remains challenging due to individual variations and the influence of factors such as sex, genetics, and environmental conditions. 4
This study investigates cranial suture closure in the native Gujarati population through autopsy cases, correlating endocranial and ectocranial suture closure with chronological age.
Aims and Objectives
To assess the correlation between cranial suture closure and chronological age in individuals from Gujarat.
To compare endocranial and ectocranial closure patterns in sagittal, coronal, and lambdoid sutures.
To evaluate sex differences, if any, in suture fusion.
To analyze if cranial suture closure can be used as a reliable parameter for age estimation.
Materials and Methods
Study Design and Setting
This descriptive cross-sectional study was conducted at the Department of Forensic Medicine and Toxicology, Tertiary care center, Ahmedabad, Gujarat, during the period from July 2021 to July 2022. The study population comprised individuals undergoing medicolegal post-mortem examination at the institute. The procedures were conducted in accordance with the ethical standards of the committee and with the 1964 Helsinki Declaration and its later amendments. Written informed consent for the use of research data was obtained from the next of kin.
Sample Size
Sample size was calculated using the correlation formula,
with Zα/2 = 1.96 (95% CI), Z(1–β) = 1.28 (90% power), and assumed correlation (r) = 0.50, yielding 35 participants. To account for nonresponse and withdrawals, the sample was inflated by 10%. Thus, a minimum of 38 cases was required, but we included 100 medicolegal autopsy cases aged between 13 and 78 years to enhance the reliability and validity of the results. The sample was equally distributed between males (50 cases) and females (50 cases).
Inclusion criteria:
Cases undergoing medicolegal post-mortem examination. Cases of known age confirmed through official documents in accordance with the Juvenile Justice Act, 2015. Priority was given to documentary evidence such as birth certificates, matriculation certificates, hospital records, and school admission forms. Aadhaar card details were cross-checked, but not considered the sole authentic proof.
Exclusion criteria:
Unknown or unclaimed bodies where the exact age could not be confirmed. Cases with deformed, diseased, or fractured skulls that might interfere with suture examination. Cases with pathological conditions affecting bone development.
Age Verification
The age of each individual was confirmed through official documents, including birth certificates, service records, driving licenses, passports, ration cards, or voter identification cards, to ensure accuracy of chronological age data.
Examination Protocol
After reflection of the scalp using standard autopsy techniques, the coronal, sagittal, and lambdoid sutures were examined both endocranially and ectocranially. The calvaria was removed using a craniotome, taking care to preserve the complete suture patterns for accurate assessment.
Suture Assessment Method
The degree of suture closure was evaluated using the Acsadi-Nemeskeri complex method, which provides a standardized scoring system
4
:
Grade 0: Open—visible space remains between adjoining bone edges. Grade 1: Incipient closure—continuous, often zigzagging line clearly visible. Grade 2: Closure in process—thinner line with fewer zigzags, interrupted by areas of complete closure. Grade 3: Advanced closure—only pits indicate suture location. Grade 4: Closed—suture location no longer recognizable.
Suture Segmentation
Each suture was divided into standardized segments for detailed analysis:
Sagittal suture: Divided into four equal segments. Coronal suture: Examined in three segments each on the right and left sides (a total of six segments). Lambdoid suture: Studied in three segments, each on the right and left sides (a total of six segments).
This segmentation allowed for a total of 16 measurement points across the three major cranial sutures, providing comprehensive coverage of suture closure patterns.
Statistical Analysis
Data were analyzed using SPSS Statistics Version 20. Descriptive statistics (median) were calculated for age and suture scores. Pearson’s correlation (r) assessed the relationship between chronological age and suture closure, with p < .05 considered significant. One-way ANOVA tested differences in closure across age groups, while independent t-tests and chi-square tests evaluated gender differences. A multiple linear regression model predicted age based on ectocranial and endocranial scores, with model performance measured by R², mean absolute error (MAE), and standard error.
Results
Age and Gender Distribution
A total of 100 medicolegal autopsy cases were analyzed. The study participants ranged in age from 13 to 78 years. The highest number of cases (25%) belonged to the 30–39 age group, followed by the 20–29 group (23%). The mean age was 37.2 ± 15.1 years. Out of 100, 50 were males (Table 1).
Ectocranial Suture Closure Patterns by Age and Gender.
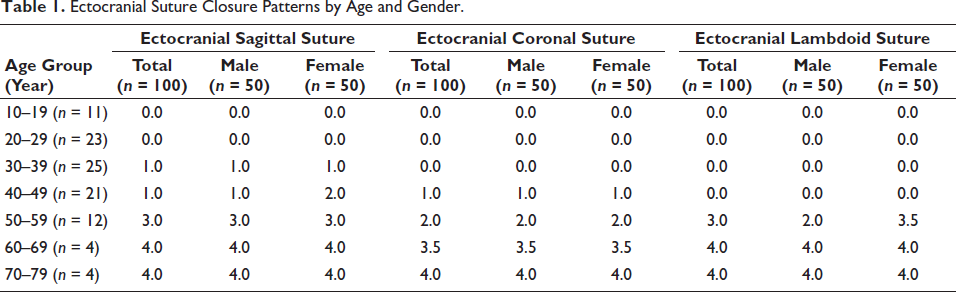
Sagittal suture closure begins in the 30–39 age group and progresses significantly by the 50s, with near-complete fusion by age 60. While early and mid-life fusion shows minimal gender differences, females exhibit slightly more closure in their 40s. Coronal sutures show delayed closure, first appearing in the 40–49 group and accelerating in the 50s, reaching near-complete fusion by 60–69 years. No notable sex-related differences are observed. Lamboid sutures display the latest onset, with closure initiating after age 50. Fusion is generally complete by 60+, and females tend to fuse earlier than males in this region. Overall, sagittal sutures close first, followed by coronal and then lamboid. Closure scores correlate strongly with age, and although sex differences are minor, females tend to fuse slightly earlier. Suture closure is minimal before 40, making it most reliable for age estimation in middle to older adults (Table 1).
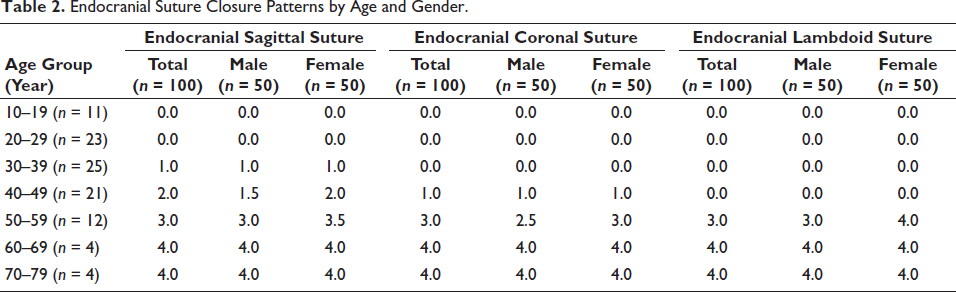
Sagittal suture closure begins in the 30s, progressing steadily through the 40s and 50s, with females showing slightly earlier fusion. By age 60, complete closure (Score 4.0) is seen in both sexes. Coronal closure starts later, appearing in the 40–49 group and increasing rapidly in the 50s, again with females slightly ahead. Full fusion is observed in all individuals by age 60. Lamboid sutures remain open until after 40, then fuse sharply in the 50s, with females showing more complete closure. From age 60 onward, fusion is complete and consistent across both sexes. Overall, sagittal sutures close first, followed by coronal and lamboid. Closure correlates strongly with age, especially after 50, and occurs slightly earlier in females. Endocranial closure is rare before 40, making it most valuable for age estimation in older adults (Table 2).
Endocranial Suture Closure Patterns by Age and Gender.
Endocranial sagittal sutures had the highest correlation (r = 0.946), making them the most reliable for age estimation. Coronal sutures showed similar reliability on both surfaces (r ≈ 0.88), while lambdoid sutures had the lowest but still strong correlations (r ≈ 0.83). Overall, endocranial surfaces offered slightly better predictive value than ectocranial (Table 3).
Correlation of Suture Closure with Chronological Age by Suture Type and Surface.

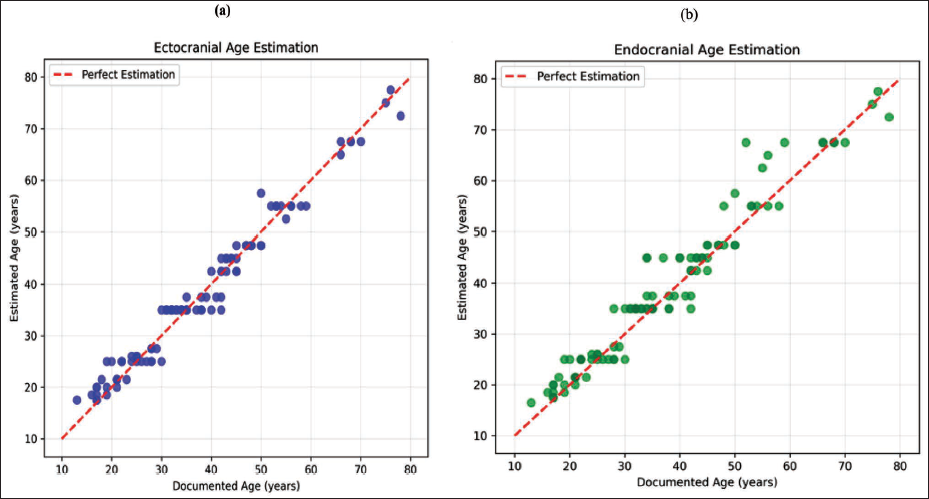
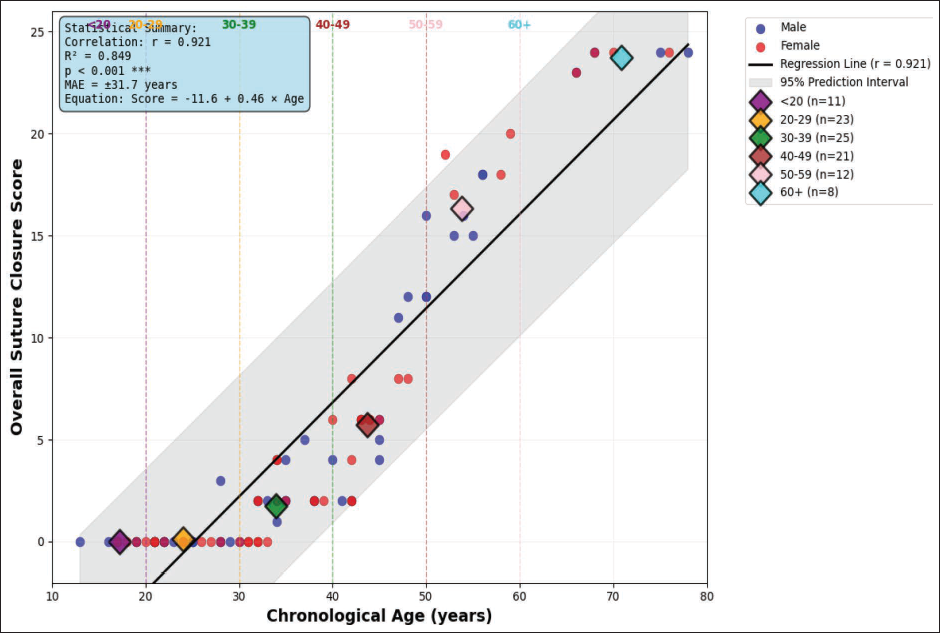
The analysis demonstrates a very strong positive correlation between documented age and estimated age by closure of both endocranial and ectocranial sutures (r = 0.921 and r = 0.916, respectively, p < .001 for both) (Figure 1).
Correlation Between Documented Age and Estimated Age by (a) Ectocranial Suture Closure and (b) Endocranial Suture Closure.
ANOVA results demonstrate statistically significant age-related differences across all sutures, with the sagittal suture showing the strongest association (F = 89.45, p < .001), followed by the coronal (F = 67.23) and lambdoid (F = 54.12). These findings confirm that each suture contributes meaningfully to age estimation (Table 4).
ANOVA Analysis of Suture Closure.

Endocranial sutures show a more consistent and reliable pattern of closure compared to ectocranial sutures. Endocranial suture closure proved more accurate, with 85% of cases within range, 78% within ± 5 years, and a lower MAE of 4.2 years. Ectocranial closure showed slightly lower accuracy (81% within range, 74% within ± 5 years) and a higher MAE of 4.8 years. Endocranial estimation shows slightly lower error and variability, making it more precise. The MAE under 5 years suggests that both methods are forensically acceptable for adult age estimation (Table 5).
Comparison of Accuracy Metrics for Ectocranial and Endocranial Age Estimation.

The regression model further reinforces this relationship, explaining 84.9% of the variance in age (R² = 0.849), with a MAE of ± 4.91 years. Among the evaluated features, the sagittal suture emerged as the most influential predictor, highlighting its critical role in age estimation models (Table 6).
Regression Analysis of Suture Closure.

Gender Analysis of Suture Closure Patterns
The analysis found no significant gender differences in cranial suture closure patterns. Accuracy rates were comparable between sexes, with endocranial estimation slightly more accurate in both males (83.3%) and females (85.1%). Ectocranial accuracy was similar for males (81.4%) and females (80.9%). These findings indicate that gender-specific adjustments are not required, and the same age estimation approach can be reliably applied to both gender (Figure 2).
Regression Analysis of Suture Closure.
Discussion
This cross-sectional study was conducted on 100 medicolegal autopsy cases (50 males, 50 females) aged 13–78 years in the Gujarat population.
Chronological Patterns of Suture Closure
Our study reveals that cranial suture closure follows a predictable chronological sequence, with sagittal sutures beginning closure in the 30s, followed by coronal in the 40s, and lambdoid after 50. This pattern aligns with findings by Bhaurao Parchake et al. 7 (2015) from Nagpur, who reported that early sagittal suture closure began at 20–29 years and reached near-complete closure by 50–59 years. Parmar et al. 6 (2012) documented sagittal suture closure in the 50–60 year range, coronal at 50–60 years, and lambdoid at 45–55 years in their study of 220 cases, which closely parallels our findings. However, their study showed slightly earlier lambdoid closure compared to our results. Bhise et al. (2016) also reported a similar sequence of endocranial closure, beginning with the sagittal suture. 8
Endocranial Versus Ectocranial Closure Patterns
Our study confirms the greater reliability of endocranial suture closure for age estimation, with higher accuracy (85%) and lower MAE (4.2 years) compared to ectocranial closure (81%, MAE 4.8 years). This supports findings by Oza et al. 5 (2019) who noted earlier and more regular endocranial fusion, with endocranial fusion beginning as early as 32 years for the sagittal suture compared to 35 years ectocranially. Kumar et al. 4 (2012) reported endocranial closure observable as early as 21 years for coronal sutures. This inconsistency may be attributed to the outer skull’s exposure to mechanical stress, trauma, and environmental factors. 9 Gaur et al. 10 (2007) established that endocranial closure provides more reliable age estimation parameters, while Singh et al. 11 (2004) confirmed through CT analysis that endocranial fusion occurs more uniformly and predictably than ectocranial fusion in Indian populations.
Statistical Reliability and Correlation Strength
The strong correlations observed in our study (r = 0.946 for endocranial sagittal, r = 0.884 for coronal, r = 0.830 for lambdoid) demonstrate robust age-related closure patterns. These correlations are notably higher than those reported in many Western studies, possibly reflecting population-specific genetic or environmental factors affecting suture closure in the Indian population. A recent 3D CT study of 263 Indian adults found correlations ranging from 0.499 to 0.512 for different suture segments, with standard errors of 13.27–15.08 years. While their error rates are higher than our MAE of 4.2–4.8 years. 12
Gender Differences in Suture Closure
Our study found minimal gender differences in suture closure patterns, with comparable accuracy in males (83.3%) and females (85.1%). This aligns with Perizonius et al. 13 (1984), who also found no notable sex-related differences in closure timing. While Sahni et al. 14 (2005), Parmar et al. 6 (2012) and Verma et al. 15 (2010) reported earlier closure in males, while Oza et al. 5 (2019) observed earlier closure in females. These inconsistencies suggest that gender-related closure patterns may vary by population, highlighting the need for further region-specific research. The role of hormonal influences on suture closure, particularly estrogen’s effects on bone metabolism, requires further investigation in the Gujarat population.
Methodological Considerations
While some studies question the reliability of cranial sutures for age estimation, our findings highlight the value of assessing predictable partial closure, particularly on the endocranial surface. Soliman et al. 16 (2023) found complete fusion to be rare, even in old age, reinforcing the need to distinguish it from partial closure, which our study shows follows a clear chronological pattern. Despite criticism of variability and inaccuracy in past research, literature reviews consistently acknowledge that endocranial sutures offer greater reliability, aligning with our results.
Population-specific Variations
The variability in suture closure across populations highlights the importance of developing region-specific reference data. While Kumar et al. 4 (2012) found no clear age-closure correlation in a Karnataka population, our Gujarat-based study shows more consistent and predictable patterns, possibly due to regional genetic or environmental factors. This emphasizes the need for localized standards in forensic age estimation.
Technological Advancements
Recent literature highlights the growing role of CT imaging in forensic suture analysis, offering greater precision and visualization than traditional autopsy methods. Although our study used conventional techniques, future research should explore CT-based assessments in the Gujarat population to validate and potentially enhance age estimation accuracy. 17
Limitations
The modest sample size, cross-sectional design, and uneven age distribution, particularly in older groups, may affect generalizability of findings. Additionally, our age range of 13–78 years may not fully capture closure trends in advanced age. Soliman et al. 16 included participants over 100 years old and found that many sutures remain partially open, even in old age. Despite using standardized criteria, the subjective nature of suture scoring introduces potential observer bias, which could be minimized through inter-observer reliability testing. Additionally, environmental and genetic influences on suture closure were not examined, which may explain some of the observed individual and regional variations.
Conclusion
This study provides compelling evidence that cranial suture closure is a reliable, gender-independent method for age estimation in the Gujarat population. The endocranial sagittal suture is the most reliable primary indicator for age estimation due to its strong correlation with chronological age. Coronal sutures serve as effective secondary indicators, providing additional confirmation. Both endocranial and ectocranial methods are proven reliable, with optimal accuracy observed in the 30–60 years age group, where suture closure is most progressive. As no significant gender differences were found, a unified protocol can be applied to both males and females, simplifying forensic application.
For future research, it is recommended to: (a) Expand the sample size to strengthen statistical significance, (b) Include additional sutures such as metopic and occipital, (c) Validate the method across other regional populations in India, and (d) Integrate with other skeletal or dental indicators to enhance overall accuracy in forensic casework.
Footnotes
Abbreviations
ANOVA: Analysis of Variance
CT: Computed Tomography
IRB: Institutional Review Board
MAE: Mean Absolute Error
r: Pearson correlation coefficient
SPSS: Statistical Package for Social Sciences
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Ethics Committee of Smt. N.H.L. Municipal Medical College, Ahmedabad.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent for the use of research data was obtained from the next of kin.